
Abstract
Objectives
The pandemic has affected over 182 million coronavirus disease 2019 (COVID-19) cases worldwide. Accumulated evidence indicates that anosmia is one of the significant characteristics of COVID-19 with a high prevalence. However, many aspects of COVID-19-induced anosmia are still far from being fully understood. The purpose of this review is to summarize recent developments in COVID-19-induced anosmia to increase awareness of the condition.
Methods
A literature search was carried out using the PubMed, Embase, Web of Science, and Scopus. We reviewed the latest literature on COVID-19-induced anosmia, including mechanisms of pathogenesis, olfactory testing, anosmia as predictive tool, pathological examinations, imaging findings, affected factors, co-existing diseases, treatments, prognosis, hypothesis theories, and future directions.
Results
The possible pathogenesis of COVID-19-induced anosmia may involve inflammation of the olfactory clefts and damage to the olfactory epithelium or olfactory central nervous system by severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2). The D614G spike variant may also play a role in the increased number of anosmia patients. Anosmia may also be an essential indicator of COVID-19 spread and an early indicator of the effectiveness of political decisions. The occurrence and development of COVID-19-induced anosmia may be influenced by smoking behaviors and underlying diseases such as type 2 diabetes, gastroesophageal disorders, and rhinitis. Most patients with COVID-19-induced anosmia can fully or partially recover their olfactory function for varying durations. COVID-19-induced anosmia can be treated with various approaches such as glucocorticoids and olfactory training.
Conclusion
Anosmia is one of the main features of COVID-19 and the underlying disease of the patient may also influence its occurrence and development. The possible pathogenesis of COVID-19-induced anosmia is very complicated, which may involve inflammation of the olfactory clefts and damage to the olfactory epithelium or olfactory central nervous system.
Introduction
Coronavirus disease 2019 (COVID-19) is an emerging infectious disease caused by the severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) and characterized by fever or chills, cough, shortness of breath or difficulty breathing, fatigue, muscle or body aches, headache, new loss of taste or smell, sore throat, congestion or runny nose, nausea or vomiting, and diarrhea. 1 The COVID pandemic has wreaked havoc on many countries around the world. As of July 2, 2021, over 182 million COVID-19 cases and over 3.95 million deaths have been reported cumulatively globally. 2 As of June 30, 2021, a total of 2,950,104,812 vaccine doses have been administered worldwide. 2 Although large-scale vaccination is speeding up, many new SARS-CoV-2 variants threatening to circumvent the vaccines and existing natural immunity will continue to affect the COVID-19 pandemic. 3
Anosmia refers to the loss of olfactory function (OF), and its common causes include nasal disorders, head trauma, and infections. 4 The pathophysiology of post-infectious anosmia is unclear, but it is thought to involve olfactory neuroepithelium destruction or direct pathogen transmission to the brain through the olfactory nerve. 5 SARS-CoV-2 infection also triggered anosmia, a COVID-19 marker, known as COVID-19-induced anosmia. 4 Anosmia had approximately 62% prevalence in patients who tested positive for COVID-19. 6 Females and young people were more prone to develop COVID-19-induced anosmia. 7,8 COVID-19-induced anosmia was also associated with significant ethnic differences, with the prevalence being 3 folds higher in Caucasians than in Asians. 9 With the growing number of COVID-19 patients, the number of patients suffering from COVID-19-induced anosmia increases. COVID-19-induced anosmia will remain one of the most common disorders in the otolaryngology department for some time to come. 10
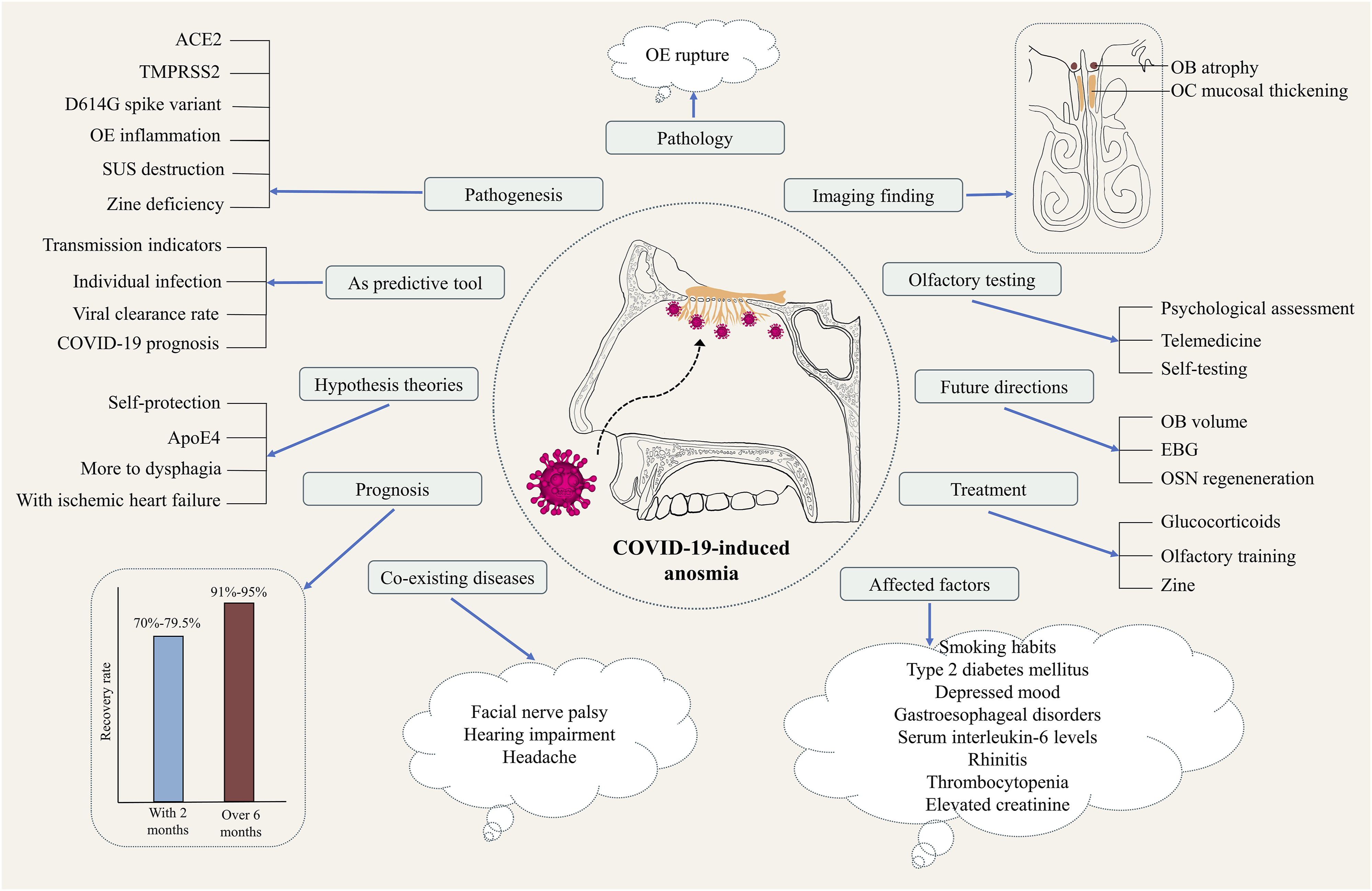
Studies on COVID-19-induced anosmia have boomed over the past year; however, many aspects of COVID-19-induced anosmia remain far from being completely understood. Therefore, we endeavored to produce a narrative review to improve our understanding of COVID-19-induced anosmia. We searched literature databases, including PubMed, Embase, Web of Science, and Scopus, using variations of the descriptors such as COVID-19, SARS-CoV-2, and anosmia. Inclusion criteria were the literature on COVID-19-induced anosmia published in English since the outbreak of COVID-19. We screened the title and abstract of all retrieved records for potential relevance. We excluded non-relevant topic studies, non-English articles, and unavailable full-text articles. A flowchart of the literature search process is presented in Figure 1. Here, we highlight recent advances related to COVID-19-induced anosmia, including mechanisms of pathogenesis, olfactory testing, anosmia as predictive tool, pathological examinations, imaging findings, affected factors, co-existing diseases, treatments, prognosis, hypothesis theories, and future directions (Figure 2). Flowchart showing the process of literature screening. Schematic diagram summarizing the main points about COVID-19-induced anosmia. COVID-19: Coronavirus disease 2019; ACE2: Angiotensin-converting enzyme 2; TMPRSS2: Transmembrane serine protease 2; OE: Olfactory epithelium; SUS: Sustentacular cell; ApoE4: E4 allele of apolipoprotein E; OSN: Olfactory sensory neurous; EBG: Electrobulbogram; OB: Olfactory bulb.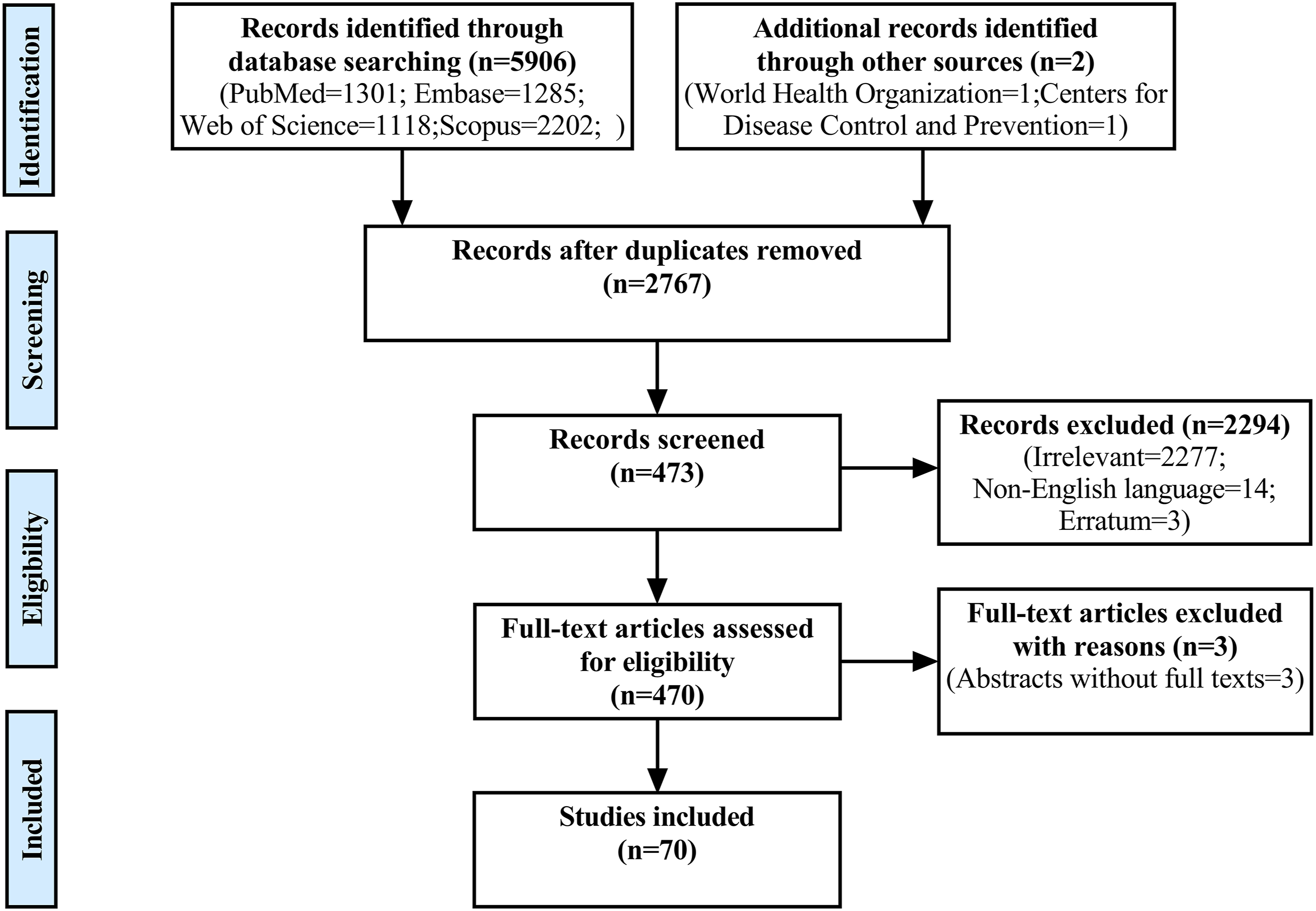
Mechanisms of Pathogenesis
The underlying mechanisms of COVID-19-induced anosmia remain controversial and not fully understood. 11 It is well known that the SARS-CoV-2 virus invades human cells via the angiotensin-converting enzyme 2 (ACE2) and triggers the transmembrane serine protease 2 (TMPRSS2), which promotes virus uptake. 12 Cells with high ACE2 and TMPRSS2 expression have a potent virus binding ability and are susceptible to virus infection. 12 ACE2 and TMPRSS2 can be found in the sustentacular cells (SUSs) and glandular cells of the olfactory epithelium (OE), which provides anatomical evidences for the expression of ACE2 and TMPRSS2 in the OE and olfactory bulb (OB) of the human. 13
The D614G spike variant may be partly responsible for the increased number of patients with chemosensory dysfunction. 9,14 It is an essential viral genetic factor promoting chemosensory epithelial cell infection and may function with unknown host factors to increase smell and taste damage. 14 It is more common in Europe and the Americas, contributing to a higher prevalence of chemosensory dysfunction in these areas. 9,14
Direct inflammation of the OE may play a role in COVID-19-induced anosmia. 11,15 Tumor necrosis factor α (TNF-α) is one of the most potent and relevant inflammatory mediators in nasal mucosal inflammatory diseases. 16 In the OE of COVID-19 patients, elevated pro-inflammatory cytokine TNF-α was found. 15 A prospective study has shown that patients with COVID-19-induced anosmia had nasal inflammation that lasted up to 5 months, compared to patients with COVID without anosmia and healthy individuals. 11
The reduction of nutrients around the olfactory cilia can impair olfactory activity in COVID-19 patients as the reduction of energy available to the cilia will disrupt the odor transmission process. 17 A meta-analysis showed that a subset of SUS, rich in cytoskeletal regulatory proteins, is the most susceptible cell type to SARS-CoV-2 infection. 18 In COVID-19 patients, compromised abundance or cellular activity of SUSs, olfactory stem cells, and Bowman’s gland cells of the olfactory epithelium are the most likely causes of anosmia. 18 The SUSs contribute to the metabolism of olfactory neurons by releasing glucose into the mucus of the cilia. 17 SUSs had a higher level of ACE2 expression in the OE. 19 The death of SUSs disrupts the metabolic processes of olfactory neurons, which might cause OD. 17
Zinc deficiency is believed to be linked to anosmia in COVID-19 patients. 20 Anosmia may be an adaptive response of COVID-19 to reduce nasopharyngeal zinc, eventually leading to a decrease in the essential ACE2 receptor that binds SARS-CoV-2. 20 The reduced local zinc response might also be responsible for the reduced severity of COVID-19. 20 However, another study suggested that zinc might not affect anosmia in COVID-19 patients. 21 Nonetheless, zinc therapy significantly shortened the time to recover from anosmia without affecting the overall recovery time of the COVID-19. 21
Olfactory Testing
Because of its limited correlation with objective olfactory testing, the self-assessment of OF by the patient was unreliable. 22 Psychological assessment involves the response of the patient to stimuli such as odor and taste. The olfactory psychophysical assessment usually includes test items such as odor threshold, odor discrimination, and odor identification, which are definitively objective tests. 22
Telemedicine reduces cross-infection during the COVID-19 outbreak and prevents and manages epidemics following the COVID-19 pandemic. 23,24 Telemedicine also allows safe and timely capture of the OF data of self-isolated COVID-19 patients. 22 A study of a group of COVID-19 skiers who underwent telemedicine quantitative olfactory testing for four consecutive weeks showed these patients could complete full Sniffin’ Sticks Test (SST), visual analog scales, and questionnaires by themselves in the quarantine situation. 25 Alternatively, there is an easier way to perform a telemedicine olfactory test at home. The method employed some common household odors for odor discrimination testing and solutions with increasing denatured ethyl alcohol dilutions for olfactory threshold testing. 26
Individuals can select familiar odorous items from their daily life to employ as odorants in their homes for self-testing. 27 In addition, participants can also measure olfactory perception by rating possible household odorants with a real-time online tool. 28
Nowadays, the application of large-scale olfactory tests for COVID-19 is still limited. 29 Some patients with COVID-19-induced anosmia self-reported normal olfaction; however, the psychophysical olfactory evaluation revealed mild anosmia. 30 Therefore, long-term follow-up and regular olfactory tests are necessary for patients with COVID-19-induced anosmia.
Anosmia as Predictive Tool
Anosmia is the strongest predictor of COVID-19. 6 The specificity and sensitivity of the symptom of anosmia for the diagnosis of COVID-19 were 97% and 65%, respectively, and the positive and negative predictive values were 63% and 97%, respectively. 31 Anosmia should be recognized as an early manifestation in diagnosing COVID-19 and should be tested regularly.
The increased incidence of sudden olfactory changes in the general population may also serve as an essential indicator of the spread of COVID-19 in the population. It was also an early signal of the effectiveness of political decision-making, predating the prevailing government indicators. 32 A study conducted in France, Italy, and the United Kingdom found positive correlations between the self-reports of sudden smell and taste changes and the pressure indicators of the hospital, such as COVID-related hospitalizations, critical care resuscitation unit admissions, and mortality rates. 32 Creating a uniform internet-based self-reporting system for new cases of sudden OD would help in screening and combating the COVID-19 pandemic. 33
An online olfactory tool for 12,020 participants from 134 countries indicated that their olfactory ratings were significantly correlated with the national COVID-19 infection rate in their countries over time. 28 Additionally, this real-time online tool showed considerable suggestive power at the individual level, with a sensitivity of 90% and specificity of 80%. 28
There was an independent and significant correlation between the viral clearance rate and the SST scores in COVID-19-induced anosmia patients, with a sensitivity of 79% and specificity of 87% (AUC = .883) for predicting viral clearance when the SST was >10.5. 34 Olfactory and gustatory dysfunctions were also associated with the prognosis of COVID-19 and were negatively associated with mortality in patients with an odds ratio of .26 (.15–.44). 35
Pathological Examinations
Two studies have been conducted to examine the pathological features of the OE and nasal mucosa of COVID-19 patients with anosmia, respectively. 36,37 Vaira et al. 36 performed an OE biopsy on a 63-year-old female patient who presented with anosmia for over 3 months following SARS-CoV-2 infection. The biopsy showed that the OE had a significant rupture, indicating that the lesion was in the epithelium itself. Biopsy and immunohistochemical analysis of the nasal mucosa of COVID-19-induced anosmia patients showed mild inflammatory changes with scattered SARS-CoV-2 nucleoprotein-positive cells in the stroma. 37 Mucosal infiltration of CD68+ macrophages expressing SARS-CoV-2 antigens may be involved in OD. 37
Another research studied the effect of SARS-CoV-2 on the olfactory system of the hamster and found that the OE was severely impaired, leading to a substantial loss of cilia required for olfactory detection. 38 Anosmia in COVID-19 patients may be related to olfactory epithelial desquamation and immune cell recruitment. 38
Some studies have also examined the olfactory system pathology in cadavers of patients who died from COVID-19. Morbini et al. 39 performed minimally invasive dissection of the olfactory complex on two corpses. Transmission electron microscopy revealed that 80 nm to 100 nm viral particles were presented on the cell membrane of ciliated respiratory cells of the olfactory mucosa in one patient, and intracytoplasmic viral inclusion bodies and interstitial virus particles were presented in the OB of another patient. Another post-mortem histological study showed the focal atrophy of the mucosa and the distinct leukocytic infiltration of the OE. 40 Digestive chambers with positive immunohistochemistry CD68 staining have been identified in olfactory nerve fibers, suggesting axonal damage. 40 The multifocal microvascular injury was also detected in the cadaver’s OBs, with no signs of SARS-CoV-2 infection. 41 Passive diffusion and axonal transport passing through the olfactory complex is likely to be the main pathway for SARS-CoV-2 access to the central nervous system (CNS). 39
Imaging Findings
OB atrophy is a typical imaging finding in COVID-19-induced anosmia patients. A case–control study found that the bilateral OB height was significantly lower in patients with COVID-19-induced anosmia than in age- and sex-matched healthy controls in MRI images, suggesting mild-to-moderate OB atrophy in 88% of patients. 42 The OB volume of a 19-year-old female with COVID-19-induced anosmia was 29.96 mm3 and 35.51 mm3 in MRI images after about 2 months, compared to 49.5 mm3 and 47.46 mm3 3 years ago, respectively, which were significantly shrunken compared to the pre-onset period. 43 This case report confirmed the possibility of OB atrophy in the COVID-19-induced anosmia patient by comparing the OB volume before and after the onset of the disease.
The presence or absence of mucosal thickening and edema in the olfactory clefts (OCs) area on imaging remains controversial. A prospective, single-center, case–control study of 20 COVID-19-induced anosmia patients who underwent MRI examination during the early stage of the disease revealed complete obstruction of the OCs in 19 cases, while age-matched healthy controls had no block of the OCs. 44 Following a follow-up month, as the olfactory scores (OSs) improved, the MRI displayed only seven cases with the OCs’ obstruction. 44 The OS was positively correlated with the absence of OCs’ obstruction. 44 A paranasal sinus computed tomography study of 49 patients with COVID-19-induced anosmia found no abnormal changes in the mucosa or OCs, implying that the anosmia conduction system does not appear to play an essential role in this process. 45 Another study came to a similar conclusion. 46 Since no significant mucosal inflammatory changes were detected in the OCs area, the effectiveness of steroid therapy is questionable in these patients. 45 A single-center retrospective cross-sectional study found that 25.4% of COVID-19 patients without anosmia had mucosal thickening of the OCs in CT images. 47
Affected Factors
The occurrence and development of COVID-19-induced anosmia are associated with a variety of factors. These factors included smoking habits, 35 type 2 diabetes mellitus, 48 depressed mood, 49 anxiety, 49 gastroesophageal disorders, 50 serum interleukin-6 levels, 51,52 rhinitis, 53 thrombocytopenia, 53 and elevated creatinine. 53 The high prevalence of anosmia in COVID-19 patients with smoking habits may be related to the fact that tobacco causes more severe damage to OE cells. 35 Reduced first-line defense of nasal immunity in type 2 diabetes mellitus patients increased SARS-CoV-2 susceptibility in the nasal cavity with the unknown cause. 48 The severities of olfactory and gustatory loss was associated with depressed mood and anxiety, indicating that emotional dysfunction may be a symptom of the CNS in COVID-19 patients since SARS-CoV-2 can invade the CNS through the olfactory pathway. 49
Co-Existing Diseases
OD in COVID-19 patients can also co-exist with other diseases. Homma et al. 54 reported a case of a 35-year-old Japanese female COVID-19 patient with concomitant OD and facial nerve palsy. It was speculated that SARS-CoV-2 had induced peripheral neuropathy of the facial and olfactory nerves via the upper respiratory tract. Jacob et al. 55 described a 61-year-old woman with simultaneous anosmia, ageusia, and hearing impairment after SARS-CoV-2 infection, suggesting that clinicians need to be aware of this triadic association. A cross-sectional study found that COVID-19 patients presenting with OD and ageusia had a much higher incidence of headaches than those without these symptoms. 56 Headache was strongly associated with OD and ageusia. 56 These cases exhibited the diversity of clinical features of SARS-CoV-2 infection.
Treatments
Various approaches have been attempted to treat COVID-19-induced anosmias, such as oral and intranasal glucocorticoids, olfactory training (OT), and zinc. A prospective, randomized, controlled study showed significant improvement in OSs in both the mometasone furoate nasal spray group and the OT group compared to pre-treatment. 57 However, there were no significant differences in duration of anosmia, OSs, and OD recovery rates between the two groups. 57 A multicenter randomized case–control study showed that COVID-19-induced anosmia patients in a combination treatment group using systemic prednisone and nasal irrigation, with betamethasone, rinazine, and ambroxol, and had significantly improved in OSs compared to those in the untreated control group. 58 Steroid-containing combination drugs may be an effective specific therapy. 58 A randomized case–control study found that the recovery time of olfactory and/or gustatory function was substantially shorter for COVID-19-induced anosmia patients treated with zinc than those who did not receive zinc treatment. 21
Although the exact mechanism of OT is unclear, studies have shown that repeated stimulation of olfactory neurons by clearly specified odorants can improve the regenerative capacity of the olfactory system and neuroplastic potential. 59 Patients were exposed to four odorous compounds (eucalyptol, phenyl ethyl alcohol, citronella oil, and eugenol) for 5 min and twice daily for 12 weeks or longer. 60 A pilot study investigated the effectiveness of oral glucocorticoids combined with OT in treating COVID-19-induced anosmia and showed that the OD of the patients improved significantly. 61 Another study showed that 70% of COVID-19-induced anosmia patients regained their normal olfactory function after 2 months of OT. 62 However, the sample size of these studies was too small, and further studies in a larger population sample are warranted to validate the findings. 61,62
Prognosis
OD caused by SARS-CoV-2 has a good overall recovery outcome. Headache, nasal congestion, and platelet count might be the specific predictors of the recovery from OF. 63 A prospective study conducted in Belgium found that full recovery of OF in 79.5% of patients with COVID-19-induced anosmia was possible within 2 months. 64 The OD severity correlated with olfactory loss duration and had a high predictive effect. 64 An animal study showed that the OEs of SARS-CoV-2-infected golden Syrian hamsters were severely damaged at 3 days post-infection and gradually recovered at days 5 and 10 post-infection. 65 COVID-19-induced anosmia is liable to be completely reversible. 65
Two studies have investigated the recovery of the OF in COVID-19 patients with more than half a year of follow-up. A multicenter study from Europe showed that OD disappeared in 95% of patients 6 months after onset. 66 A study from Italy investigated the recovery of smell in patients with COVID-19-induced anosmia by telephone interview 8 months following diagnosis and revealed that 91% of patients recovered their sense of smell, with 53% recovering fully. 67 In addition, the study found that women and younger patients appeared to be more likely to regain OF. 67
Hypothesis Theories
To resolve the topical issue, researchers have also proposed some hypotheses on the mechanism of COVID-19-induced anosmia.
Le Bon et al. hypothesized that COVID-19-induced anosmia might be triggered by olfactory receptor neurons cutting off the pathway of SARS-CoV-2 into the brain through immunomodulatory self-protection mechanisms. 68 Being associated with anosmia, the e4 allele of apolipoprotein E (ApoE4)is a risk factor for future dementia. 69 It is postulated that SARS-CoV-2 may be an increased risk factor for future dementia in COVID-19-induced anosmia patients with ApoE4. 69 The study showed that the severity of ischemic heart failure is closely correlated with OD. 70 Therefore, OD has been postulated as a predictive factor of myocardial injury in patients with COVID-19. 71 The swallowing mechanism of COVID-19 patients can also be adversely affected by functional defects in taste, smell, and pharyngeal sensation, making them more prone to dysphagia. 72
It is essential to note that the above theories are hypotheses and have not been clinically or experimentally confirmed.
Future Directions
The exact mechanisms of SARS-CoV-2 damage to the olfactory system remain not fully understood nowadays. 73 More studies should be conducted on olfactory mucosal pathology, dynamic changes in OB volume, electrobulbogram (EBG), and the regeneration of the olfactory sensory neurons. In-depth studies of human olfactory mucosa specimens will provide a comprehensive understanding of the interactions between SARS-CoV-2 neural invasion, immune response, apoptosis, and neurogenesis. 68 Magnetic resonance imaging studies of OB volume changes at different time points in COVID-19-induced anosmia patients can be performed, enabling clinicians to have a more accurate prognosis of olfactory outcomes. 43 EBG, a non-invasively recording signal from the human OB, is used both for olfactory-related translational work and as a daily clinical tool to detect pathology-related lesions in the central olfactory processing in humans. 74 To our knowledge, there are no studies of EBG for COVID-19-induced anosmia patients. OB signal changes in EBG may be helpful in the diagnosis and prognosis of anosmia in patients with COVID-19. The SARS-CoV-2 infection impairs the activity and function of olfactory neurons, and the regeneration of olfactory sensory neurons merits further investigation. 75
Conclusion
Anosmia is one of the principal features of COVID-19 with a high prevalence, and underlying diseases of patients may also influence its occurrence and development. The possible pathogenesis of COVID-19-induced anosmia is complicated and may involve inflammation of the OCs and damage to the OE or olfactory CNS by SARS-CoV-2. Most patients with COVID-19-induced anosmia can regain their sense of smell.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Soft Science Research Project of Science and Technology Association of Wuxi Municipality, China (grant number: KX-21-B64).