
Abstract
Keywords
Introduction
Behçet’s disease is a systemic inflammatory disorder characterized by recurrent oral and genital ulcerations, relapsing uveitis, and systemic vasculitis involving arteries and veins of all sizes. 1 The disease has a unique geographical distribution, with the highest incidence in the Middle East and East Asia. 2 Although the causes and pathogenesis of Behçet disease remain unknown, the disease is believed to be triggered by exposure to an infectious or other external agent in genetically predisposed people. 3
Sudden sensorineural hearing loss (SSNHL) is a rapid hearing loss of 30 dB at 3 contiguous frequencies within 3 days. The incidence of SSNHL is 5 to 20 per 100 000 persons per year. 4 The etiology of SSNHL can be confirmed in only 10% to 15% of cases, however, and the remaining cases are categorized as idiopathic. Potential pathoetiologies of idiopathic SSNHL include viral infection, vascular disturbance, stress-mediated response, inner ear membrane rupture, and immune-mediated disease. 5
Considering the immunologic mechanisms underlying SSNHL etiology and Behçet’s disease being one of the autoimmune diseases, several case series of sensorineural hearing loss (SNHL) in patients with Behçet disease, including a few cases of SSNHL, have been reported. 6 -9 Currently, no evidence-based treatment is available for SSNHL; steroids are clinically recommended. 10 However, approximately one-third of patients with SSNHL recover no hearing improvement after steroid administration, and alternative treatments such as intratympanic steroid injection (ITSI), hyperbaric oxygen therapy (HBOT), and acupuncture may improve prognosis.
We present a case of Behçet disease accompanying bilateral SSNHL, which was successfully treated using combined modalities; we also review relevant literature.
Case report
A 21-year-old man with Behçet disease since childhood presented to our clinic with a 10-day history of bilateral SSNHL. He had a history of bilateral uveitis as well as recurrent oral and genital aphthae. At a rheumatology/immunology and allergy department, he had been receiving prednisolone (5 mg/d), low-dose weekly methotrexate, and supplements of folic acid. Otoscopic examination results were normal. Initial audiometric testing revealed severe to profound SNHL with a pure-tone average (.5, 1, 2, and 4 kHz) of 90 dB in the right ear and 70 dB in the left ear (Figure 1A). His sound recognition threshold was 100 dB in the right ear and 45 dB in the left ear. Tympanometry results were normal. The patient exhibited no other symptoms of Behçet disease, such as oral or genital ulcers, arthralgia, skin lesions, or abdominal pain. Routine laboratory tests revealed that his blood cell counts, liver and renal function, c-reactive protein count, and erythrocyte sedimentation rate were within the normal ranges. Magnetic resonance imaging of the brain found nothing abnormal. The patient was started on oral prednisolone therapy (1.0 mg/kg daily) as well as 3 ITSIs in each ear every other day. The ITSIs were .8 mL of 4 mg/mL betamethasone administered through the anterior inferior quadrant of the tympanic membrane. The oral corticosteroid was tapered over a period of 21 days (prednisone at 40 mg/d for 3 days, 30 mg/d for 4 days, and finally 10 mg every 7 days). Acupuncture and HBOT were introduced alongside the pharmacotherapy. Acupuncture was performed 3 times a week, and each treatment session lasted 30 minutes. HBOT consisted of 3 courses of 60-minute daily exposure to 100% oxygen at 2.5 atmospheres absolute on weekdays and rest on weekends. After pharmacological treatment and 5 sessions of HBOT, the patient’s hearing improved. After 15 sessions of HBOT, the patient had significant hearing improvement in the left ear (more than 20 dB) and slight improvement in the right ear (10 dB) as shown in Figure 1B. At a 3-month follow-up, his hearing was stable, and his speech recognition had improved. (A) Audiometric results before treatment showed pure-tone average (.5, 1, 2, and 4 kHz) of 90 dB in the right ear and 70 dB in the left ear. (B) Audiometric results after treatment showed partial improvement of more than 20 dB in the left ear and 10 dB in the right ear.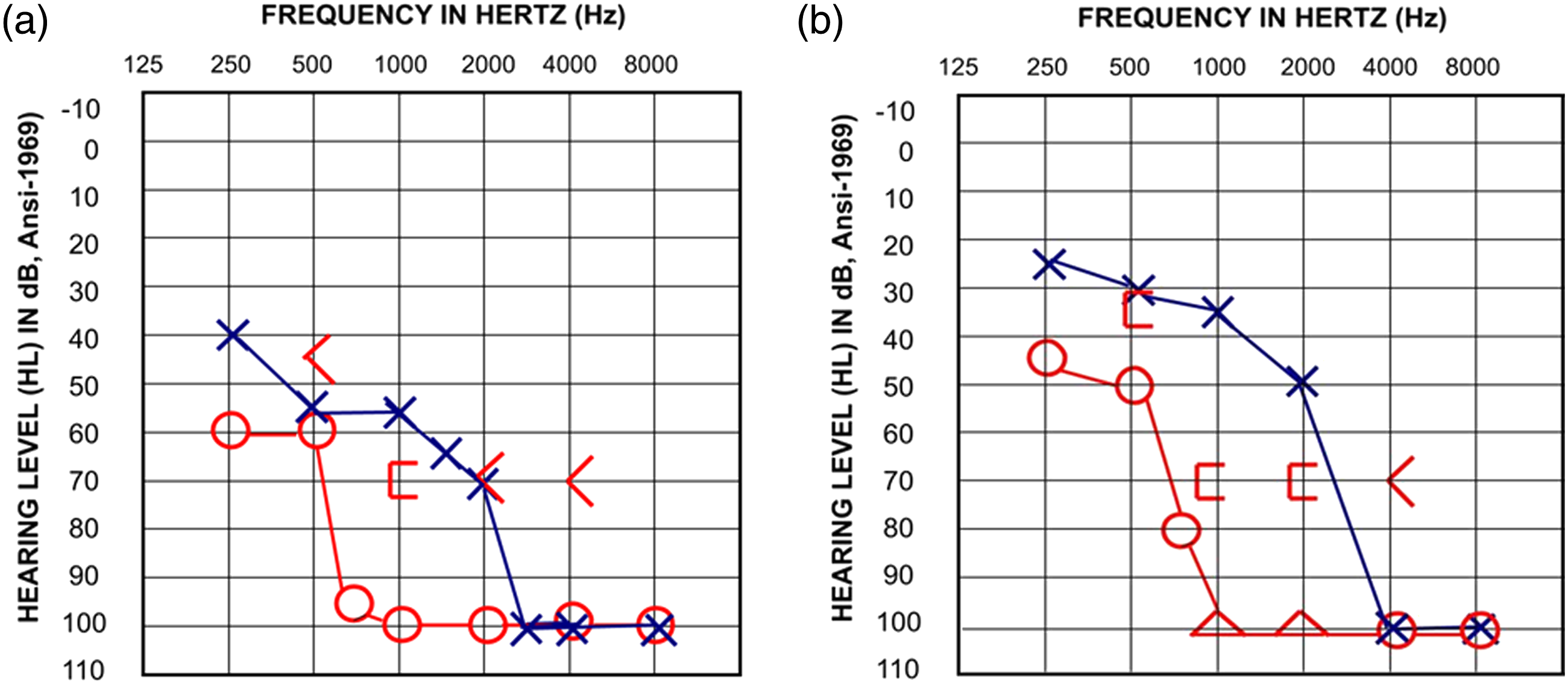
Discussion
The etiology of most SSNHL cases is unclear, but immune-mediated mechanisms are thought to be involved because vasculitis may result in vascular deposition of immunoglobulins and decreased perfusion of the cochlea. 11 Our literature review indicates that SNHL is common in patients with Behçet disease, in which it significantly affects high-frequency hearing, especially that of older patients. 12 -15
Summary of previously reported cases of Behçet disease with SSNHL.
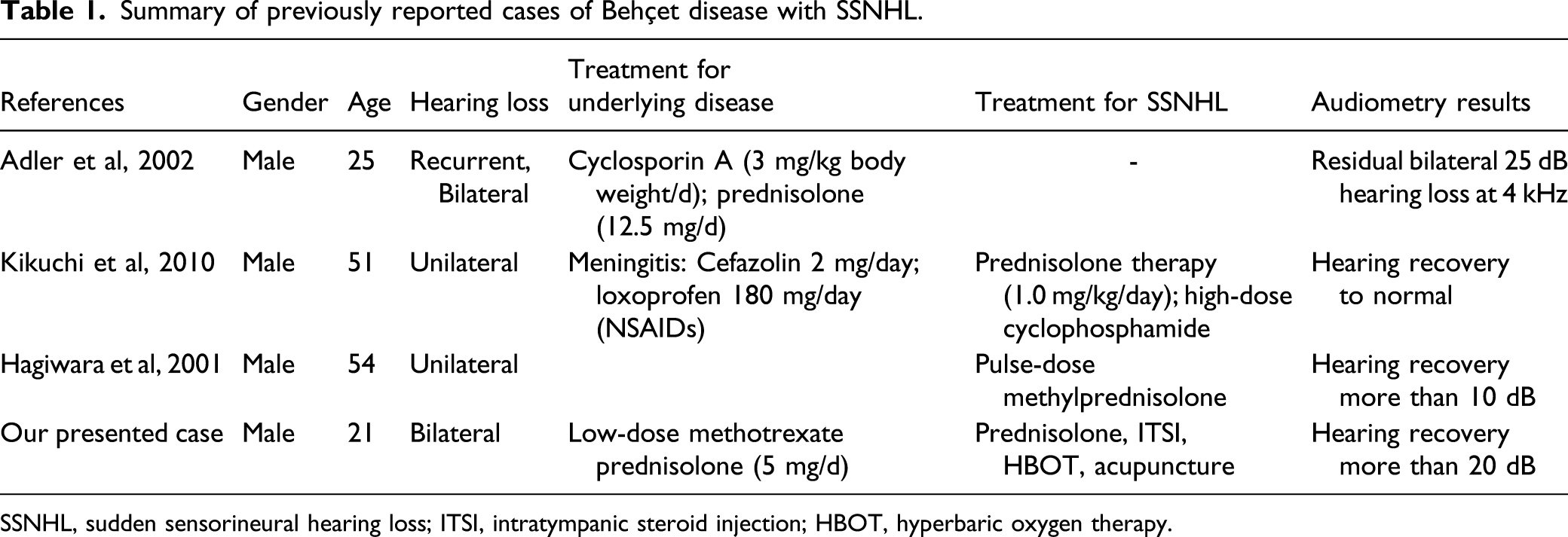
SSNHL, sudden sensorineural hearing loss; ITSI, intratympanic steroid injection; HBOT, hyperbaric oxygen therapy.
Currently, no evidence-based treatment for SSNHL is available, and a tapered course of systemic steroids is clinically recommended. 10 Additional treatments include local ITSI administered concurrently or sequentially and a combination of both with HBOT. 16 -19 Acupuncture also plays an important role in alternative treatment, but few data on its efficacy are available. 20
Although systemic glucocorticoids are considered the standard therapy for idiopathic SSNHL, evidence is lacking that supports their efficacy for hearing recovery in autoimmune disease alone or with simultaneous SSNHL. Regular administration of prednisolone in our patient over the several years was not able to prevent acute hearing loss. Similar results were reported by Adler et al, 7 who unsuccessfully treated patients with Behçet diseases and sudden hearing loss with immunosuppressive agents including prednisolone, azathioprine, and cyclosporine A. Therefore, alternative therapies must be developed.
A recent study reported the benefits of combined acupuncture, HBOT, and conventional steroid therapy for treating SSNHL. 21 The cochlea is sensitive to hypoxia. HBOT can increase perilymphatic oxygen tension, which promotes the delivery of oxygen to the cochlea and reduces inflammation. Acupuncture can promote blood flow to the ear, enhance auditory nerve conduction, and increase oxygen delivery to the cochlea. 19,22,23
Our case demonstrates the benefits of combined steroid-HBOT-acupuncture therapy for promoting microcirculation in Behçet disease with SSNHL.
Intratympanic steroid injections to the inner ear are believed to provide more targeted relief by approaching the round window through an optimal route. Intratympanic steroid injections may provide a greater likelihood of high-frequency hearing recovery than of low-frequency recovery because of the increased absorption of dexamethasone in the base of the scala tympani. 24 Although our patient’s high-frequency (4 or 8 kHz) hearing remained poor after combined ITSI and systemic steroid therapy, this may be due to previous high-tone SNHL, which is expected in patients with Behçet disease. 12 -15
Adjuvant HBOT used with immunosuppressive agents has benefits for treating autoimmune conditions including perianal fistulas in Crohn’s disease, systemic scleroderma, and lupus-prone autoimmunity in mice. 25 -27 Therefore, HBOT, alone or combined with acupuncture, may provide benefits by reducing inflammation and promoting oxygen delivery to damaged tissues; thus, it can be considered for patients with autoimmune diseases and associated complications as an adjunctive treatment to standard immunosuppressive agents.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by Tri-Service General Hospital, Grant Number TSGH-D-110081.
Informed consent
The corresponding author has obtained written informed consent that the patient provides patient information to be published.
Data availability
The data presented in this study are available on request from the corresponding author.