
Abstract
Objective
Body dysmorphic disorder (BDD) represents a bridge between the fields of psychiatry and cosmetic surgery. It is a psychiatric disorder involving altered body image and has been associated with cosmetic surgery. Many studies have investigated BDD following rhinoplasty. However, their findings were inconsistent, which prompted us to conduct this systematic review to obtain strong evidence about the prevalence of BDD among rhinoplasty candidates.
Methods
We searched the literature using electronic databases such as PubMed, Scopus, Web of Science, and others using keywords relevant to the study outcomes. We also manually examined the references of the included studies and relevant reviews to look for articles that might have been missed during the electronic search.
Results
Nine articles met the inclusion criteria. We identified 7 other relevant articles; since they had been included in a review conducted in 2016, they were not included in the final list of articles. However, they were included in the discussion, and their findings have been compared with ours. The included articles resulted in a total sample of 712 rhinoplasty candidates. The estimated prevalence rates of BDD in these articles ranged from 22% to 52%, which was considered high by all the authors of the included studies.
Conclusion
The prevalence of BDD among rhinoplasty candidates is high, and adequate management and interventions are needed to reduce it.
Introduction
A culture of undergoing procedures for altering facial esthetics to achieve Western standards of beauty has been noted, especially among individuals residing in low-to middle-income countries.1,2 It is believed that one should have an attractive pattern of facial characteristics to achieve the highest degree of beauty. Among the different parts of the face, the nose holds significant esthetic value and represents a common cause of dissatisfaction among various populations.1,2 Accordingly, estimates show that rhinoplasty is one of the most common esthetic surgeries among various populations, and individuals aged between 13 and 34 years usually undergo rhinoplasty to achieve a favorable cosmetic appearance.3-5 It has also been reported that adolescents of ethnicities characterized by large noses and those with body dysmorphic disorders (BDD) are the ideal candidates for this procedure,3-10 highlighting the social importance of this procedure.1,5,6,8,9,11,12
BDD has been considered a bridge between the fields of psychiatry and cosmetic surgery; it represents psychiatric disorders related to altered body image and has been associated with cosmetic surgery.3,4 Plastic surgeons and other clinicians have previously demonstrated that it is difficult to identify BDD in the clinical setting. Moreover, mental health specialists have demonstrated that BDD is underdiagnosed.4,13 The management of BDD is complex; many patients believe that it only requires physical interventions, whereas experts indicate that although the problem arises from a physical defect, the mentality of the affected individual is key to the development of BDD, and these individuals therefore require psychological or psychiatric treatment. 3
Patients with BDD mainly experience psychological problems due to their perception of their body. The symmetry, attractiveness, and perfection of the target body part are important determinants of surgical success and are also risk factors for developing BDD.14,15 Many studies have assessed the prevalence and associated factors of BDD in patients undergoing rhinoplasty. Veale et al. conducted a systematic review of 7 studies on this topic in 2016 16 and reported that the prevalence of BDD among patients who underwent rhinoplasty was 20.1%. Many investigations have been published subsequently, with variable prevalence rates and updates on the associated risk factors. Accordingly, this systematic review aims to collate and update the current evidence regarding the prevalence of BDD in rhinoplasty candidates.
Patients and Methods
Inclusion and Exclusion Criteria
The main study outcome was the current prevalence of BDD among rhinoplasty candidates. Accordingly, studies were included if they were: (1) on patients who were indicated for cosmetic rhinoplastic surgeries; (2) cross-sectional investigations, as they are the most suitable for assessing the prevalence of BDD in rhinoplasty candidates; and (3) included an adequate definition of BDD in the methodology. Studies from across the globe on patients from all age groups were included. Studies were excluded if they (1) were on an unrelated topic, did not assess the outcome of interest, assessed the prevalence of BDD in patients undergoing cosmetic surgeries other than rhinoplasty, or assessed the prevalence of BDD in patients undergoing functional rhinoplasty; (2) had an unoriginal design; (3) were published outside the search timeline; and (4) were case reports, letters, editorials, commentary, discussion, protocols, and theses.
Search Strategy
This study followed the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines. 17 To formulate a well-constructed search strategy for retrieving all relevant studies and gathering current evidence, to increase the value of our evidence, and to avoid missing any potentially relevant studies, we conducted both manual and electronic searches. The manual search was conducted within the references of the included studies and current relevant reviews. The electronic search was conducted to retrieve all relevant studies from Medline within the following databases: PubMed, Scopus, Google Scholar, Web of Science, Excerpta Medica DataBASE, and the Virtual Health Library maintained by the World Health Organization. The following search terms, modified based on the database, were used: (rhinoplasty OR septorhinoplasty) AND (Body dysmorphic disorder OR dysmorphic OR dysmorphobias OR dysmorphia.
Screening and Data Extraction
The reports identified through the literature search were screened in 2 steps according to the outcomes of interest and inclusion and exclusion criteria. First, we systematically screened the title and abstract of each identified study, with each investigator being blinded to the decisions of the others. Next, the final decisions of the investigators were compared, and a final decision that all members agreed on was obtained through public discussion under the supervision of a senior investigator. Full-text screening was performed similarly. To facilitate screening and prevent potential overlap among the included studies, all articles were numbered consecutively until the data extraction stage. Furthermore, to facilitate identification and screening, the relevant data of all articles, including title, authors, digital object identifier, journal, uniform resource locator, and abstract, were inserted into an Excel sheet. After creating the final list of articles, a standardized extraction sheet was designed based on the outcomes of interest, and it was divided into 3 tabs, including the baseline characteristics of the participants of each study, study population and outcomes, and domains of the quality assessment tool.
Quality Assessment
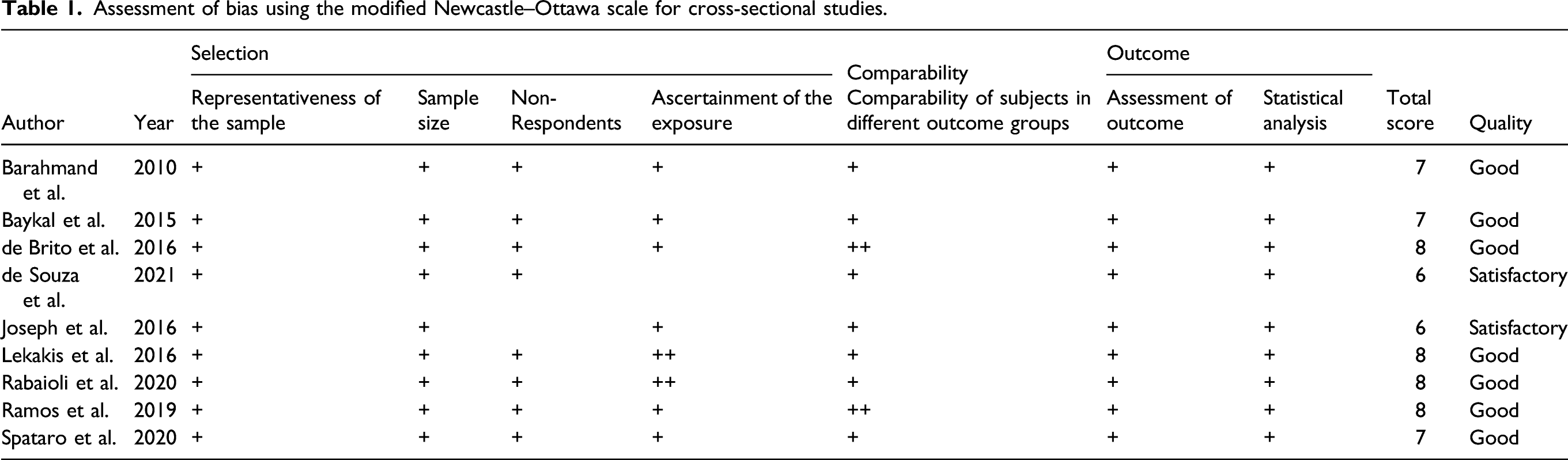
Since we only included cross-sectional studies, we used the modified Newcastle–Ottawa scale (NOS) for cross-sectional studies for quality assessment. 18 It consists of 3 major domains designed to assess the quality of a study’s methods, assessment and compatibility, and reporting of outcomes. Studies were given scores for each domain and classified into non-satisfactory, satisfactory, good, or excellent based on the total score, which ranged from 0 (indicating a high degree of bias) to 10 (indicating no bias).
Results
Search Results
The flow diagram of the search strategy, study selection, and reasons for excluding studies is presented in Figure 1. Briefly, we retrieved 2214 citations from all the databases, of which 846 duplicates were excluded using Endnote. The remaining articles underwent title and abstract screening followed by full-text screening, which yielded 8 relevant articles, in addition to one article that was identified by manual searching, resulting in a total of 9 included studies. The final list of included studies was comprised of more than 9 studies, but we excluded 7 studies1,3,9,19-22 that had been included in a meta-analysis published in 2016
16
; we thought it better to exclude these articles and only reported the weighted overall prevalence rate estimated in their analysis in our discussion. We also included one article that had not been included in the meta-analysis, although it was published in 2010,
23
because we believed we would be able to retrieve relevant information from this article. Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) flow diagram of the search strategy for retrieving relevant articles. VHL: Virtual Health Library, EMBASE: Excerpta Medica Database.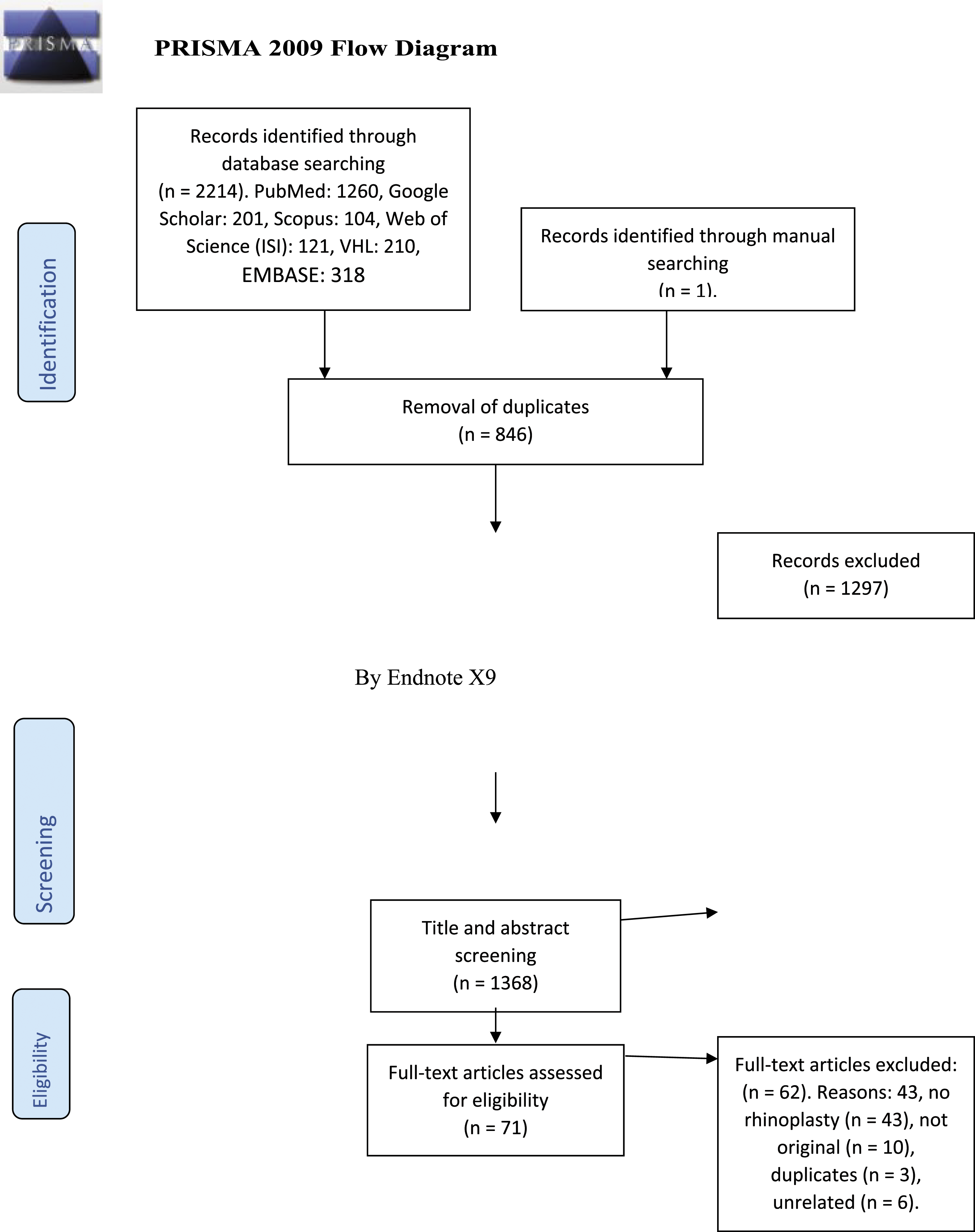
Risk of Bias
Assessment of bias using the modified Newcastle–Ottawa scale for cross-sectional studies.
Baseline Characteristics
Characteristics and conclusions of the included studies.
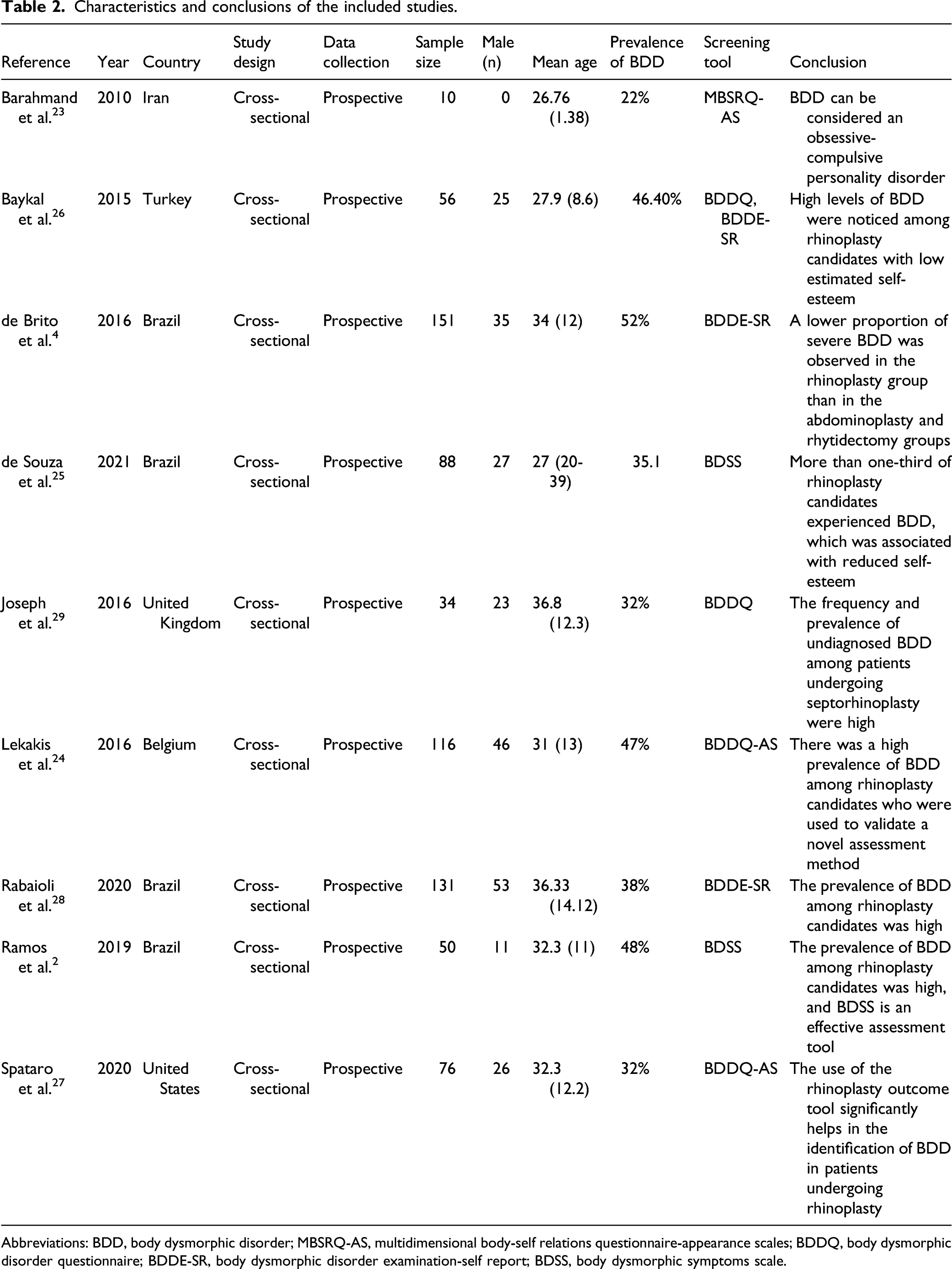
Abbreviations: BDD, body dysmorphic disorder; MBSRQ-AS, multidimensional body-self relations questionnaire-appearance scales; BDDQ, body dysmorphic disorder questionnaire; BDDE-SR, body dysmorphic disorder examination-self report; BDSS, body dysmorphic symptoms scale.
Discussion
In this section, we report and discuss the results of the included reports of the prevalence rates of BDD among rhinoplasty candidates. In brief, all the studies reported similar prevalence rates, with no significant variations, and most authors reported that the prevalence rates were high, especially in studies in which rhinoplasty candidates were compared with controls. A detailed discussion of all the included studies has been presented in the following paragraphs. In a Brazilian cross-sectional study, de Brito et al. 4 reported that the prevalence of BDD among rhinoplasty candidates was 52%, which was lower than the estimated rate among abdominoplasty candidates (57%) but higher than that among rhytidectomy candidates (42%). Furthermore, among the 3 groups, the severity of BDD was lowest in the rhinoplasty candidates. In another Brazilian cross-sectional study, Ramos et al. 2 reported a BDD prevalence rate of 48% among rhinoplasty candidates. Similarly, Lekakis et al. 24 who validated the Body Dysmorphic Disorder Questionnaire–Aesthetic Surgery (BDDQ-AS) in their cohort study, reported a prevalence rate of 47%. The control group in their study, which did not undergo rhinoplasty, had a BDD prevalence rate of 7% as assessed using the BDDQ-AS. De Souza et al. 25 compared the prevalence of BDD between rhinoplasty candidates and individuals from the general population in their cross-sectional analysis and reported that the rhinoplasty group had a higher prevalence of BDD and higher mean Body Dysmorphic Symptoms Scale score than the control group (rhinoplasty: 35.1% vs control: 3.2% and rhinoplasty: 53-6 and 1 0–2, P < .001, respectively).
A Turkish cross-sectional study by Baykal et al. 26 found that rhinoplasty candidates tended to have high BDD scores and low estimated self-esteem scores. Spataro et al. 27 estimated a BDD prevalence rate of 32% among rhinoplasty candidates in the United States and also reported that the use of the Standardized Cosmesis and Health Nasal Outcomes Survey was significantly associated with the severity and identification of BDD. A study of 100 Iranian female rhinoplasty candidates revealed a relatively low BDD prevalence rate of 22%. 23 In 2020, another A Brazilian study by Rabaioli et al. in 2020 28 reported that the prevalence of BDD among rhinoplasty candidates was 38%, which was considered high by the authors. The participants of that study were divided into the mild-to-moderate (n = 39), without symptoms (n = 81), and severe BDD (n = 11) groups based on their Body Dysmorphic Disorder Examination scores, with estimated total mean scores of 89.02, 32.90, and 114.90, respectively. In the United Kingdom, Joseph et al. 29 also reported that the prevalence of BDD among septorhinoplasty candidates was high, indicating an urgent need for adequate screening modalities for better prevention and management. They also reported that gender plays a significant role in the prevalence of BDD, with prevalence rates of 45% and 26% when rates were separately estimated for women and men, respectively. The prevalence rate of BDD in the control group of that study was 4%, and BDD was mostly observed in the women in the group. The prevalence rates in the studies included in this review are higher than those reported in the previous systematic review by Veale et al. 16 who reported prevalence rates ranging from 1.8% to 31.5%. Furthermore, in contrast to our findings, Veale et al. reported BDD was more prevalent in men than in women, and there was significant heterogeneity among the included studies in terms of the age of the included participants.
Our study may have some limitations. First, the lack of representation of certain cultures might represent a major limitation to the estimation of the global prevalence rate. Second, some studies did not identify and adjust for factors that could significantly affect the prevalence rate. Finally, the total sample size was relatively small. Considering that the evidence from the included studies is not representative, future investigations with fewer limitations are needed for adequate validation of the current evidence.
Our systematic review provides current evidence on the prevalence of BBD among rhinoplasty candidates. Our results indicate a high prevalence of BBD among rhinoplasty candidates, emphasizing the need for adequate interventions and management.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Authors’ contributions
Idea of the article: Ibrahim AlAwadh Literature Search: Naif AlSughier, Mohemmaed AlKarzae Solve arguments: Badi AlDosari Data Analysis: Ibrahim AlAwadh, Ahmed Bogari, Turki Azhar, Nada AlTaylouni Drafting and writing: Ibrahim AlAwadh, Ibrahim AlQuniabut Critical Revision: Badi AlDosari, Ahmed Bogari, Turki Azhar, Nada AlTaylouni.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.