
Abstract

Significance statement
Endotracheal intubation may result in injury to the hypopharynx, larynx, and trachea, leading to granuloma formation. Postintubation granuloma of the larynx-hypopharynx is an uncommon cause of airway obstruction and stridor, especially in infants. Only one case of postintubation laryngeal granuloma in infants causing stridor has been previously described in the literature. We present the first clinical report of postintubation granuloma of the hypopharynx in an infant, treated successfully with endoscopic resection.
A 4-month-old female was referred to our ear, nose, and throat (ENT) department with a 1-month history of progressive inspiratory stridor, respiratory distress, and feeding problems. She was born by cesarean section due to twin pregnancy (27 weeks) and premature onset of delivery, weighed 700g, and APGAR scores were 5 at 1 minute and 6 at 5 minutes. Immediately after birth, the neonate was intubated and transferred to neonatal intensive care unit for further diagnosis and treatment. The neonate diagnosed with patent ductus arteriosus, on the 1st day of life, was successfully restored with surgery at 58th day. She was also diagnosed with nenonatal respiratory distress syndrom type 2 and bronchopulmonary dysplasia. During her hospitalization, the patient suffered from two episodes of sepsis by staphylococci aureus, controlled effectively with medications.
The patient was intubated three times (9 days of intubation in total) during her 3-month hospitalization. After the third extubation, she developed a progressive inspiratory stridor. Flexible fiberoptic laryngoscopy revealed a pedunculated mass (1.9 x 1.6 x 0.8 cm in size) at the posterior wall of hypopharynx (Figure 1A). The mass was prolapsing into the airway and was obstructing 100% of the glottic aperture during inspiration (Figure 1B). An endoscopic resection of the mass, en block with its pedicle, under general anesthesia was performed, using bipolar diathermy and 0o 4 mm endoscope. The patient had an uneventful recovery with immediate relief of upper airway obstruction symptoms (Figure 1C). Intraoperative endoscopic images: A—showing the granuloma (G) arising from hypopharynx; B—causing obstruction of the glottis, in contact with epiglottis (E), during inspiration; and C—after the resection of the granuloma.
Histopathologic examination revealed inflammatory reaction with ulcer and granulomatous tissue in the hypopharynx (Figure 2). The child remains asymptomatic and with no signs of recurrence 1 year after surgery. Histopathological examination showing inflammatory reaction with ulcer and granuloma (H&E, X40). H&E, hematoxylin and eosin.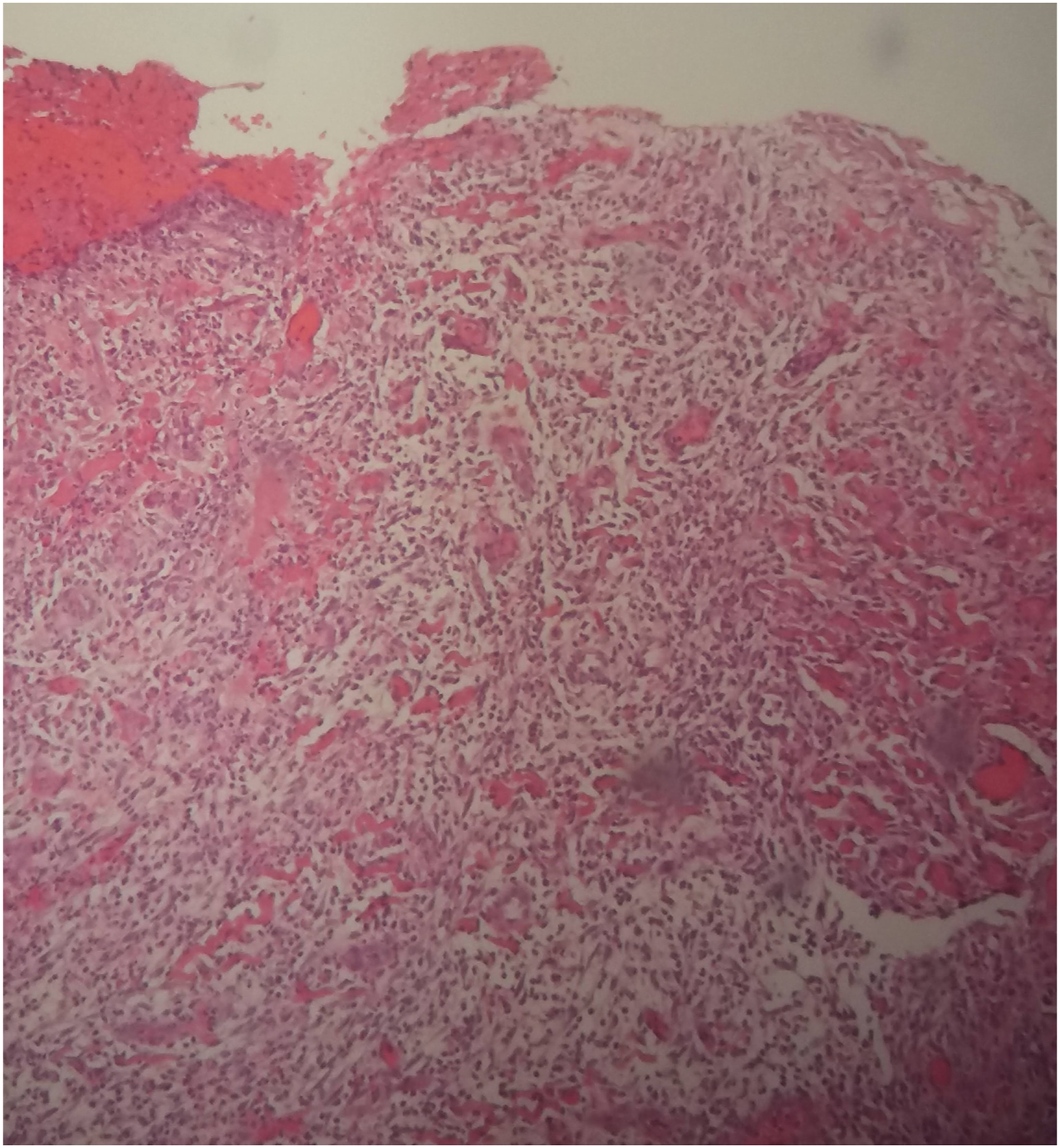
In the neonatal and infant period, inspiratory stridor is a common symptom that intimates airway obstruction and requires immediate assesment. 1 At this age, the differential diagnosis of stridor includes congenital lesions such as laryngomalacia, cardiovascular anomalies and vocal cord paralysis. 2 Masses of head and neck and trauma are unusual causes of neonatal and infant stridor. 1 Postintubation laryngeal granulomas are extremely rare in infants and children because of the higher position and tapered shape of their larynx, which can displace mechanical traumatic forces of the endotracheal tube away from the posterior glottis and toward to the subglottic region.2-4
In 1932, Claussen 5 was the first who described postintubation granulomas. In most cases, they develop in patients after a long period of intubation, but they can also being developed after a shorter period of time. 6 A variety of risks factors for postintubation complications have been described such as inappropriate size of tube, duration of intubation, position of the patient, abnormal laryngeal anatomy, and multiple intubations.2,4,7 The incidence of postintubation laryngeal granulomas varies from 1 per 800 to 1000 intubations.2,3,5 To our knowledge, only one clinical report of postintubation laryngeal granulomas in infants has been previously described in the literature. 4 This is the 2nd case of postintubation granuloma in an infant causing stridor, and the first arising from hypopharynx.
Postintubation laryngeal granuloma’s pathogenesis includes mucosal injury and secondary perichondritis.2,3,8 This area may develop secondary infection and ulceration.2,3,8 The ulcerated area attempts to heal and is often covered with epithelium.4-6 Ultimately, a pedunculated granular tissue is formed.2,3,8 The most common position of granulomas in childhood is the subglottic laryngeal area. 4 In contrast to children, the most common location of postintubation granulomas in adults is along the posterior aspect of the vocal cords in the region of the vocal process of the arytenoid cartilage or, less commonly, at the posterior cricoid plate. 4 In our case, we suggest a mechanical injury of mucosal and the underlying fascia and muscles.
In the literature, there is no consensus for the treatment of granulomas of the larynx area. Inhaled steroids and proton pump inhibitors may be effective of the treatment of non-specific granulomas. 6 Surgical excision with microlaryngeal instruments or with the CO2 laser preferred for the treatment of postintubation lesions, causing airway obstruction or suspected for malignancy.2,6 Postoperatively, a close follow-up is required as these lesions tend to recur.2,6
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed consent
We declare that written informed consent for patient information and images to be published was provided by the patient.