
Abstract
Objective
Few reports discuss the characteristics of repeated recidivism of cholesteatoma. We describe the clinical characteristics of patients with cholesteatoma who experienced at least two recidivism episodes after initial surgery for cholesteatoma requiring canal wall reconstruction.
Methods
We reviewed the medical records of 11 patients who underwent surgery for cholesteatoma with canal wall reconstruction at our department between April 2008 and March 2018 and subsequently experienced two relapses that necessitated revision surgery involving tympanomastoidectomy with canal reconstruction. Patient age at the time of the first surgery ranged from 6 to 56 (mean, 25.7) years. Seven (63.6%) of the 11 patients were male. These 11 patients were classified according to the type of recidivism, and their characteristics (pathology, operation date, operation method, pattern of relapse, and position of recurrence) were investigated.
Results
Four cases involved secondary residual cholesteatoma, with the mean interval between the first revision surgery and the second revision surgery being 23.8 (range, 11–39) months. Secondary residual sites included the anterior tympanic cavity, tympanic sinus, and anterior end of the reconstructed cartilage of the canal wall. The other seven cases involved secondary recurrence, with the mean interval between the first and the second revision surgery being 26.1 (range, 12–57) months. The sites of recurrence were at the edges of the reconstructed cartilage. One notable case involved the cartilage junction, leading us to hypothesize that retraction of the temporal muscle flap and the patulous Eustachian tube was the underlying cause.
Conclusion
For residual cholesteatoma, strict measures are necessary to maintain the operation under clear view, and more careful follow-up is necessary in patients who have had previous surgery at another hospital. For recurrent cholesteatoma, it was recognized that Eustachian tube function must be ascertained in advance, and careful observation of the reconstructed cartilage edge is necessary.
Introduction
Middle ear cholesteatoma is one of the most common middle ear diseases, with an incidence of 9.2 to 12.6 cases per 100,000 adults and 3 cases per 100,000 children. 1,2 It is prone to recidivate, with one form of recidivism being residual cholesteatoma and the other being recurrent cholesteatoma. Residual cholesteatoma may not be detected on inspection, and a small recurrence may not be found on imaging findings. It is well known that residual cholesteatoma is more likely to occur when using the canal wall up (CWU) approach than in the canal wall down (CWD) approach, and recidivism rates can also be affected by surgical approaches. 3 Therefore, to reduce the risk of residual cholesteatoma as much as possible, we mainly performed mastoidectomy on demand, which is an approach to secure only the area necessary to confirm the entire cholesteatoma. In addition, the scutum and posterior canal wall were reconstructed with thin-sliced cartilage to maintain the postoperative morphology of the external auditory canal. However, a residual cholesteatoma sometimes occurred, necessitating staged surgery. By contrast, the open method of tympanomastoidectomy with canal reconstruction carries a risk of recurrent cholesteatoma. 4 As a countermeasure, the cartilage used for reconstruction is placed anteriorly close to the bone wall, and its height is adjusted to the original position of the tympanic membrane to prevent the formation of a retraction pocket. However, if recurrence occurs, revision surgery has to be performed when it becomes difficult to clean up the ear canal. When the mastoid cavity is wide open during surgery, it is filled with cortical bone, bone putty, cartilage fragments, or muscle flap to prevent retraction.
Despite these measures, relapse cholesteatoma is still experienced occasionally. Several reports regarding the characteristics of single recidivism of cholesteatoma have been published, but only a few have focused on and discussed those that recidivate repeatedly. Therefore, we investigated the characteristics of patients with repeated recidivism and discussed the countermeasures.
Materials and methods
Between April 2008 and March 2018, 221 ears in 212 patients underwent surgery for cholesteatoma in our department. Of these, surgery for cholesteatoma with canal wall reconstruction was performed on 175 ears of 166 patients, and 33 ears of 32 patients had only one recidivism (24 ears of 23 cases for residual cholesteatoma and 11 ears of 11 cases for recurrent cholesteatoma). Among these, 11 ears of 11 patients who underwent revision surgery due to relapse were included in the study. Patient age at the time of the first surgery ranged from 6 to 56 (mean, 25.7) years. Seven (63.6%) of the 11 patients were men. Patients were classified according to the type of recurrence, and the following factors were collected from patient medical records: pathology, operation date, operation method, pattern of relapse, and position of recidivism. The operation methods were categorized using the SAMEO-ATO system. 5 First and second recidivism rates were calculated using Kaplan-Meier survival analysis. The protocols were approved by the Ethics Review Committee of Tottori University (approval number 20A184). This study was conducted based on an opt-out policy: if a patient did not wish to be a research subject in this study, the patient’s information was immediately excluded from analysis and not used in this study.
Results
Residual cholesteatoma
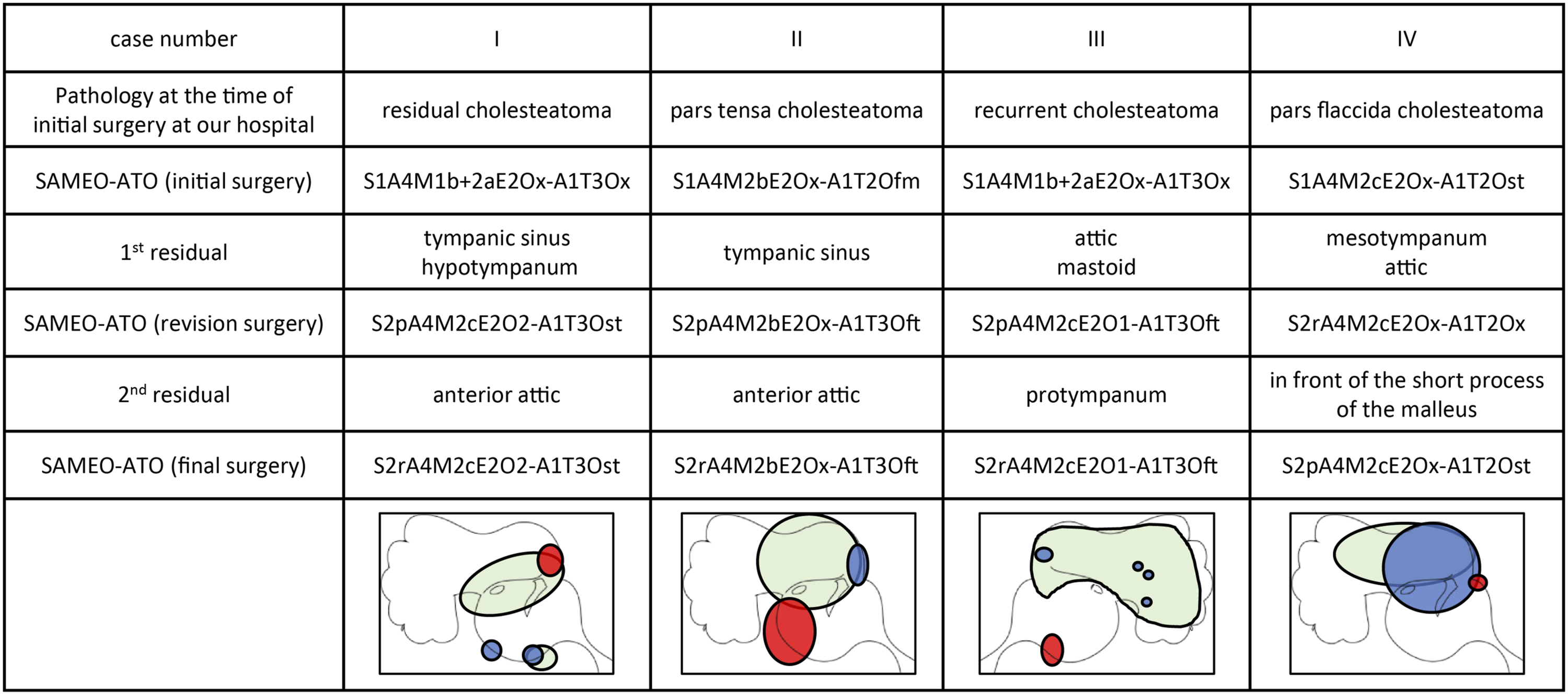
There were four cases of residual cholesteatoma that were repeated twice. These included two cases of pars flaccida cholesteatoma and two cases that developed residual cholesteatoma after surgery at other hospitals. The mean period from the initial surgery to the second revision surgery was 41.8 (range, 25–58) months, and the mean period from the revision surgery to the second revision surgery was 23.8 (range, 11–39) months (Figure 1A). Residual recidivism rate is shown in Figure 1B. Second residual cholesteatomas were found in the anterior tympanic cavity, tympanic sinus, and anterior end of the reconstructed cartilage of the canal wall (Figure 2). There were two cases of remnant ectopic recidivism, both of which involved patients who developed cholesteatoma after surgery at other hospitals. Hearing results after final surgery were as follows: 0–10 dB in 1 case, 21–30 dB in 1 case, and >30 dB in 2 cases. The postoperative condition of the tympanic membrane was generally good in all cases, but only one case had a slight retraction that did not require maintenance. No otorrhea was observed in any of the patients. Period from initial surgery to reoperation in cases of residual cholesteatoma. Gray bars: period from initial surgery to first reoperation. Dark gray bars: period from the first reoperation to the second reoperation. In cases I–III, the patient was followed up after confirmatory surgery, and surgery was performed upon recognition of recidivism. In case IV, the patient was diagnosed with residual cholesteatoma and underwent staged surgery after dropping out of follow-up. (B) Residual recidivism rate in Kaplan-Meier survival analysis. The timing of the first residual recidivism and the second residual recidivism followed a similar trend. Lesion of repeated residual cholesteatomas. Green: primary cholesteatoma. Blue: 1st residual cholesteatoma. Red: 2nd residual cholesteatoma. Repeated recidivism was observed in areas where it was difficult to secure the field of view or perform surgical operations. Two cases of ectopic residual cholesteatoma were observed.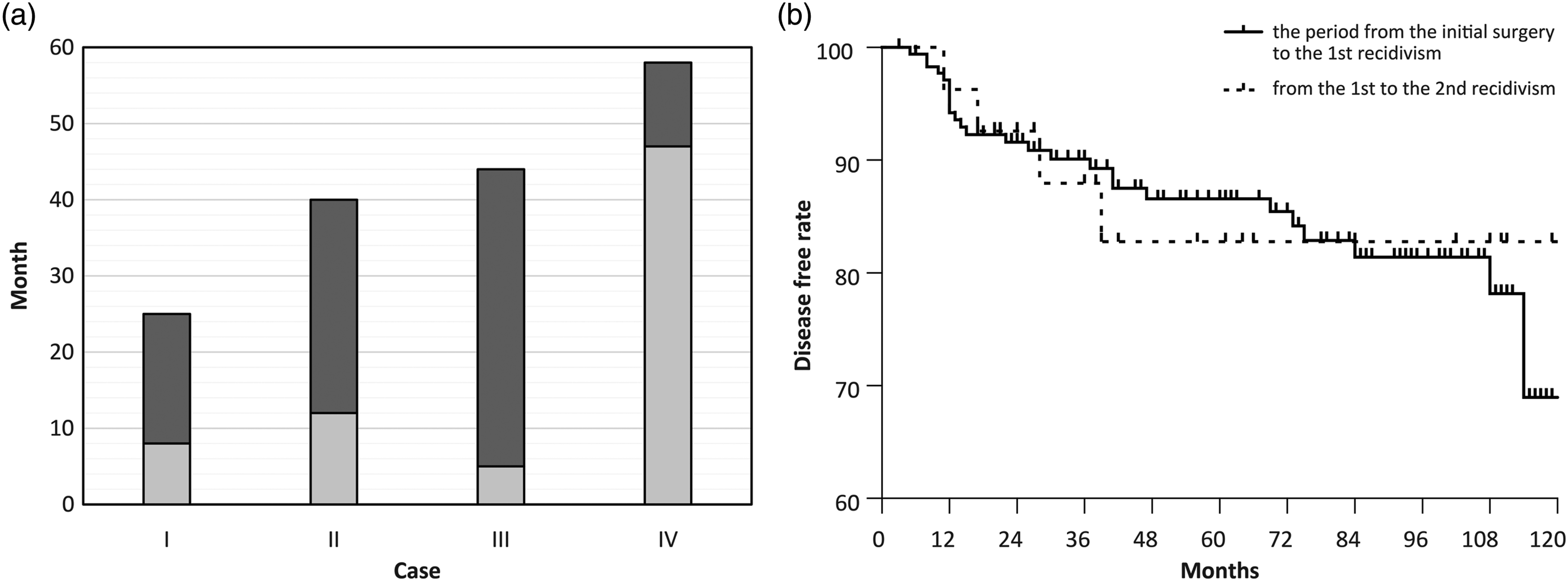
Recurrent cholesteatoma
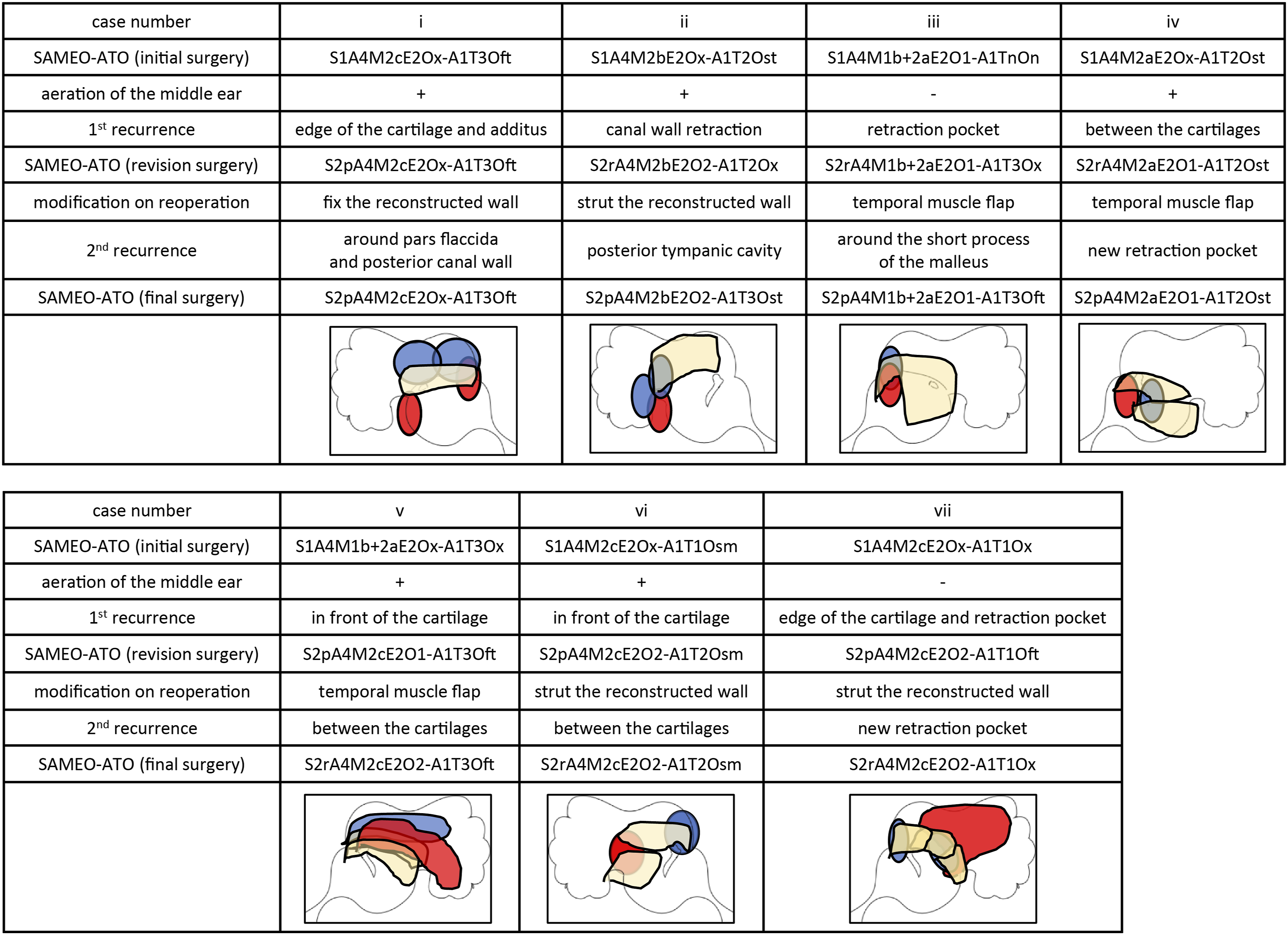
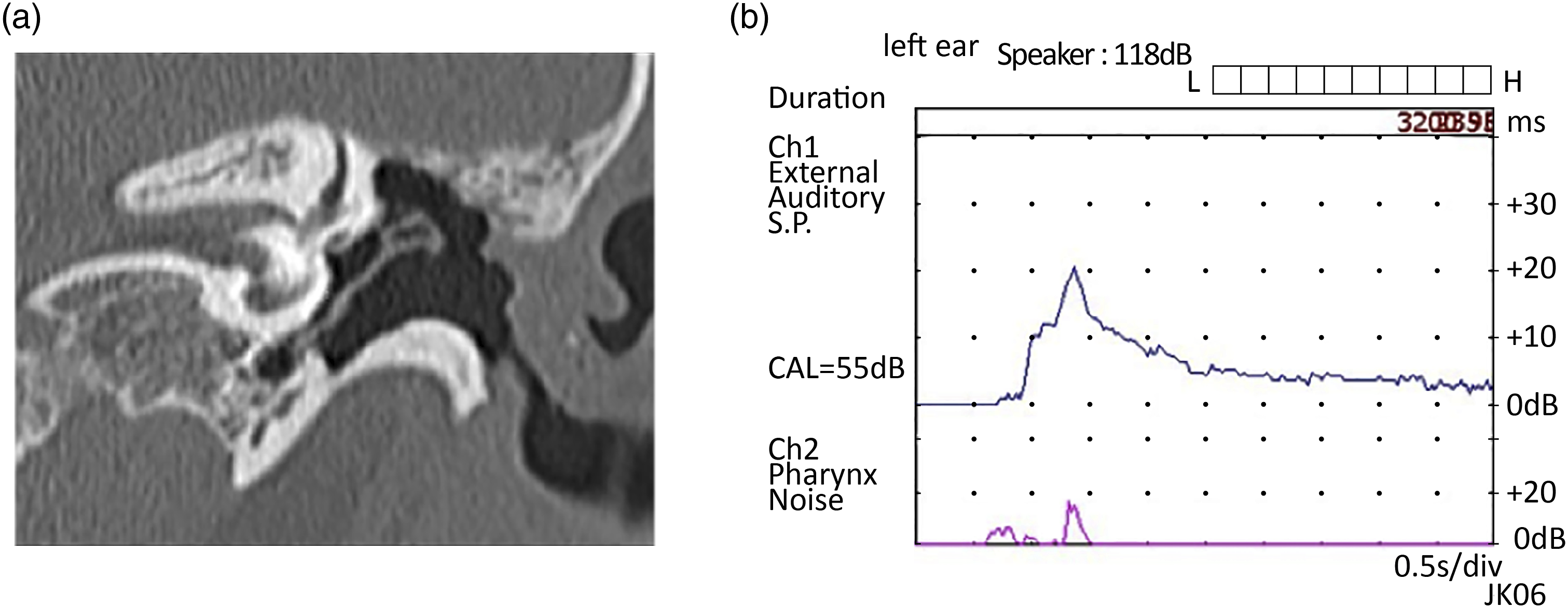
There were seven cases of recurrent cholesteatoma which were repeated twice. These included four cases of pars flaccida cholesteatoma and three cases that developed cholesteatoma after surgery at other hospitals. The mean period from the revision surgery to the second revision surgery was 26.1 (range, 12–57) months (Figure 3A). Recurrent recidivism rate is shown in Figure 3B. The sites where the first and second recurrences occurred are summarized in Figure 4. The most common sites of recurrence were the edges of the reconstructed cartilage and the area where the cartilage overlapped. In case v, in which there was a large relapse from the cartilage junction, it was expected that the retraction of the temporal muscle flap and patulous Eustachian tube was affected (Figure 5). Hearing results after final surgery were as follows: 11–20 dB in 3 cases, 21–30 dB in 1 case, and >30 dB in 3 cases. As for the postoperative condition of the tympanic membrane, only two cases showed slight retraction, but no maintenance was required. No otorrhea was observed in any of the patients. Period from initial surgery to reoperation in cases of recurrent cholesteatoma. Black dot bar: the period from initial surgery to reoperation. White dot bar: the period from the first reoperation to the second reoperation. In cases I-IV, the patients were followed up after the initial surgery and underwent recessive surgery followed by confirmatory surgery. In cases V–VII, the patients were followed up after confirmatory surgery and underwent reoperation due to retraction pocket formation. (B) Recurrent recidivism rate in Kaplan–Meier survival analysis. Lesion of recurrent cholesteatoma. Blue: lesion of the first recurrence. Red: lesion of the second recurrence. Yellow: area of the reconstructed cartilage before the second reoperation. Results of examination of case V. (A) Computed tomography image of the temporal bone. The external auditory canal and scutum were retracted, forming an open cavity. (B) Sonotubometry results showing patulous Eustachian tube.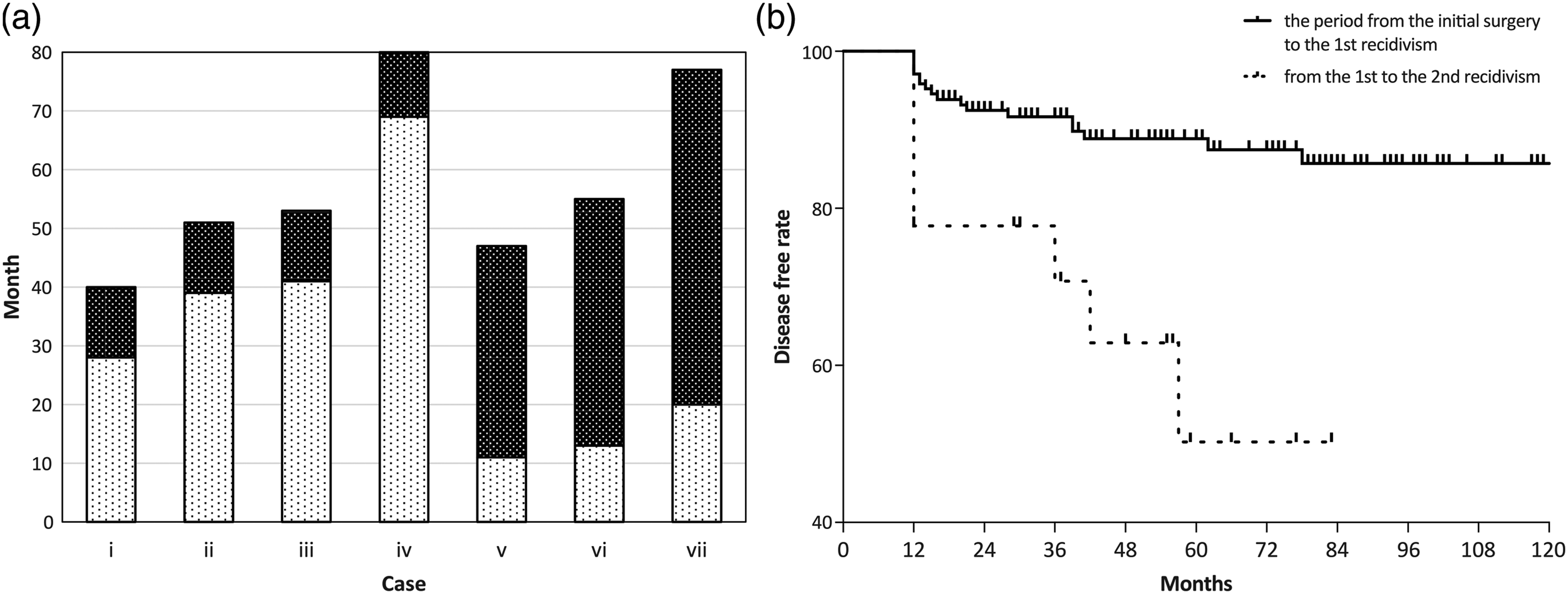
Discussion
The standard surgical treatment for a cholesteatoma is its complete removal so that the middle section of the ear is maintained in good condition and is free from recidivism. Cholesteatoma recidivism can be divided into residual and recurrence types. To reduce residual cholesteatoma, it is important to remove the cholesteatoma without disrupting the matrix. 6 Therefore, it is important to consistently establish a clear view of the surgical field to confirm that continuous removal has been achieved. 7 In our department, tympanomastoidectomy with canal wall reconstruction, which is based on the method described by Suzuki, 8 is performed as the basic technique. This method has the following advantages: it removes the cholesteatoma under clear view, reduces the risk of residual cholesteatoma, brings the external auditory canal morphology closer to normal shape, and prevents cavity problems. In contrast, one disadvantage of this technique is that there is always the risk of developing recurrence. 4 Recurrence is generally believed to be associated with postoperative re-aeration of the tympanic cavity. Therefore, when performing surgical treatment for patients with poor aeration in the tympanic and mastoid cavity, we used bone fragments or bone putty to physically reinforce the reconstructed part of the ear canal to fill the mastoid cavity. 9
In contrast, it is difficult to completely prevent residual cholesteatoma even in cases of CWD tympanomastoidectomy, meaning that staged or confirmatory surgery has to be performed as a countermeasure. 10,11 In addition, after surgery, patients should undergo long-term follow-up to check for residual cholesteatomas using imaging examinations, or to detect recurrent cholesteatoma. If recidivism is observed, the lesion should be resected consecutively by revision surgery whenever possible, and if there is bone remaining in the recurrent lesion, additional drilling should be performed. However, most previous reports were limited to a single recidivism, and we believe that comprehensively determining the clinical characteristics of cholesteatoma would be significant for the management of patients with repeated recidivism.
With regard to residual cholesteatoma, Nobel et al 12 stated that it is most likely to occur in areas that are difficult to visualize and manipulate, and that the incidence also increases when visualization is difficult to perform due to bleeding. Therefore, in microscopic surgery, it is difficult to remove areas that cannot be visualized clearly, such as the facial recess and the tympanic sinus, 13 even when using the CWD approach. By contrast, the removal procedure is also an important factor affecting the risk of residual cholesteatoma. Sheehy et al 14 and Ogawa et al 15 have categorized the risk of residual cholesteatoma development based on the removal status and discussed the indications for staged surgery. They indicated that the surgeon’s judgment of whether the cholesteatoma was removed reliably is an important factor.
In the present study, cases of repeated residual cholesteatoma were found in the anterior tympanic route, in front of the malleus, and in the posterior tympanic cavity, where blind manipulation is required in microscopic surgery. This result is similar to reports on single recidivism, which were performed when high-definition endoscopes were not yet fully available. Blind manipulation is a risk factor, and the combined use of high-definition endoscopes, which has become widespread in recent years, is considered to be indispensable. In contrast, it was interesting to note that ectopic residual cholesteatoma with different sites was observed only in the cases that developed cholesteatoma after surgery at other hospitals. In these cases, it is easy to lose the details of removal at the time of the initial surgery of the primary site. Performing follow-up was considered necessary, and more attention should be paid to residuals in these cases.
Recurrent cholesteatoma is greatly influenced by postoperative re-aeration of the tympanic and mastoid cavity. 8 Age, 16 Eustachian tube function, 17 and mucosal preservation 18 have been reported as factors that affect retraction. In the present study, there was recurrent cholesteatoma at the edge of the reconstructed cartilage fragment and at the site where the cartilage was overlaid. The reason for the recurrence in this area seems to be the vulnerability of the connection. As the wound heals after surgery, the reconstructed cartilage adapts to the defect, but the cartilage edge may retract or protrude in some cases. In addition, poor aeration increases the negative pressure in the middle ear cavity, which may lead to further deformation of the reconstructed area. Therefore, the cartilage used for reconstruction should be as large as possible, and the number of joints should be reduced to prevent recurrence. Depending on the size of the defect, both the auricular cartilage and nasal septal cartilage may be considered as reconstruction materials. In addition, in cases of poor Eustachian tube function, there is a risk of large retraction pocket formation as in case v. Therefore, it is necessary to insert a ventilation tube 19 or perform mastoid obliteration if the risk of residual is low. 20 In recent years, there have been some reports that the transcanal endoscopic approach is effective in preventing recurrence and underscores the importance of the mucosa and mastoid air cells. 21,22 It may be necessary to fundamentally reconsider the approach and incorporate methods that strive to preserve the mucosa in future studies.
In these cases of repeated recidivism, it is reasonable to consider that the postoperative follow-up period begins a new follow-up period from the time of the last surgery. With regard to the appropriateness of the length of the follow-up period for cholesteatoma, some reports suggest that approximately 10 years or more is necessary. 23,24 However, their findings may have been influenced by differences in the equipment and resolution currently used for imaging studies. In some of those cases, detection may even have been delayed due to a lack of detailed confirmation. Patient selection bias due to the small number of cases and differences in follow-up methods are also cause for concern in these studies. Therefore, adequacy of the length of the follow-up period remains controversial although Kuo et al 24 reported that a follow-up period of less than 5 years was clearly inadequate. In our study, recidivism was observed in some cases approximately 5 years after the initial or final surgery, which supports their results, indicating the need for follow-up examination and imaging studies for at least 5 years after the final surgery.
However, we also observed that our cases had a higher recidivism rate than that reported previously. 3 One reason for this phenomenon, according to Kuo et al, 24 is that the standard calculation method tended to underestimate the recidivism rate compared to the Kaplan–Meier analysis, and this discrepancy increased with the follow-up duration. Another potential reason for the difference in our study findings may be that the aggressive confirmatory surgery, which was performed in approximately half of the patients in this study, detected smaller residual recidivism at an early stage; this could not be confirmed on postoperative follow-up with imaging examination alone. However, all inherent limitations and risks of bias observed in this study may be due to the small sample size and the retrospective design of this study. Hence, the results and findings of this study cannot be generalized to different populations. In contrast, considering radiation exposure, it is not desirable to always perform temporal bone computed tomography (CT) scans, and it is desirable to perform examinations with lower radiation doses at each follow-up using either cone-beam CT or non-echo-planar diffusion-weighted magnetic resonance imaging. 25
Cases of repeated recidivism of cholesteatoma were presented in this study. For residual cholesteatoma, strict measures such as the use of an endoscope and additional drilling at the extraction site are necessary to maintain the cholesteatoma removal operation under clear view, and more careful follow-up is necessary in cases who underwent previous surgery at other hospitals. For recurrent cholesteatoma, it was recognized that the Eustachian tube function must be ascertained in advance, and careful observation of the reconstructed cartilage edge is necessary. Postoperative follow-up with imaging examination should be performed for approximately 5 years from the last surgery.
Footnotes
Authors’s Note
The 28th Annual Meeting of the Japan Otological Society (3/Oct/2018 – 6/Oct/2018).
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics approval
The protocols were approved by the Ethics Review Committee of Tottori University (approval number 20A184).