
Abstract
Extraskeletal Ewing sarcoma (EES) is a relatively rare primary tumor of the soft tissues predominantly affecting men in the second and third decades of life. They are a less common form of the cancerous growth known as an Ewing sarcoma, which occurs in bones or soft tissue such as cartilage. Head and neck ESS can require intervention including endoscopic sinus surgery, septoplasty, inferior turbinectomy, and left internal nasal valve repairs with septal cartilage This is a case report on an unusual presentation of ESS in the sinonasal region.
Introduction
Ewing’s sarcoma (ES) is a rare type of cancerous growth occurring in bones or soft tissue surrounding bones—such as cartilage or nerves. Ewing’s sarcomas are some of the most aggressive adult and childhood cancers due to both unresponsiveness to treatment as well as potential metastases.1,2 Less common are extraskeletal Ewing sarcomas (EES) which occur in soft tissues and rarely form in the head and neck. 3 These tumors typically affect 10- to 20-year-olds and have a high cure rate, as it is more responsive to chemotherapy than other soft tissue sarcomas. Ewing’s sarcoma affects about 200 children and young adults every year in the United States and shows up slightly more often in males. While adults can get ES, it is uncommon. There have been few studies of EES in the head and neck. An extensive study done in 1973 by Ogura and Schenck 1-4 discussed unusual nasal tumors, and ES was not among them.We report an unusual case of EES in the nasal region.
Case
Presentation
A 56-year-old Hispanic male with a past medical history of hypercholesterolemia, essential hypertension, gastroesophageal reflux, hypotestosteronemia, obstructive sleep apnea, and chronic sinusitis was referred by his primary care physician (PCP) for sinus surgery. The patient presented with nasal congestion, right nasal obstruction, and sinus pressure. His past medical history is significant for recurrent sinus infections requiring antibiotic therapy on multiple occasions. In addition, he has been dependent upon Afrin for nasal congestion. His PCP successfully changed him to over the counter nasal sprays with no relief of his nasal obstruction symptoms. Computed tomography (CT) sinus at an outside facility showed bilateral maxillary sinus with lobulated mucosal thickening, multiple opacified posterior left ethmoid cells, and a 13-mm lobulated soft tissue density of the posterior superior left nasal fossa consistent with a polyp formation.
A more current preoperative CT sinus (Figure 1) showed disease in the posterior ethmoids and the frontals floors, deviated nasal septum impacted into the left inferior turbinate and multiple polyps in both maxillary sinuses. Preoperative CT sinus (August 2020). Left septal deviated nasal septum impacted into the left inferior turbinate and multiple polyps in both maxillary sinuses. On further image review, there is disease in the posterior ethmoids and the frontal floors.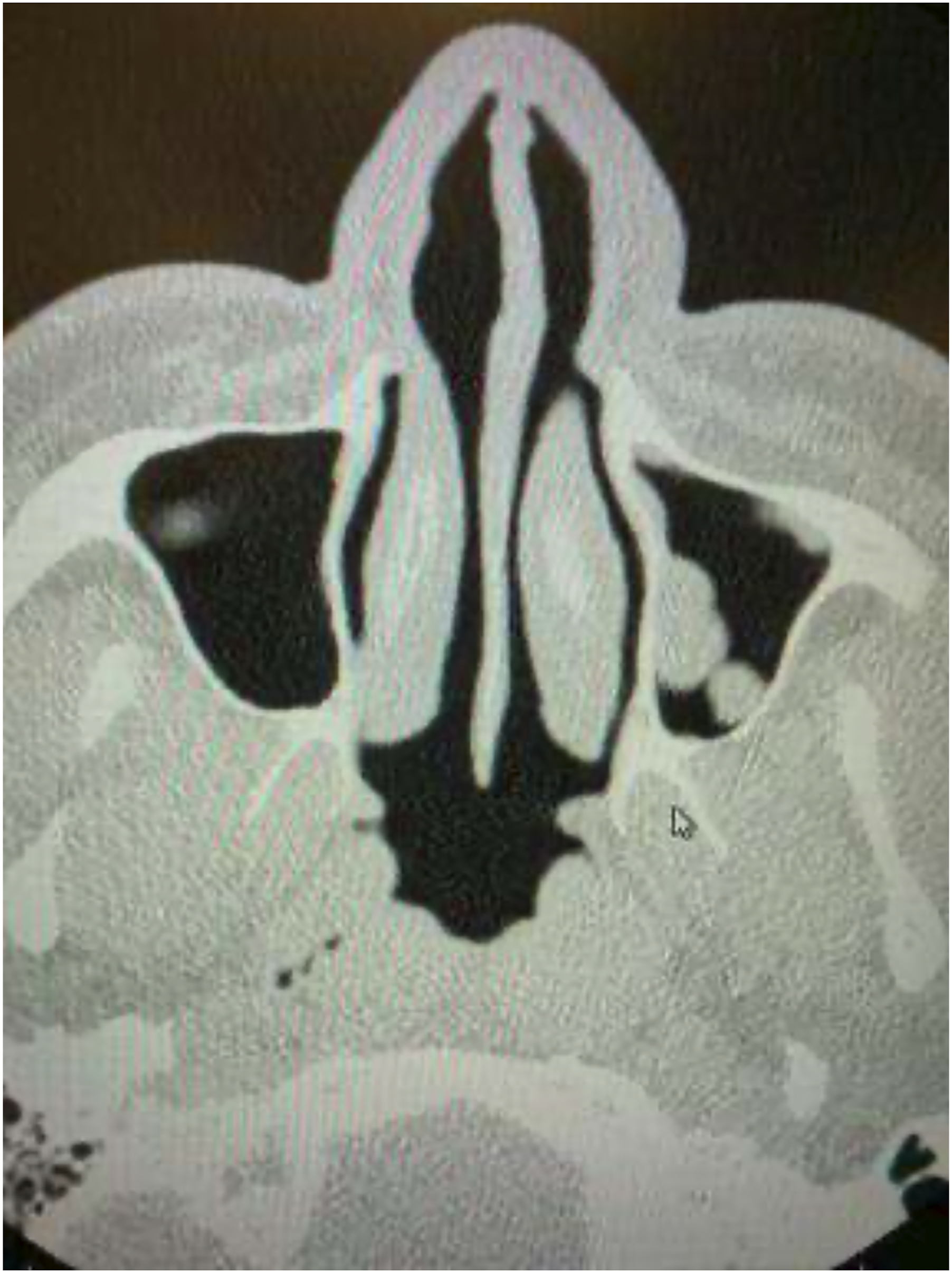
Intervention and Treatment
Image-guided functional endoscopic sinus surgery (FESS), septoplasty, inferior turbinectomy, and left internal nasal valve repair with septal cartilage were performed endoscopic images can be seen in Figure 2. An untouched round 3.5-cm mucosal covered mass was suctioned out from the right ethmoid area at the end of the surgery. However, the most likely etiology was from the left side according to the preop CT scan. Initial surgical pathology showed malignant undifferentiated epithelioid neoplasm, high grade, in the right ethmoid. Endoscopic view shows an ethmoid polyp.
Postop MRI of the sinus showed a mass in the “left” anterior nasal fossa associated with the middle turbinate. This mass suggested a neoplastic disease although it did not enhance with contrast. Follow-up PET scan showed only a mild active right inguinal lymph node. A revision FESS, total bilateral ethmoidectomy, and bilateral partial maxillectomy followed after the additional diagnostic exams. The tumor emanated from the left middle turbinate, as expected.
Outcome
Prior to the final pathology report, slides were sent to Mayo Clinic for additional studies, and the report was amended to incorporate additional findings: the sarcoma fusion panel demonstrated an EWSR1-Fli1 rearrangement. The final diagnosis was changed from “Malignant undifferentiated epithelioid neoplasm, high grade” to “Extraskeletal Ewing Sarcoma, EWSR1-Fli-1.” General histological slides showed sheets of small cells with a high nuclear-to-cytoplasmic ratio. 5 The CD99 markers and FLl-1 markers positivity supported the diagnosis of EES.
After the revision FESS, the final pathology confirmed EES in the left middle turbinate.
Discussion
Extraskeletal Ewing sarcoma was first discussed in 1969 as a small cell tumor in children. 6 Since then, there have been few studies reviewing EES, which typically presents as a painful, rapidly growing mass. 6 Extraskeletal Ewing sarcoma has been shown to mostly affect female Caucasians and has rarely been found in African Americans and Asian Americans. In addition, patients with EES were shown to have a higher mean age than those with ES.7,8
Studies on patients with EES have found that the 5-year survival rate was between 59.7–69.7%, although the prognosis is directly correlated to the site, size, gender, age, metastases, and previous cancer history.8-11 The survival rate has increased over time due to treatment protocols calling for the combination of different methods such as chemotherapy and surgery. 11
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.