
Abstract

Significance Statement
We reported a patient with congenital malleus bar fixing to external auditory canal (EAC) and causing a long-term conductive hearing loss (CHL), which was promptly diagnosed and treated. This anomaly depicted on high-resolution computed tomography (HRCT) is challenging to both of radiologist and otologist. Clinically, the potassium titanyl phosphate (KTP) laser is a useful and safe technique to release this bony fixation.
A 12-year-old girl presented with a left hearing loss for 5 years. The pure tone audiogram (PTA) displayed a left CHL with air conduction (AC) of mean 52.5 dB hearing level (dB HL) at 0.5k, 1k, 2k, 4k with a mean air bone gap (ABG) of 46.25 dB HL. The high-resolution computed tomography (HRCT) of temporal bone was arranged.
A bony spur-like process from EAC on axial view was noted (Figure 1A). On coronal view, this bony process fixed the neck of malleus and EAC (Figure 1B). Otherwise, no other anomaly was found on the CT. (A). A bony spur-like process (arrowhead) from external auditory canal is noted on axial view. (B). The bony bar fixed to the neck of malleus (arrow) is found on coronal view. (Asterisk, head of malleus).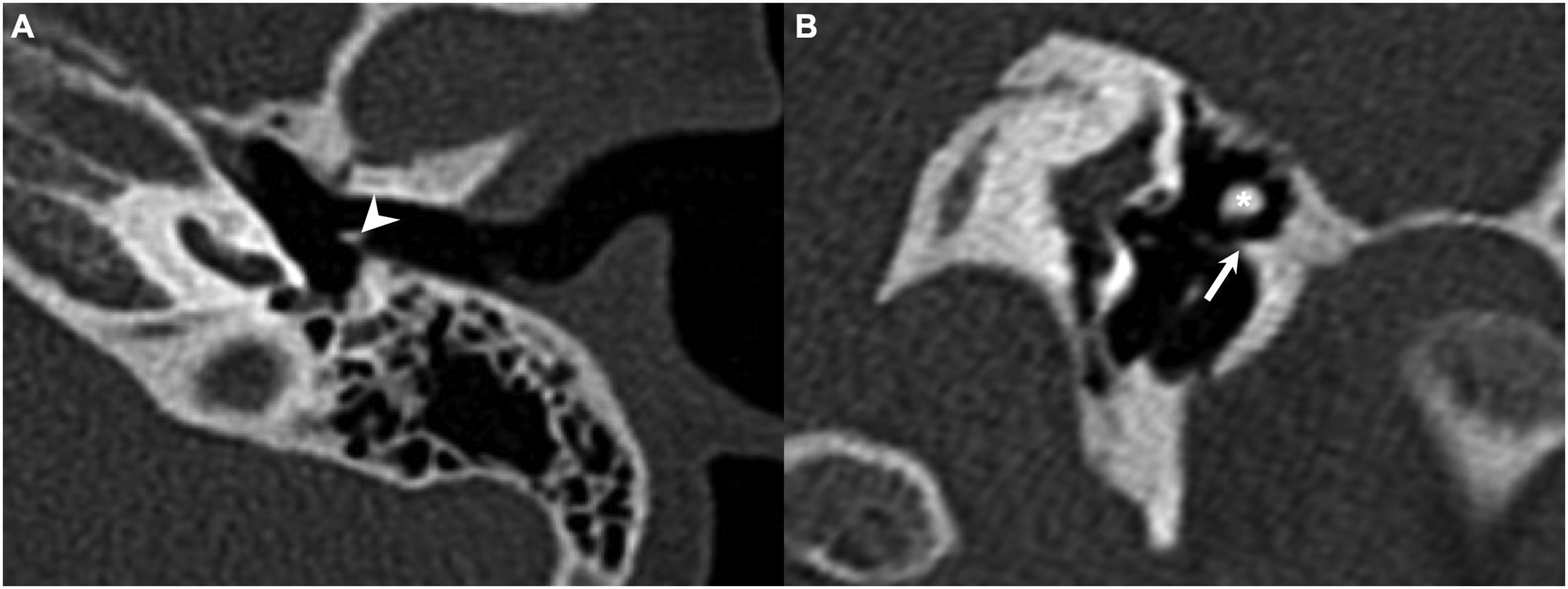
The diagnosis of congenital malleus bar fixing to EAC causing CHL was impressed. Via endaural approach, an exploratory tympanotomy with potassium titanyl phosphate (KTP) laser was performed to release the bony bar (Figure 2). The mobility of the ossicular chain was repaired without complication occurring postoperatively. The PTA displayed left AC recovering to mean 21.25 dB HL with a mean ABG of 15 dB HL on postoperative 2 years. (A). The bony bar (arrowhead) fixes from external auditory canal to neck of malleus. (Asterisk, head of malleus).
Congenital malleus bar was first described by Nomura et al. 1 for a bony bar fixing from the posterior EAC to malleus neck. A bony fixation of the malleus is an uncommon cause of CHL. 2 Based on Subotic et al., the incidence of isolated bony fixation of the malleus is around 1.4%. It could be caused by developmental anomaly, trauma, chronic infection of the ear, or otosclerosis according to different theories. 3
The congenital malleus bar usually leads to CHL, which might be due to ossicular chain fixation or discontinuity. A CHL in the range of 40-60 dB HL with a normal eardrum but no deteriorating hearing by degrees is suggestive of a congenital ossicular malformation. 4 The preoperative fine-cut HRCT is helpful to identify the whole bony bar. However, because only the tiny anomaly could be depicted on CT, the recognition of this illness is challenging to both radiologist and otologist.
For the surgery, a congenital malleus bar could be directly severed or removed via a microcurette with dexamethasone injection. 2,5 To our patient, we utilized KTP laser to release the bar for more delicate surgical process and less complication occurrence. A great hearing outcome was obtained postoperatively.
Here, we reported a patient of congenital malleus bar causing CHL. Although very rare, this congenital disease should be considered in the differential diagnosis of long-term CHL. Through CT images and clinical pictures, this article is helpful for clinician to have a correct diagnosis of this disease.
Footnotes
Acknowledgments
The authors thank all of the members of Department of Otorhinolaryngology-Head and Neck Surgery, Chang Gung Memorial Hospital, Linkou.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Statement of Ethics
Written informed consent was obtained from the patient for publication and any associated images. Approval of this case study was obtained from the Institutional Review Board (IRB) of Chang Gung medical foundation. (IRB No.202101503B0).