
Abstract
Rhabdomyomas are rare benign mesenchymal tumors of the skeletal muscles and uncommon in the head and neck region. Laryngeal rhabdomyomas are much rarer. We present the case of a 32-year-old woman who was admitted to our hospital for shortness of breath due to pneumothorax. As otolaryngologists, we were consulted for a soft tissue tumor over the left side of the larynx that was accidentally found on the chest computed tomography (CT). The patient underwent laryngomicrosurgery for tumor biopsy, and histological examination revealed a laryngeal rhabdomyoma. After the operation, magnetic resonance imaging of the neck was performed and the tumor was suspected as rhabdomyosarcoma. Positron emission tomography/computed tomography (PET/CT) showed an 18F-fluoro-2-deoxy-D-glucose (FDG)-avid soft tissue mass on the left side of the larynx. After complete tumor removal via transoral laser microsurgery, no recurrence was reported for 5 years.
Introduction
The rhabdomyoma is a rare benign mesenchymal tumor of the skeletal muscles and is classified into two subtypes: cardiac and extracardiac. Extracardiac rhabdomyoma can be subclassified into fetal, juvenile, and adult types, depending on both clinical and morphological examinations, instead of the patient age. 1 Rhabdomyomas in the head and neck area account for 70–93% of cases of adult-type rhabdomyoma, but laryngeal rhabdomyomas are much rarer, with only approximately 40 cases reported.1-3
Laryngeal rhabdomyomas can cause symptoms such as hoarseness, dysphagia, foreign body sensation, or shortness of breath, similar to other types of laryngeal tumors. Imaging findings usually imply a benign lesion owing to the submucosal location without invasion to the surrounding soft tissues. However, rhabdomyomas may mimic malignant tumors on computed tomography (CT) scans because of indistinct borders blending into adjacent isodense muscles. 4 The diagnosis is usually confirmed by histopathologic findings, and the primary treatment is surgical excision. 2
Case report
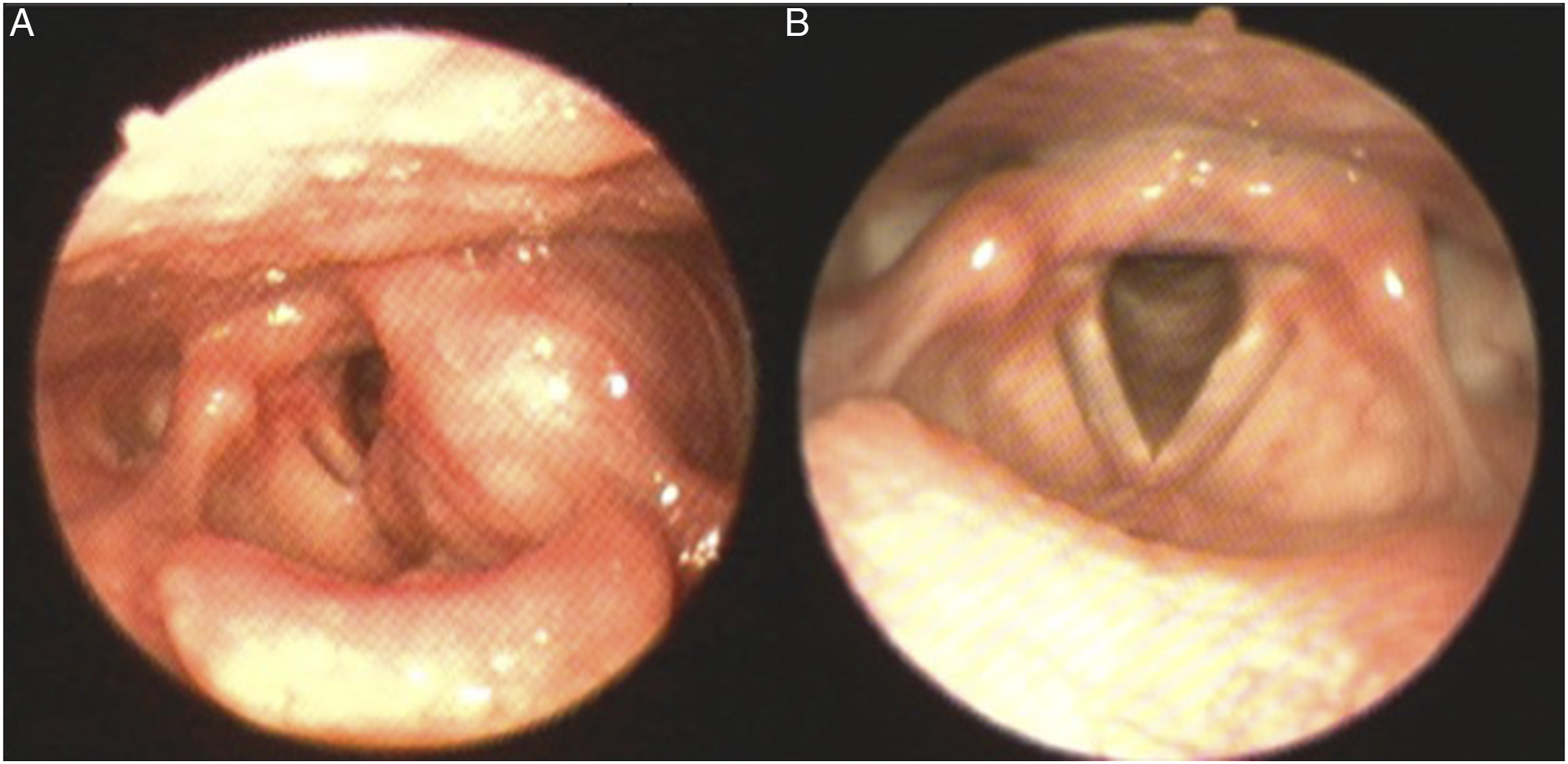
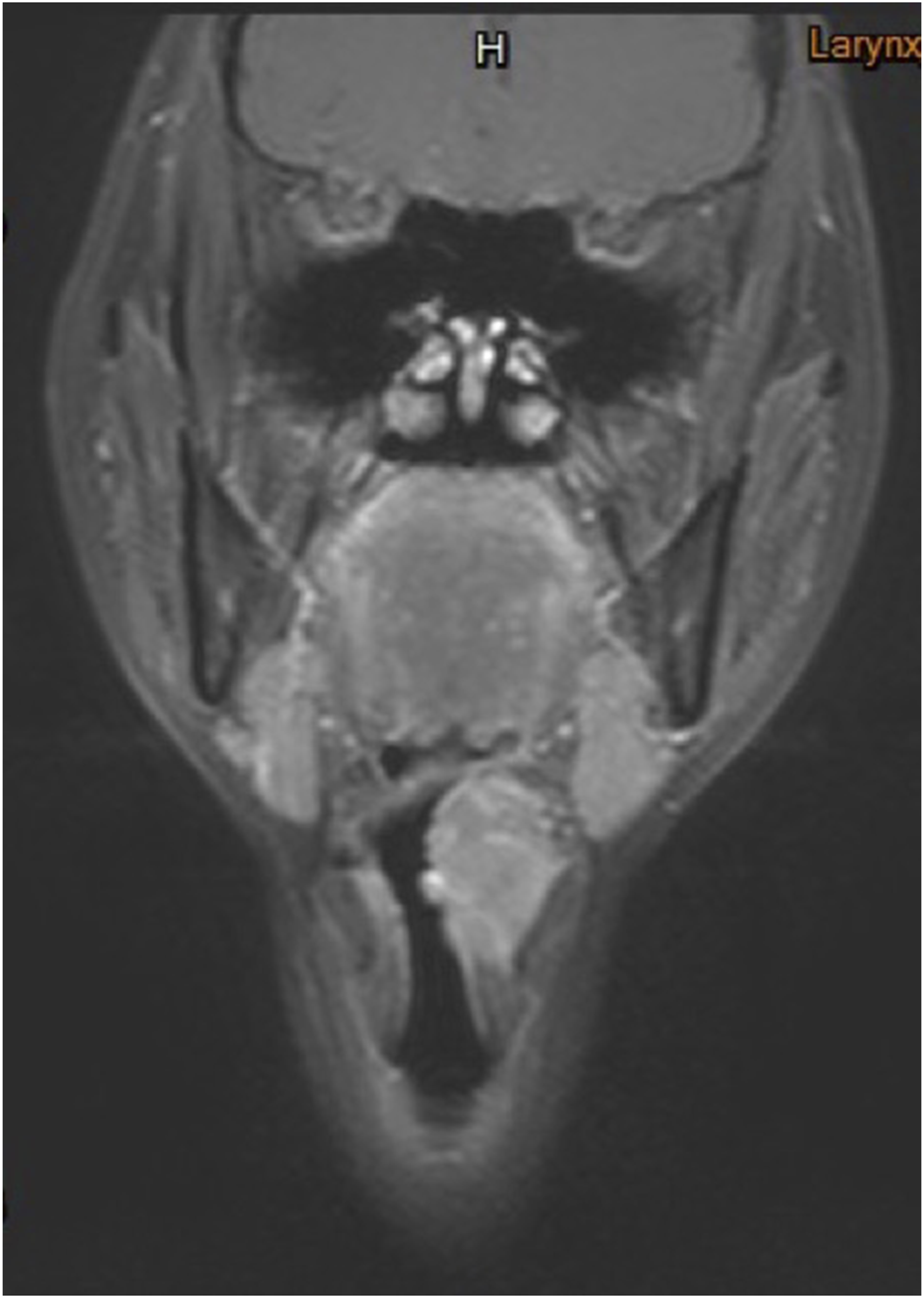
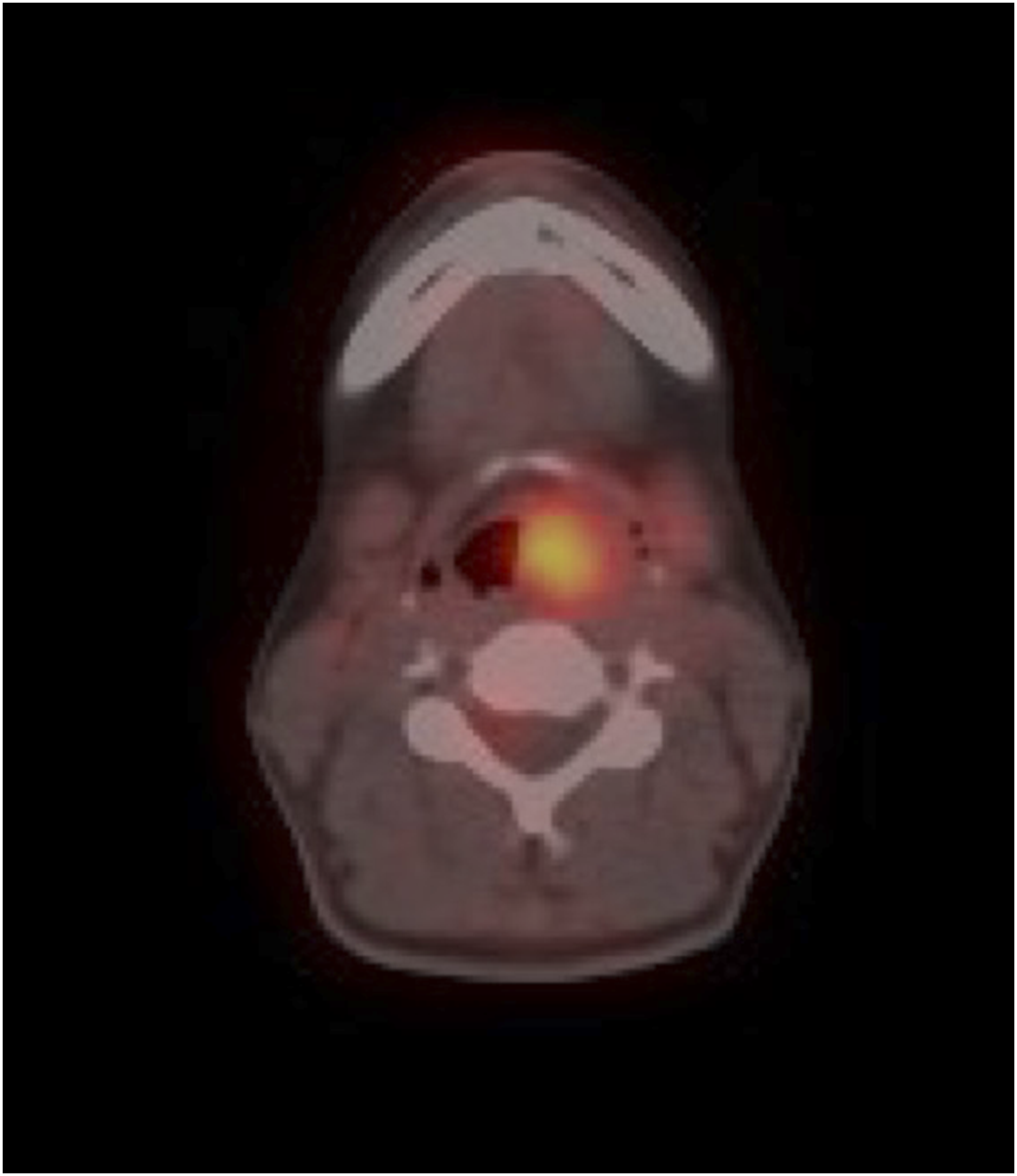
A 32-year-old woman without underlying disease was admitted to our hospital for shortness of breath due to pneumothorax. The Department of Otolaryngology-Head and Neck was consulted because a soft tissue tumor was accidentally found over the left side of the larynx on a non-enhanced chest CT examination (Figure 1). This patient also complained of hoarseness for approximately 1 year and denied cigarette smoking and alcohol use. Fiberoptic laryngoscopy revealed a submucosal tumor with a smooth surface beneath the aryepiglottic fold (Figure 2). The patient underwent laryngomicrosurgery for tumor biopsy, and the histologic examination revealed a laryngeal rhabdomyoma. After the operation, further imaging studies were performed to evaluate the precise extension of the tumor. The neck magnetic resonance imaging (MRI) showed an enhancing soft tissue mass with a maximal diameter of 3.3 cm at the left larynx, which was compatible with rhabdomyosarcoma (Figure 3). The 18F-fluoro-2-deoxy-D-glucose positron emission tomography/computed tomography (FDG-PET/CT) scan delineated a 3 cm × 2 cm large 18F-fluoro-2-deoxy-D-glucose (FDG)-avid soft tissue mass with maximal standardized uptake value (SUVmax) of 8 at the left larynx without adjacent thyroid cartilage erosion (Figure 4). The complete tumor was removed via transoral laser microsurgery while the voice change did not occur. Non-enhanced computed tomography revealed a well-defined tumor at the left side of the larynx. (a) The fiberoscopic view of a bulky lesion beneath the arytenoid fold. (b) The endoscopic aspect of the larynx 5 years after tumor excision. Left laryngeal tumor in T1-weighted MRI scan. PET/CT image revealed a moderate FDG-avid lesion at the left side of larynx (SUVmax: 8).
The definite pathology report was laryngeal rhabdomyoma, which is consistent with previous biopsy results. The tumor cells showed rare to no mitotic figures, and the immunohistochemical analysis was positive for desmin and myogenin and was negative for CD68, S100, melan-A, and HMB-45 staining. The patient has been free of recurrence for 5 years after tumor excision (Figure 2(b)).
Discussion
Rhabdomyomas are rare benign tumors derived from skeletal muscles and are more uncommon than their malignant counterparts, rhabdomyosarcomas. 1 In the larynx, rhabdomyomas usually present as solitary lesions but may be multicentric in approximately 15% of cases. They are more prevalent in men than in women (4:1), and the reported ages of affected patients range from 16 to 76 years. 2 During endoscopy, laryngeal rhabdomyomas are usually seen as masses covered by the mucosa. Imaging findings usually suggest a benign lesion because of the submucosal location without invading the surrounding soft tissues. However, from previous reports and our case, we do not have a specific clinical image feature to distinguish rhabdomyoma from rhabdomyosarcoma.
MRI is the imaging modality of choice because of its superior soft tissue resolution and is highly effective in precisely determining the dimensions of tumor origin, local spread, and regional nodal involvement. 5 Rhabdomyoma usually presents as a homogenous lesion that is isointense or slightly hyperintense to muscle on T1- and T2-weighted MRI and slightly hyperdense on CT,4,6 and rhabdomyosarcoma also has similar characteristics, intermediate-to-low signal intensity compared with muscle on T1-weighted imaging, high signal intensity on T2-weighted imaging, and heterogeneous contrast enhancement. 5
In our case, the malignant tumor should not be ruled out because the tumor had few indistinct borders blending into adjacent isodense muscles and presented with heterogeneous contrast enhancement.
In FDG-PET/CT scans, a high SUVmax is one of the useful parameters for the differential diagnosis between malignant and benign tumors. Federico et al. 7 reported that primary rhabdomyosarcoma had an average SUVmax of 7.2 (range, 2.5–19.2) in the pediatric population. Bizon et al. 8 were the first to describe that adult-type rhabdomyoma in FDG-PET/CT scan has an elevated FDG uptake. de Trey et al. 6 confirmed this information by performing PET/CT in a patient with head and neck multifocal adult rhabdomyoma. The image showed an elevated FDG uptake in all previously diagnosed lesions, with a SUVmax of 2.9. Khalaf et al. 9 presented a multifocal adult FDG-avid rhabdomyoma of the head and neck. Interestingly, the FDG uptake level was slightly higher (SUVmax: 8) in our case, exceeding the average SUVmax of rhabdomyosarcoma.
In recent years, an increasing number of studies have reported a statistically significant association between SUV uptake and survival or aggressiveness in soft tissue sarcoma, 10 yet none of the related associations has been published in rhabdomyoma. To our knowledge, this is the fourth case reporting the finding of PET/CT scan and SUVmax data of rhabdomyoma. Further data information and case collection are needed to determine whether high or low SUVmax values are clinically significant in rhabdomyoma.
Conclusion
Laryngeal rhabdomyomas are rare tumors. To date, imaging findings alone are nonspecific for the diagnosis of rhabdomyoma in the adult population. Therefore, as head and neck surgeons, we must keep in mind that FDG-avid rhabdomyoma would imitate rhabdomyosarcoma in PET/CT scan and puzzle our decision-making. Diagnosis is confirmed by histopathology and immunohistochemistry.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.