
Abstract
We aimed to summarize the surgical treatment for pharyngolaryngeal stenosis and discuss prognosis in patients with Behcet’s disease. Six cases of pharyngolaryngeal stenosis caused by Behcet’s disease were analyzed retrospectively. All underwent surgical treatment for pharyngolaryngeal stenosis after systematic medical treatment. The follow-up time for the 6 patients was between 1 and 12 years. Four of the 6 patients underwent adhesiolysis as their first procedure. Two of these 4 experienced recurrence of stenosis within 6 months and underwent flap repair as their second procedure. The remaining two patients underwent flap reconstruction as their first procedure and maintained good swallowing function. Three of the 6 patients underwent preoperative tracheotomy because of dyspnea. Tracheal decannulation was successful in all patients. None of the patients experienced recurrence after their final surgical procedure and all recovered to a near-normal condition. Pharyngolaryngeal stenosis caused by Behcet’s disease is a rare but severe complication; surgical intervention should be considered in patients with dysphagia after systematic medical treatment.
Keywords
Introduction
Behcet’s disease is an uncommon systemic vasculitis of unknown etiology. 1 It can involve both arteries and veins of all sizes causing damage to almost all organ systems. Recurrent oral and genital ulcers, and eye lesions are the hallmarks of the disease, but otorhinolaryngological manifestations have occasionally been reported.2,3 In rare cases, Behcet’s disease has led to cicatricial pharyngolaryngeal webs and stenosis, which may be secondary to myositis. 4 Patients often present with dysphagia and/or dyspnea and require surgical intervention. 5
In the traditional surgical treatment of pharyngolaryngeal stenosis, adhesiolysis may be the only surgical procedure required; however, if stenosis subsequently recurs, adhesiolysis can be performed again. Removal of scar tissue and flap repair are carried out as simultaneously directly after adhesiolysis has been completed. Various flaps can be used for repair such as a pectoralis major myocutaneous flap, deltopectoral flap, anterolateral thigh flap, free jejunal transfer, or radial forearm free flap. These techniques have been used in pharyngolaryngeal reconstruction after tumor resection and have proved to be effective. 6 Free flaps have the advantages of being thin and soft when used for pharyngolaryngeal repair. However, in patients with Behcet’s disease, extensive vasculitis may cause increased failure of flap reconstruction. Pedicled myocutaneous flaps can also be affected by myositis and are slightly too thick and bulky for small or circumferential defects. 7 A flexible and reliable flap can be successfully used to reconstruct the pharyngolaryngeal region in patients with chronic vasculitis.
Here we report 6 patients with pharyngolaryngeal stenosis secondary to Behcet’s disease. Different surgical strategies were used to treat these conditions.
Methods
Data from 6 cases of pharyngolaryngeal stenosis (20–63 years old; 3 men and 3 women) caused by Behcet’s disease and treated between 2007 and 2019 in Beijing Tongren Hospital were analyzed retrospectively. All of these patients had been admitted to our department for dysphagia after recurrent pharyngeal ulcer. None of them had a past history of trauma or surgery at the time of presentation. After multidisciplinary consultation, they were diagnosed as having Behcet’s disease and received drug therapy in the Department of Rheumatology. Pharyngolaryngeal stenosis persisted after the ulcers had been treated with systematic medication (Figure 1). The patients were then transferred to our department for further management. Photographs of various pharyngolaryngeal stenoses caused by Behcet’s disease: (a,b) fiberoptic laryngoscopy showing adhesions between the posterior pharyngeal wall and soft palate; (c, d) stroboscopic laryngoscopy showing bilateral arytenoid fold extensively adhering to the posterior pharyngeal and lateral pharyngeal wall.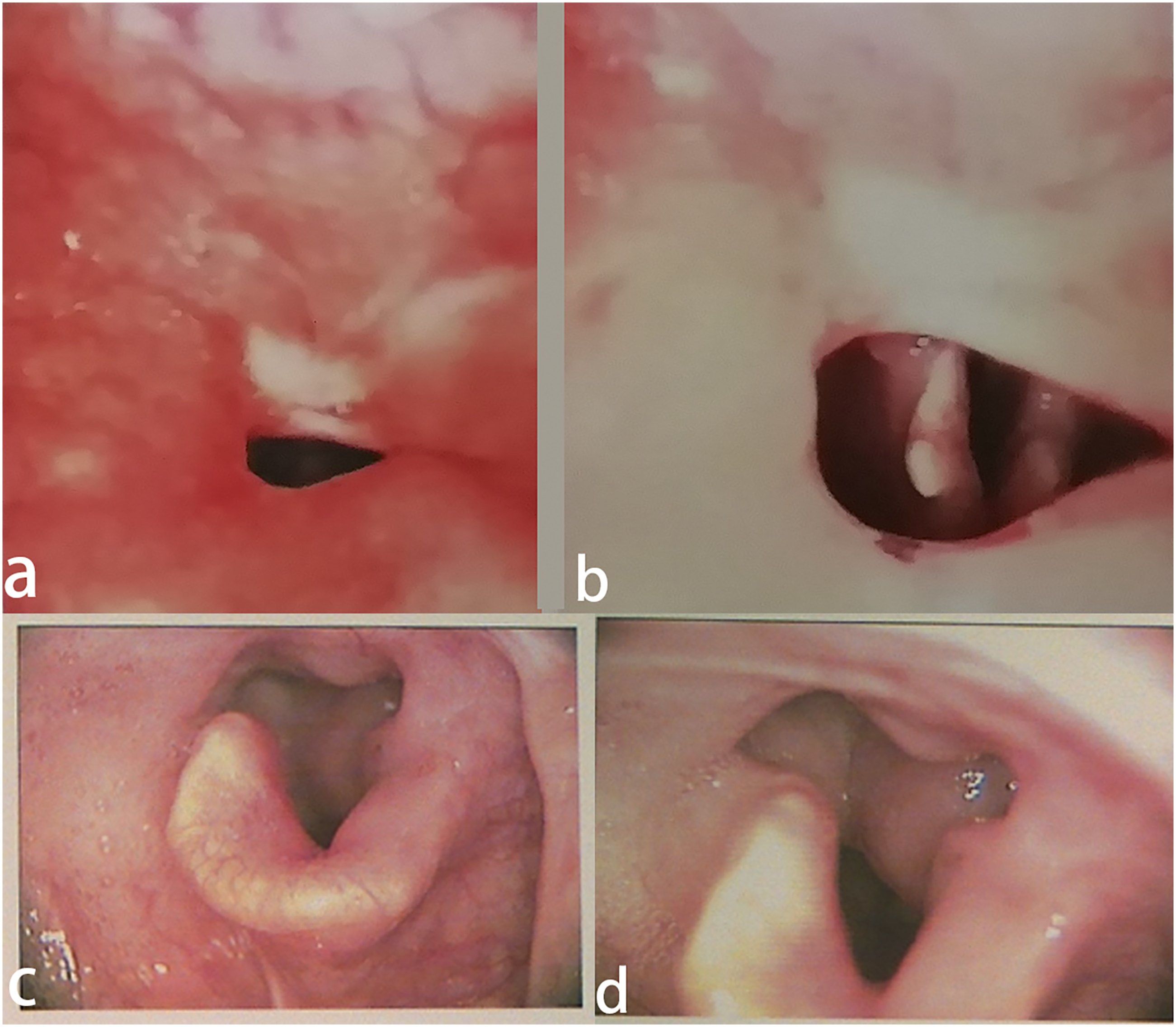
Most of the enrolled patients denied weight loss but the indexes of their BMI ranged from 16.0 to 21.6. Four patients had progressive dyspnea after exercise. Three patients underwent transoral laser microsurgery while two of them relapsed after 6 months. These two patients finally underwent flap repair 2–3 years later. Two patients underwent flap repair as the initial treatment. The other 1 patient underwent uvulopalatopharyngoplasty.
Surgical Procedure
Transoral laser microsurgery
The procedure was performed under general anesthesia. Cicatricial adhesions in the pharyngolarynx were divided under suspension laryngoscopy. A 5 W CO2 laser in continuous mode was used to separate the adhesions.
Internal mammary artery perforator (IMAP) flap
The location of the dominant IMAP was assessed by preoperative digital subtraction angiography (DSA) as has been described earlier.
8
The skin and subcutaneous tissue were cut parallel to the dominant IMAP. The IMAP and accompanying veins were dissected anterogradely from the lateral edge of the sternum. Then, from the superficial surface of the pectoralis major muscle, the flap was cut from the outside to inside, and the blood vessels were dissected retrogradely. The retrograde contour of the vascular pedicle was generally dissociated to 1–2 cm outside the sternum, making the flap easy to rotate (Figure 2A). The prepared flap was used to repair the stenosis caused by adhesion of scar tissue from the level of the epiglottis to the arytenoid cartilage. After incision of the neck, we protected the external branch of the superior laryngeal nerve and divided and ligated the superior thyroid blood vessel. The inferior pharyngeal constrictor muscle was cut longitudinally at the posterior edge of the thyroid cartilage plate. After one-third of the thyroid cartilage plate had been removed, the mucosa was cut into the pharyngeal cavity, the adhesion between the epiglottis, arytenoid cartilage, and the posterior pharyngeal wall was separated, and the submucosal scar tissue on the posterior pharyngeal wall was removed. The IMAP flap was moved up to the neck through the subcutaneous tunnel (Figure 2B) and inserted into the narrow part of the hypopharyngeal. The epidermis surface was rotated so that it lined the pharynx, and an inverted mattress suture was made with the surrounding residual mucosa. The excess skin tissue was trimmed to remove the dermis. The donor area was directly closed and sutured. (A) Harvesting of the internal mammary artery perforator flap. (B) The flap passes through the subcutaneous tunnel to the neck, and the excess dermis was removed.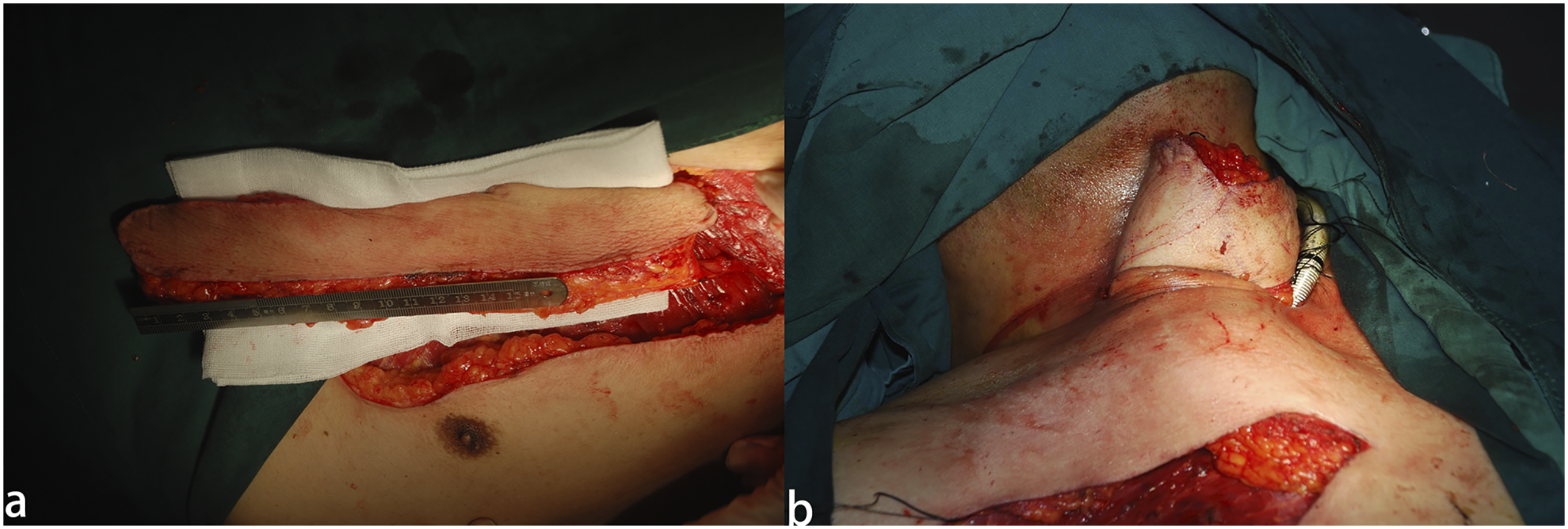
Supraclavicular artery flap
An ultrasonic Doppler blood flow meter was used to detect the cutaneous perforator of the transverse cervical artery in the supraclavicular region. The cutaneous branch, also known as the supraclavicular artery, is located in the triangle that is enveloped by the posterior border of the sternocleidomastoid muscle, external jugular vein, and the upper border of the clavicle. It arises from the transverse cervical artery in 93% of cases (7% from the suprascapular artery). 9
First, the transverse cervical artery was dissected at the intersection of the omohyoid muscle and the sternocleidomastoid muscle. The transverse cervical artery was then dissected anterogradely to confirm the origin of the supraclavicular artery in the triangle. The accompanying veins flowing into the transverse cervical vein or external jugular vein were preserved. The supraclavicular artery was dissected anterogradely for 1–2 cm, and an extended incision was made in the direction of the blood vessel as the long axis of the flap. The island flap was designed according to the size of the defect in the receiving area, and the flap was separated from the distal end to the proximal end on the superficial surface of the muscle. The deep branch of the transverse carotid artery, which enters into the trapezius muscle, was ligated and divided to ensure that the flap was delivered to the neck without tension (Figure 3A). Similar to the application of the IMAP, after part of the thyroid cartilage had been removed, the flap was raised from distal to proximal above the muscle and entered the pharyngeal cavity from the lateral pharyngeal wall to repair the mucosal defect after resection of scar tissue (Figure 3B). The donor site was sutured and sealed directly after release. (A) Harvesting of the supraclavicular artery flap. (B) The flap was transferred to the pharyngeal cavity through the lateral pharyngeal wall incision and fixed to the residual mucosa by an inverted suture.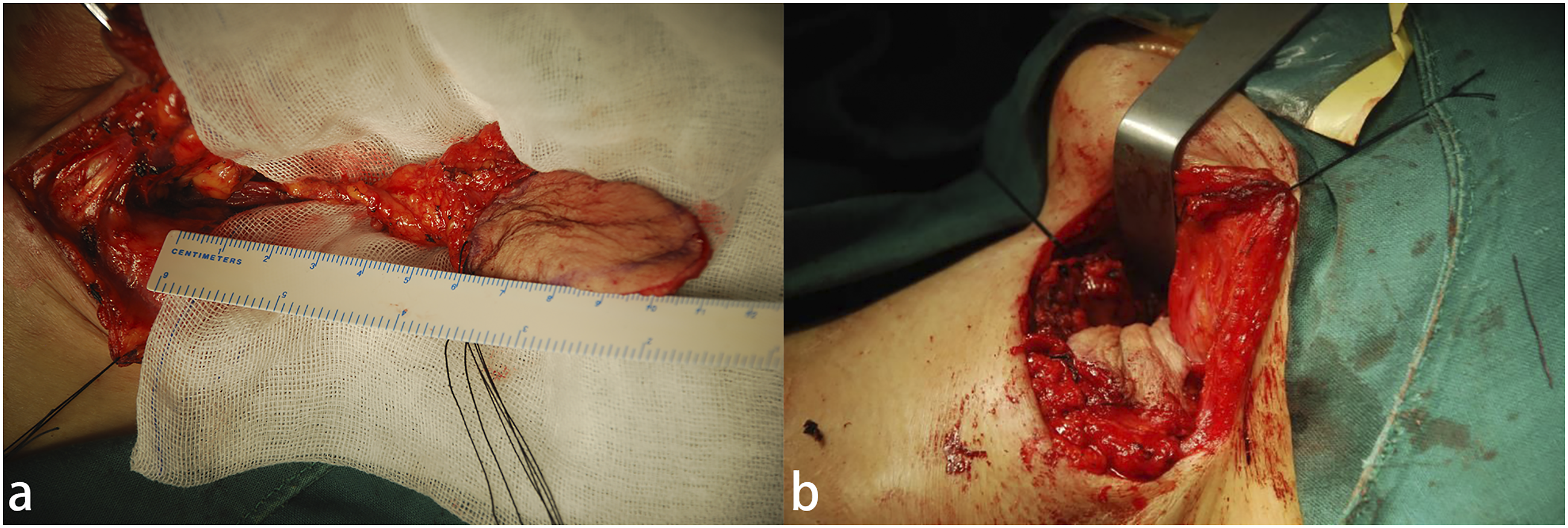
Submental island flap
The proximal parts of the facial artery and submental vessels are the pedicle of this flap. The upper incision was made along the inferior border of the mandible into the deep side of the deep cervical fascia. The marginal mandibular nerve was identified and protected on the superficial surface of the submandibular gland, mylohyoid, and digastric muscle. The submental artery was identified at the junction of the digastric anterior and mylohyoid muscle after the facial artery and anterior facial vein had been dissected. The flap was raised and separated in the plane of the deep side of the platysma from the contralateral side. The branches leading to the submandibular gland, digastric anterior, and mylohyoid muscle were ligated. The distal end of the facial artery and vein were ligated at the inferior margin of the mandible (Figure 4A). (A) Harvesting of the submental island flap. (B) The flap was sutured to the residual mucosal margin of the soft palate and lateral pharyngeal wall through the medial tunnel in the mandible.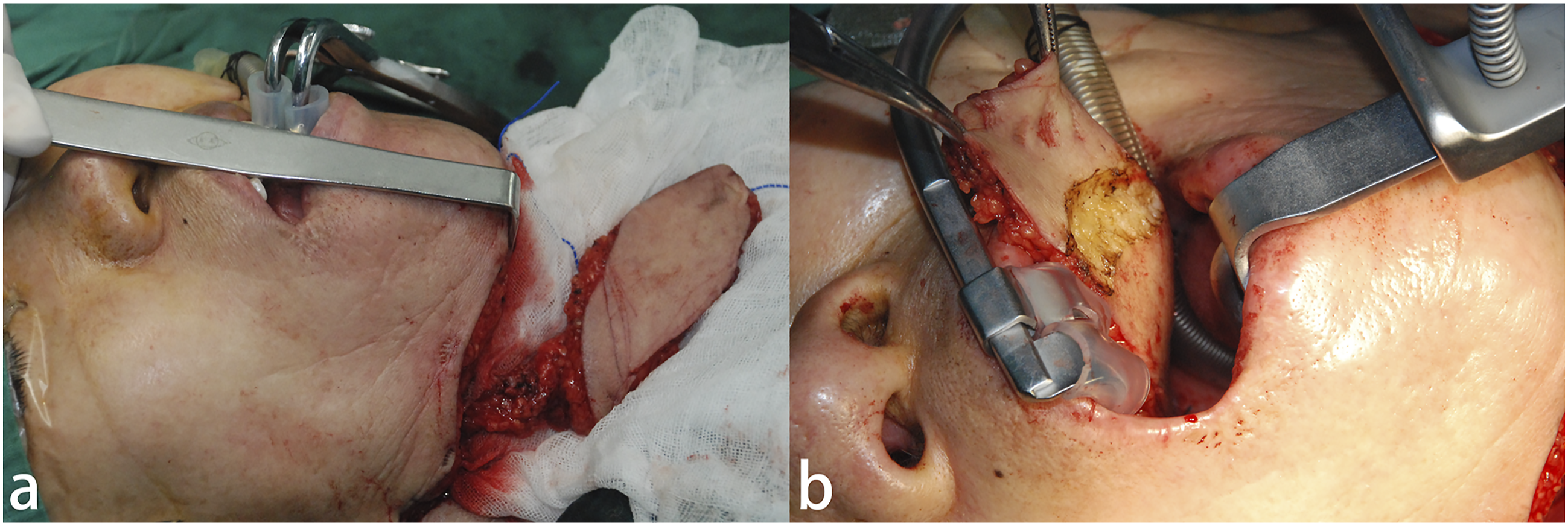
A tunnel was made inside the mandible, the distal end of the flap was pulled with the suture and transferred to the pharyngeal cavity through the tunnel, with the skin facing the pharyngeal cavity (Figure 4B). The skin surface of the flap was sutured to the soft palate residue after resection of scar tissue, to the mucosal free edge of the wound after tonsillectomy, and to the mucosal edge at the root of the tongue. The donor site in the neck could be sutured directly. In male patients, the hair follicles on the flap will gradually shrink and will not be affected in the long term.
Results
The follow-up period for the 6 patients varied between 1 and 12 years. Four of the 6 patients underwent 1 surgical procedure (2 adhesiolysis and 2 pedicled flap surgery) and the remaining two patients underwent two surgical procedures (pedicled flap reconstruction for recurrent adhesions after primary adhesiolysis). Three patients underwent preoperative tracheotomy because of dyspnea. Tracheal intubations were successfully removed in all patients during follow-up. None of them experienced disease recurrence after their final surgical procedure.
The functional oral intake scale (FOIS) 10 was used to assess oral intake. The scores were in the range 4–5 preoperatively and increased to 6–7 postoperatively.
Discussion
In this retrospective study, we analyzed data from 6 cases with pharyngolaryngeal stenosis due to Behcet’s disease who underwent either adhesiolysis alone (2 cases) or flap repair surgery using different types of flap (4 cases) after systematic medical treatment. All of them presented with pharyngeal adhesions resulting from repeated inflammation at the free edge of the soft palate and aryepiglottic fold. Four patients underwent adhesiolysis alone (3 transoral laser microsurgery and 1 uvulopalatopharyngoplasty) as their first surgical procedure. Two of these patients experienced recurrence of disease within 6 months and underwent flap repair. Two patients underwent flap reconstruction as their first procedure and maintained good swallowing function. The preoperative and postoperative average FOIS scores were 4.3 and 6.8, respectively. All of the patients recovered to a near-normal level.
For small adhesions between the posterior pharyngeal wall and anterior soft tissue, adhesiolysis alone without flap repair seemed to be effective and sufficient. Adhesions did not usually recur after release. When the lesion involved the lateral pharyngeal wall, circumferential scars would form. Residual scar tissue was prone to close again and adhesions usually relapsed after simple loosening. The two patients with adhesions of both lateral pharyngeal wall and posterior pharyngeal wall relapsed with new strictures after the first adhesiolysis procedure. In this situation, extensive resection of scars and insertion of healthy flaps prevented or decreased the development of adhesions. For the other two patients with circumferential adhesions, we performed flap repair as the first surgical treatment and observed a stable swallowing function.
The reconstruction of pharyngolaryngeal stenosis caused by Behcet’s disease was different from reconstructions required from other causes such as mechanical or chemical trauma, resection of local tumor, or chemo-/radiotherapy. For those other causes of pharyngolaryngeal stenosis, we usually used dilation 11 and other types of reconstructive surgery to address the issue. In those cases, the flap for the reconstructive surgery was always made using a thin and pliable material such as a radial forearm free flap. While the same strategy was used for the pharyngolaryngeal stenosis caused by Behcet’s disease, there may be a high risk of failure under certain circumstances such as vasculitis. 12
Compared with a free flap, a pedicled flap is more suitable for reconstruction after pharyngolaryngeal stenosis caused by Behcet’s disease. Traditional pedicle flaps such as myocutaneous flaps (e.g., pectoralis major, trapezius, latissimus dorsi) are quite bulky for this site without resection of a large amount of tissue, as is common in cancer therapy.
In this study, the internal mammary artery perforator (IMAP) flap, the supraclavicular artery flap, and the submental island flap were used to reconstruct the pharyngolaryngeal stenosis. The IMAP flap was the application of the “perforator flap concept” which was first introduced by Koshima and Soeda in 1989, 13 and has been used in defect reconstruction in head and neck surgery. 14 The supraclavicular artery island flap and the submental island flap are effective in the reconstruction of head and neck defects, and have been confirmed to have several advantages over distant free flaps.15,16
In our study, all of the patients who underwent island flap reconstruction as mentioned above recovered to a near-normal level: 5 patients recovered their normal swallowing function, and 1 patient still had difficulty in swallowing dry large food, which confirmed our premise to some extent, that local island flaps are suitable for the reconstruction of pharyngolaryngeal stenosis caused by Behcet’s disease. They require a shorter operating time, are more successful in avoiding microvascular anastomosis and have lower donor site sequelae.
Conclusion
Pharyngolaryngeal stenosis caused by Behcet’s disease is a rare but severe complication. Surgical intervention should be considered in patients with dysphagia after systematic medical treatment. A local island flap may be an appropriate option to reconstruct the pharyngeal cavity, especially in patients with extensive adhesions involving the lateral pharyngeal wall.
Footnotes
Acknowledgments
The authors wish to thank the numerous individuals who participated in this study.
Author’s Note
This study was approved by the Human Ethics Committee of Beijing Tongren Hospital, Capital Medical University. All authors have read the manuscript and approved its submission for publication.
Author Contributions
Drafting the manuscript: Junwei Huang, Zufei LiAcquisition of data: Hanyuan DuanAnalysis of data: Xiaohong ChenRevising the manuscript for important intellectual content: Hanyuan Duan, Zhigang HuangConception and design of study: Junwei Huang, Xiaohong Chen, Zufei Li
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Supported by the Beihang-Tongren big data high level Innovation Center open fund project (BHTR-KFJJ-202008) and Leading talents of "new innovation project" in Beijing Economic and Technological Development Zone (ZXZC202001020039).
Availability of Data and Materials
The datasets generated and/or analyzed during the current study are not publicly available to protect the privacy of patients, but are available from the corresponding author on reasonable request.