
Abstract
Introduction
Paraganglioma of the head and neck is a type of neurogenic tumor originating from the neural crest cells of the ectoderm. The incidence rate is 1:30000–1:100 000, accounting for .6% of head and neck tumors. 1 The carotid body accounts for approximately 60% of paragangliomas of the head and neck. 2 Paraganglioma can also occur in the jugular bulb, tympanum, and vagus nerve. Due to the complex anatomic structure of the head and neck, the tumor lies adjacent to large vessels, and lower cranial nerves, imposing a propensity of risks for extirpation of these tumors.
At present, studies show that the disease is related to genetic abnormalities and environmental factors. In 2000, Baysal et al first discovered SDHD gene mutations in patients with paraganglioma, 3 and the pathogenic genes subsequently discovered can be divided into the following 3 categories: pseudohypoxic signaling clusters including VHL, SDHx, EGLN1, EGLN2, EPAS1/HIF2A, FH, MDH2, and IDH; kinase signaling clusters including NF1, RET, KIF1B, MAX, TMEM127, H-RAS, ATRX, K-RAS, and FGFR; Wnt signaling clusters including CSDE1 mutation and MAML3 fusion. 4 The incidence of paraganglioma is higher in patients who live in a high-altitude environment or who experience chronic hypoxic diseases. 5
Approximately 10% of paragangliomas will progress to malignancy. 6 The natural course of malignant paraganglioma is highly heterogeneous, and the 5-year survival rate ranges from 12% to 85%. 6,7 Unlike other malignancies, malignant paragangliomas have no obvious pathological features, and the local appearance of the tumor cannot be used as a criterion for distinguishing benign from malignant paragangliomas. Malignant paraganglioma can only be determined by regional lymph node or distant tissue metastasis. 8 Due to the slow growth of paragangliomas, surgical resection may not be the first choice of treatment because of possible severe postoperative complications. However, malignant paragangliomas require timely treatment, but they cannot be distinguished from benign tumors at an early stage; as such, affected patients often miss the optimal time window for treatment. However, there is no recognized standard treatment for such diseases, given the extremely low incidence of malignant paragangliomas of the head and neck.
This study summarized the clinicopathological and genetic features of different types of head and neck malignant paragangliomas and analyzed various treatment modalities and prognoses, aiming to provide a reference for future treatment options for this rare disease.
Patients and Methods
This study included 6 patients with head and neck malignant paraganglioma who were treated between February 2015 and January 2020 at Beijing Tongren Hospital, Capital Medical University in China. The general information, main symptoms, physical examination, imaging examination, surgery and other treatment methods, postoperative symptoms and pathological results were collected, and the patients were followed up regularly. The diagnosis of malignant paraganglioma was confirmed by pathological results and regional lymph node or distant tissue metastasis.
This study was approved by the ethics committee of Beijing Tongren Hospital. All patients were informed of the content and significance of this study. On the premise that they had full knowledge of the study, the patients signed informed consent forms and participated in the study. Blood samples or paraffin-embedded tumor tissue samples were collected. At least 50 nanograms of DNA was isolated from each sample, and genetic testing related to paraganglioma was performed to determine the mutant gene, exon number, nucleotide variation, amino acid variation, and mutation type of the mutated gene.
Results
Clinical and Histopathological Characteristics
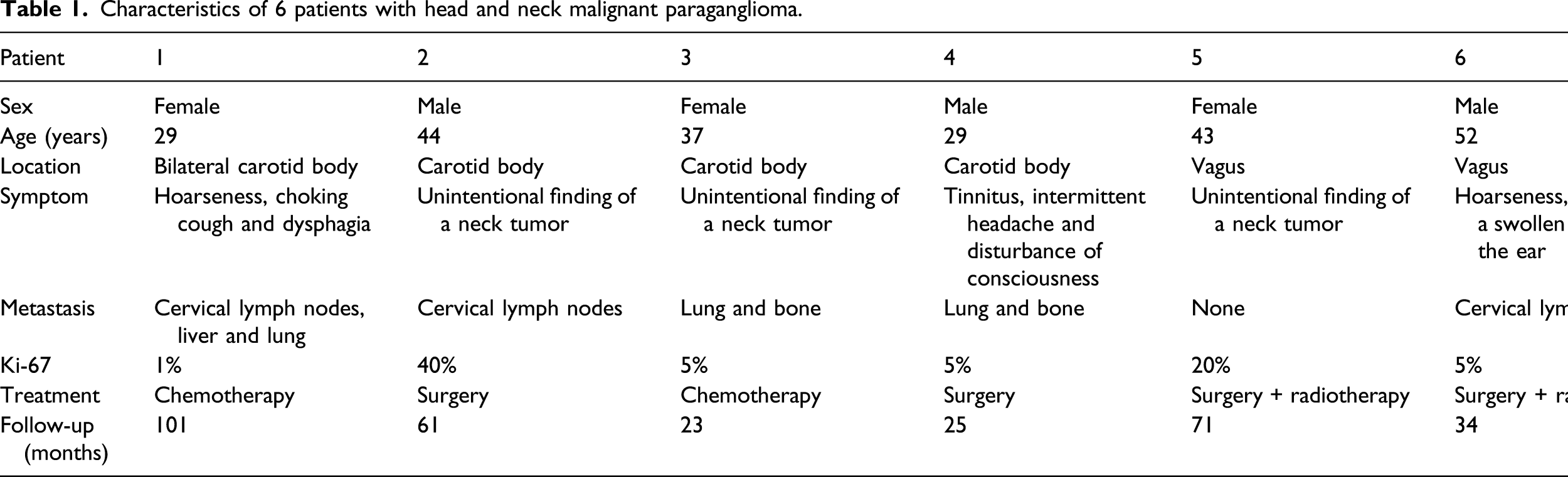
Characteristics of 6 patients with head and neck malignant paraganglioma.
Overall Survival of Patients Who Underwent Surgical Resection
The two patients with malignant carotid body tumors underwent lateral cervical vagotomy for carotid body tumor resection with reconstruction of the internal carotid artery using the great saphenous vein. After surgery, both developed hoarseness, choking cough, and tongue deviation, but the symptoms of neurological impairment gradually improved, and the only long-term complaints were mild hoarseness and tongue deviation.
With regard to the two cases with malignant vagal paraganglioma, one of them underwent lateral cervical vagotomy for vagal paraganglioma resection, and the other underwent lateral cervical vagotomy and mandibular dehiscence for vagal paraganglioma resection with tracheotomy. Both experienced severe hoarseness, dysphagia, and tongue deviation after surgery, and the symptoms were not significantly relieved in the long term. Local radiotherapy was performed after surgery.
Treatment and Prognosis of Patients Who Underwent Nonoperative Treatment
Distant metastases were present at the time of diagnosis in the two cases with malignant carotid body tumors. After the primary tumor had been diagnosed pathologically, each patient received 6 cycles of paclitaxel, ifosfamide, and dacarbazine. After chemotherapy, grade I–II gastrointestinal reaction occurred with no myelosuppression. In response to chemotherapy, one case (Patient 1) showed stable disease (SD), but hoarseness and other symptoms were improved compared with before treatment. At the follow-up time, the tumor showed no obvious change. The follow-up time was 101 months. In the other case (Patient 3), the effect of chemotherapy was a partial response (PR). In this case, the follow-up time was 23 months, and the tumor showed no obvious change.
Genomic Analysis
Summary of mutant genes.

Discussion
Clinicopathological Characteristics and Diagnosis of Malignancies
Previous studies developed the grading system for adrenal pheochromocytoma and paraganglioma (GAPP), 10 which combines clinical and histological parameters to grade tumors. However, follow-up studies have shown that GAPP has high interobserver variability and is not suitable for conventional use to distinguish between benign and malignant paragangliomas. 11 Moreover, mitotic activity, cellular atypia or vascular invasion cannot reliably predict the malignant tendency of paraganglioma. 12 In addition, there is no clear correlation between the degree of local invasion and the risk of metastasis. 13
In the present study, the level of Ki-67 expression was not related to tumor invasion or metastasis. Positive expression of Ki-67 in the primary tumor in cases showing multiple organ metastases and local lymph node metastases was 1% (Case 1), while positive expression of Ki-67 in the primary tumor in cases showing only local lymph node metastases was up to 40% (Case 2). Therefore, the diagnosis of malignant tumors still depends on the presence of metastasis in nonchromaffin sites distant from the primary tumor. However, paraganglioma may still metastasize 50 years after initial diagnosis, 14 thus long-term monitoring of recurrent or metastatic diseases is necessary. Old age at diagnosis, large primary tumor size, no surgical resection of primary tumor and synchronous metastasis are important predictors of rapid disease progression and death. 7
Paragangliomas with abnormal histological findings also require close follow-up. In this study, a case of paraganglioma of the vagus nerve was characterized pathologically by cell atypia, active cell proliferation, intravascular tumor thrombus, and tumor invasion into nerve fiber tracts. SDHB mutation was identified by gene analysis and was strongly related to the invasion and metastasis of the paraganglioma. Therefore, this patient should be treated as having a malignant paraganglioma and undergo further follow-up.
Choice of Treatment Strategy
Previous studies have shown that primary tumor resection has a positive impact on the overall survival rate of patients with malignant paraganglioma, and surgical extirpation is still the preferred treatment for such diseases. 15 For paraganglioma with no evidence of lymph node metastasis, it is recommended that lymph nodes in the adjacent area should be routinely dissected to identify the potential for hidden metastasis. 6 The recommended scope of intraoperative lymph node dissection needs to be determined. Some researchers believe that at least the lymph nodes in zones IIa, IIb and III should be included. 16 In this study, all patients with paragangliomas underwent routine neck lymph node dissection in areas II and III. Two patients with malignant head and neck paraganglioma had cervical lymph node metastasis without distant metastasis. When distant metastases are present, the strategy to treat the primary lesion should depend on details of the actual situation.
In this study, 3 patients with metastatic lesions were identified at the initial diagnosis, and only one patient underwent surgical treatment. That patient presented with intermittent headache and disturbance of consciousness and had a Shamblin III carotid body tumor. As the symptoms were caused by tumor compression of the internal carotid artery, the tumor was surgically removed, and the ipsilateral internal carotid artery was reconstructed using the autologous great saphenous vein. Another two patients with metastases preferred chemotherapy after the tumor biopsy had been clearly diagnosed. Previous studies have shown that chemotherapy with cyclophosphamide, vincristine and dacarbazine is an effective treatment for tumor growth control in patients with metastatic paraganglioma. 17 Meta-analysis of the effect of chemotherapy on tumor volume showed that complete response (CR), PR and SD were 4%, 37%, and 14%, respectively. 18 Compared with previous studies, the treatment efficacy showed similar survival outcomes for these two patients who underwent chemotherapy. 17,18 In our study, paclitaxel was used for chemotherapy of malignant paraganglioma for the first time and achieved good disease control.
In patients with unresectable metastatic paraganglioma, radiotherapy is effective for local tumor stability and symptom improvement. 19 Although radiotherapy alone cannot provide the best chance of a cure, it can be used as an adjuvant treatment to prolong survival and reduce tumor size. 20 Unlike carotid body tumors, paraganglioma of the vagus nerve tends to grow longitudinally along the vagus nerve, and it is difficult to guarantee a negative surgical margin during surgery. Therefore, the two patients with malignant vagal paraganglioma in this study were treated with local adjuvant radiotherapy after complete tumor resection and neck lymph node dissection, and no tumor recurrence or new metastasis has been found thus far.
We summarized the treatment strategies for head and neck malignant paraganglioma based on experience at a single institution, which may provide a reference for the treatment of malignant paragangliomas (Figure 1). Treatment strategy for head and neck malignant paraganglioma. Notes: HNPGL: Head and neck paraganglioma; CBT: Carotid body tumor; VPGL: Vagal paraganglioma.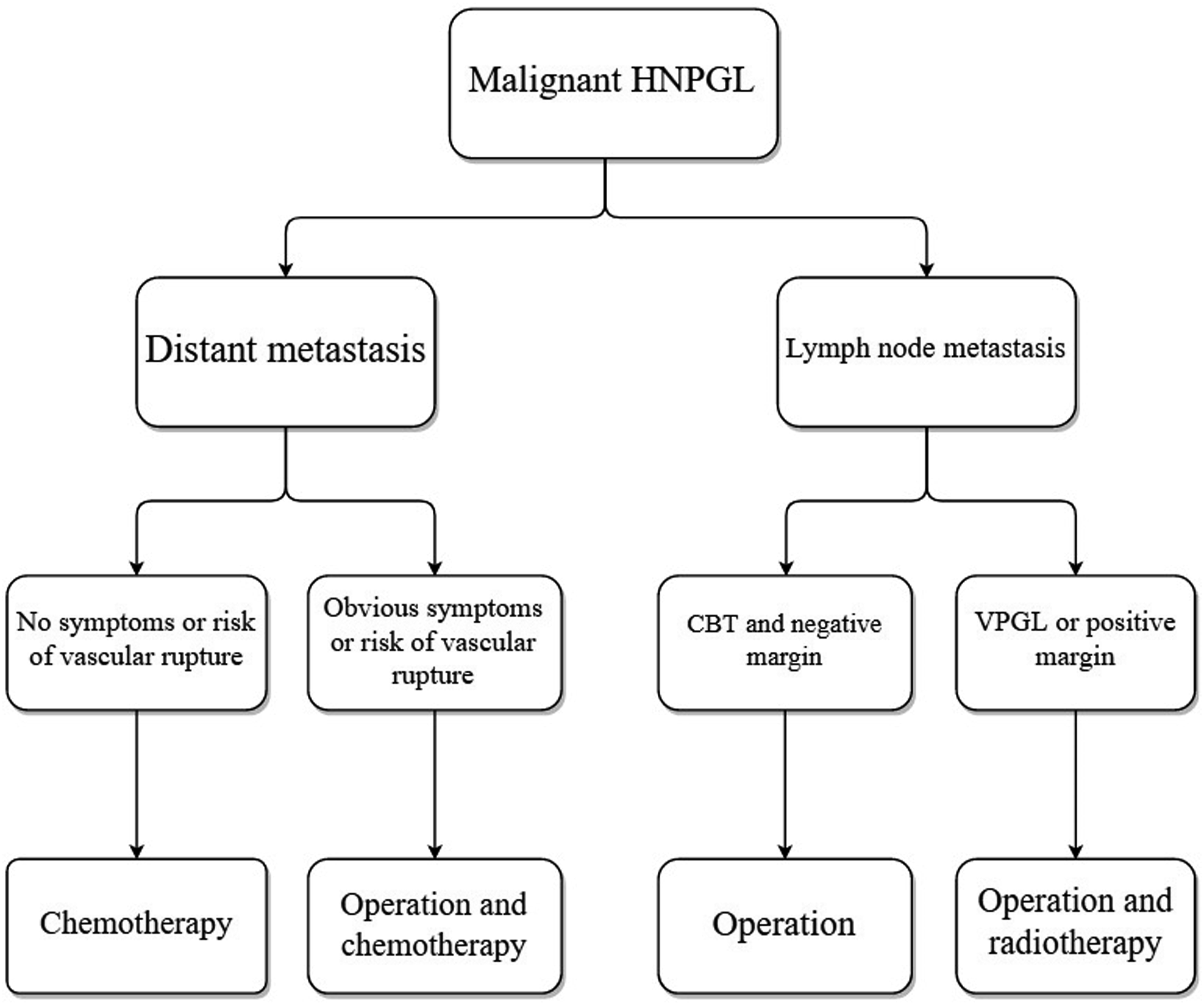
Prognosis and Rehabilitation
Reports on the clinical course of metastatic paraganglioma are very inconsistent, and the 5-year survival rate is between 12% and 85%. 6,7 All 6 patients in this study are still alive at the present time, the follow-up time was 25-101 months, and the median follow-up time was 66 months. After the treatment, no obvious progression or new metastasis was found in any of the cases. It can be preliminarily determined that the progression of the disease is still slow even if the head and neck paraganglioma is malignant. However, paraganglioma of the head and neck can compress or invade the adjacent nerves of the neck and skull base, resulting in neurological dysfunction, which is usually manifested as sympathetic nerve and X, XI, XII cranial nerve dysfunction. 6 In this study, all patients experienced variable extents of hoarseness, dysphagia, coughing upon drinking, tongue deviation, Horner syndrome or other neurological impairments after surgical resection. Of note, the neurological dysfunction symptoms of patients with malignant vagal paraganglioma were relatively severe, and further rehabilitation was required.
Mutant Gene Analysis
The occurrence and development of paragangliomas are driven by genomic alterations. At least 35% of paraganglioma patients carry mutations in related pathogenic genes. 21 It has been confirmed that SDHB, SLC25A11, and FH gene mutations are associated with a higher risk of malignant transformation of paraganglioma. 22 -24 This study identified one case each of SDHD, SDHB, ATR, and MAP3K13 gene mutations through genetic testing.
SDHx is a group of tumor suppressor genes, and mutation of these genes can inactivate the SDH enzyme, resulting in a loss of catalytic activity. Subsequently, the accumulation of succinic acid can competitively inhibit the proline hydroxylation of hypoxia inducible factor α (HIF-α), which can stabilize and heterodimerize HIF-α and then promote the expression of target genes such as vascular endothelial growth factor and glucose transporter 1. These changes lead to pseudohypoxia and the activation of various pathways of tumor development. 25 Germline mutation of the SDHx gene is associated with familial pheochromocytoma and paraganglioma disease. They are inherited in an autosomal dominant manner and have an age-related incomplete penetrance. 26 SDHB gene mutation is considered to be one of the most important risk factors for malignant transformation of paraganglioma. According to a meta-analysis report, 30% of patients with malignant paraganglioma carry SDHB gene mutations. 27 The penetrance rate of paraganglioma in SDHB gene carriers is 25-50%, and metastatic disease occurs in 17% of patients. 28,29 In addition, the overall survival of patients with SDHB gene mutations in malignant paraganglioma is shorter than that of patients with non-SDHB gene mutations. 9 SDHD gene mutations are associated with multiple paragangliomas, and most are benign tumors. 30 This study identified a patient with malignant paraganglioma who carried the SDHD germline mutation. The patient had bilateral carotid body tumors with a familial onset. At present, the remaining patients with paraganglioma in the family have not had malignant changes and continue to be closely followed up.
The ataxia telangiectasia and Rad3-related (ATR) checkpoint kinase 1 pathway plays an essential role in suppressing replication stress from DNA damage and oncogene activation. 31 ATR kinase phosphorylates BRCA1, CHK1, BLM, p53, and other DNA damage response factors to inhibit cell cycle progression and ensure genome maintenance. 32 Several studies have shown that selective ATP-competitive inhibitors of ATR kinase enhance the antitumor effects of multiple DNA-damaging agents, including radiation and multiple chemotherapy drugs. 33 -35 ATR inhibitors either used as a monotherapy or in combination with DNA-damaging chemotherapy drugs are being tested in early-phase clinical trials in advanced solid tumors and hematological malignancies. 31 In addition, the mitogen-activated protein kinase 13 (MAP3K13) gene, also known as leucine zipper-bearing kinase (LZK), is a member of the serine/threonine protein kinase family and regulates the NF-κB, JNK, and mutant p53 pathways, which play an important role in tumorigenesis. 36 In 2017, Zoe et al demonstrated that MAP3K13 promotes proliferation in HNSCC by maintaining the expression of stabilized mutant p53. Silencing MAP3K13 reduced the viability and proliferation of head and neck squamous cell carcinoma cells. Therefore, MAP3K13 may represent a drug target for a subset of these patients who have MAP3K13 amplification. 37 This study reported for the first time that patients with malignant paraganglioma carry ATR and MAP3K13 gene mutations, which might further reveal the mechanism of paraganglioma malignancy, as well as new therapeutic biomarkers. However, the concrete mechanism deserves further investigation.
Limitations
The authors acknowledge that this study has several limitations. Due to the low incidence of head and neck malignant paraganglioma, the sample size in this study was small, and it needs to be analyzed in conjunction with similar studies to reveal the optimal treatment strategy. Moreover, owing to the slow progression of paraganglioma, the follow-up time for some cases needs to be increased to evaluate the long-term effects of the treatment.
Conclusion
After comprehensive treatment, patients with malignant paragangliomas in the head and neck can attain a favorable prognosis. Genetic mutations are commonly detected in patients with malignant paragangliomas. This study also identified mutations in ATR and MAP3K13 in these patients.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.