
Abstract
Lymphangiomas are rare benign tumors of the lymphatic system, most often found at birth and before the age of 2 years. The head and neck region are the most frequent locations for lymphangioma. Involvement of the adult larynx in isolation is rare, and only a few cases have been reported so far. We report the case of a patient with a left false vocal cord reddish tumor presenting with hemoptysis and voice cracking. The surgical excision of mass was performed by direct laryngoscopy-assisted CO2 laser. The histopathological report revealed the diagnosis as cavernous lymphangioma. After a follow-up of 1 year, the patient is free of recurrence with all laryngeal functions being normal.
Keywords
Introduction
Lymphangiomas are rare, benign malformations of the lymphatic system with abnormal development in localized centers. According to the size of lymphatic cavities, 3 lymphangioma subtypes exist: capillary lymphangiomas (microcystic), cavernous lymphangiomas (macrocystic), and cystic lymphangiomas or hygromas. 1 Lymphangioma usually exists in the head and neck region. More than 90% of lymphangiomas appear before the age of 2 years, and the onset of lesions after 2 years of age is rare. They have an obvious predilection for the head, neck, oral cavity, axilla, and abdomen.1,2 Although the head and neck area is the most common location of the presentations of lymphangiomas, isolated laryngeal lymphangioma is extremely rare, with only a few cases reported.3-5 We present a case of a patient with left false vocal cord cavernous lymphangioma who presented with hemoptysis and voice cracking. These clinical symptoms have not been reported previously.
Case Report
A 28-year-old woman was presented to our outpatient clinic with complaints of pitch break and blood-tinged sputum production for 2 months. She denied the presence of sore throat, dyspnea, dysphagia, or any other chronic condition. At symptom appearance, she visited the chest internal medicine department. However, chest X-ray showed no positive findings. Thus, she was transferred to our outpatient clinic. On inspection of the laryngovideostroboscopy (LVS), a smooth and purple-reddish globular mass on the left false vocal cord was identified. During phonation, the mass was observed to move over the true vocal cords and was attached to the right false vocal cord (Figure 1A). Blood oozing was also observed at the mass surface after phonation during LVS inspection (Figure 1B). No other abnormal findings were observed at the nasopharynx, oropharynx, or hypopharynx. Under the impression of a tumor lesion on the left false vocal cord, complete resection was performed under direct laryngoscopy assisted by carbon dioxide laser. All laryngeal structures were preserved, and hemostasis was ensured. The remaining parts of the larynx appeared normal. The patient was discharged the day after surgery with a 1-week vocal rest. (A) The left false cord congested mass was identified under the laryngovideostroboscopy (LVS) when the first time the patient visited. (B) Phonation caused the mass to be squeezed. (C) Operation wound followed up after 2 months from the operation day. The wound was healing well with intact vocal cords.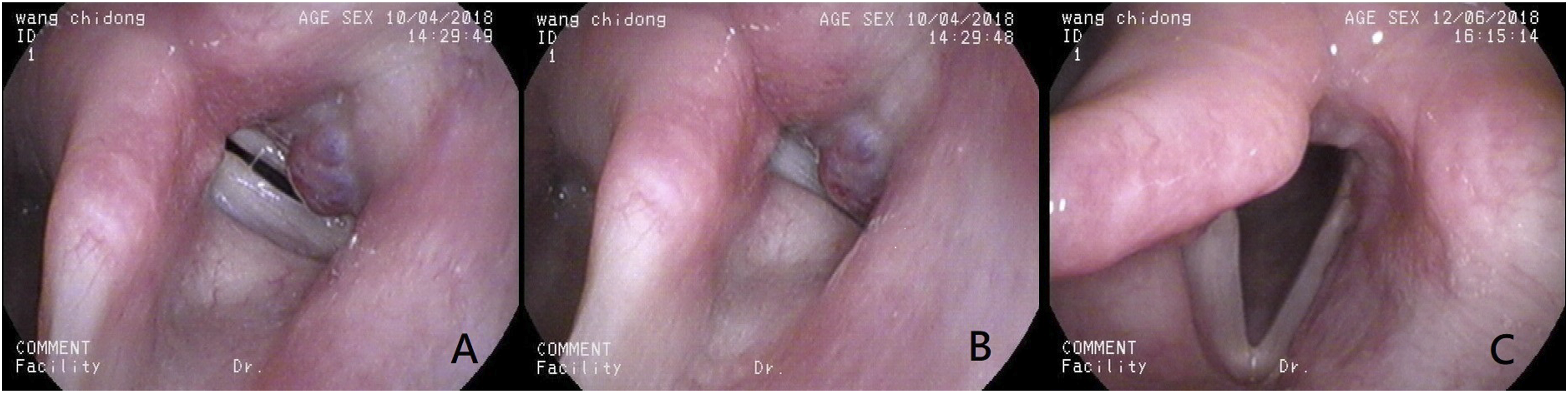
Histopathological examination of the specimen revealed cavernous lymphangioma. Microscopic view of the specimen revealed lymphatic channels of varying sizes that were filled with proteinaceous fluid (Figure 2), with no evidence of malignancy. The patient’s symptoms were resolved after complete resection of the lesion, including voice cracking and blood-tinged sputum production. The wound spontaneously healed, with no evidence of recurrence after a follow-up period of 1 year (Figure 1C). Cavernous lymphangioma. Histopathological analysis showing the presence of varying-sized lymphatic channels filled with proteinaceous fluid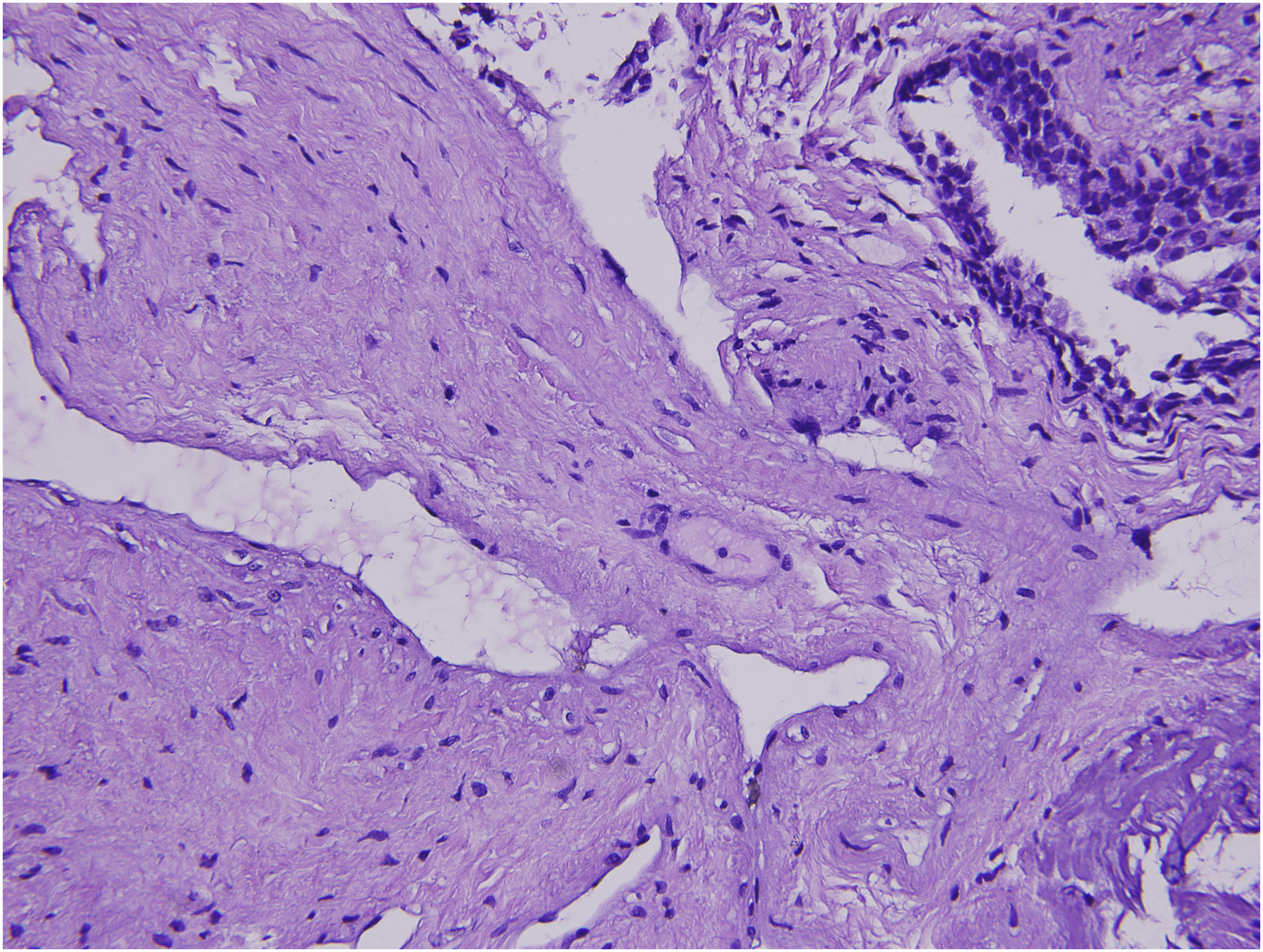
Discussion
Lymphangiomas are rare, benign malformations of the lymphatic system, with the vast majority of cases presenting before 2 years of age. In most studies, lymphangiomas are considered congenital lesions6-8; they may be the result of failed lymphatic drainage and are discovered during routine prenatal ultrasounds. 8 Acquired lymphangiomas may result from trauma, infection, or chronic lymphatic compression. 9 Lymphangiomas are due to the abnormal development of the lymphatic system in localized centers. Under microscopic view, cavernous lymphangiomas are composed of dilated lymphatic channels with one or more endothelial layers with or without an adventitial layer. In our case, the specimen showed a cavernous lymphangioma and was isolated without diffuse tissue edema.
Lymphangiomas usually exist in the head and neck region, and over 90% of lesions appear before the age of 2 years (50% of lesions are noted at birth). Lesion onset after 2 years of age is rare, and onset during adulthood is even rarer. 10 Naidu and McCalla 11 reported a comprehensive review of studies on lymphatic malformation in adults. They found 91 adult cases from 1828 to 2000. These lymphangiomas were located in the neck in all patients. Lymphangiomas have an obvious predilection for the head, neck, axilla, oral cavity, and abdomen, where a rich network of lymphatic vessels is present.1,12 Lymphangiomas originating from the larynx are extremely rare and mainly occur in regions where friction is common due to the passage of food and where many lymphatic vessels are present, including the lingual surface of the epiglottis, aryepiglottic folds, and arytenoid region. 13 To the best of our knowledge, only 2 cases of adult lymphangioma located on the false vocal cord have been reported in Turkey and Japan. Cinar et al 13 reported the case of a 47-year-old woman with the complaint of hoarseness for 3 months. Examination with indirect laryngoscopy revealed a large lymphangioma originating from the right false vocal cord, which was removed using cold instruments. Naito et al 14 reported the case of a 36-year-old woman with the complaint of hoarseness for several months, which was associated with cystic lymphangioma on her right false vocal cord. We collected 12 cases of adult laryngeal lymphangioma from 1908 to 1984, of which the lesion originated from the false vocal cord in only one case.
Symptoms of lymphangiomas depend on the location and size of the mass. 7 Laryngeal lymphangiomas present with symptoms such as voice change, stridor, and airway obstruction. Some cases have been reported in infants and children with respiratory compromise.4,5,15 Kenton et al 16 reported the case of a neonate with lymphangioma of the larynx, with symptoms of stridor, with progression to respiratory failure. To the best of our knowledge, there has been no diagnosis of lymphangioma of the false vocal cord in newborns or infants. In adults, symptoms of laryngeal lymphangiomas vary. Seven et al 3 reported the case of a 37-year-old female patient with lymphangioma on the lingual surface, who showed the symptoms of acute epiglottitis such as sore throat, dysphagia, and sensation of a lump in the throat. As to our case, the patient presented with hemoptysis and voice cracking, which were different from the symptoms documented in previous reports of false vocal cord lymphangiomas.13,14 Hemoptysis was explained by the blood oozing of the false vocal cord lymphangioma due to friction and compression during phonation, which was revealed by LVS. Voice cracking could also be attributed to the location of the lymphangioma, which occurred due to the vibration of the vocal cord. Our patient presented with no complaints of hoarseness, dyspnea, or sensation of lump in the throat, which were previously reported in other adult cases of laryngeal lymphangioma.3,10,11,13,14
Lymphangiomas have a high recurrence rate; hence, total surgical excision is the preferred management if the patient’s condition allows it. 6 We should consider preserving vital structures to prevent complications arising from phonation, respiration, and swallowing after surgery. The location, size, and extension of the lesion can help us to design the operation plan. 3 Treatment options such as cold instrument surgical excision, laser debulking, sclerotherapy, and corticosteroids have been proposed. 7 Laser surgery has the advantages of less bleeding and tissue edema compared with surgical resection, and both carbon dioxide laser and neodymium:yttrium-aluminum-garnet laser have been reported in the literature. 6 Sclerosing agents are currently under investigation, including morrhuate sodium, dextrose, tetracycline, doxycycline, bleomycin, ethanol, ethibloc, and OK-432. The purpose of sclerotherapy is to reduce the lesion size and to relieve symptoms for ease of surgical resection. 17 However, severe complications can occur after sclerotherapy, such as damage to adjacent soft tissues, which would render future operations more difficult. 6 On the other hand, radiation therapy may cause secondary malignancies and is ineffective for lymphangiomas. 7
In the previous cases of false vocal cord lymphangioma, Cinar et al 13 reported the excision of false vocal cord lymphangiomas with cold instruments. In 1985, Naito et al 14 performed tracheostomy and resected the sessile tumor through the laryngofissure approach. In both cases, symptoms resolved with preserved laryngeal function after the procedures. In our case, considering the small lesion size and the convenience of hemostasis, we used carbon dioxide laser to excise the lesion without causing damage to the surrounding vital structures of the larynx under direct laryngoscopy. No recurrence of disease occurred after a follow-up of 1 year, and the laryngeal function has been normal till date.
Conclusion
We reported this case of lymphangioma because of the unusual, involved site; isolation of the lymphangioma on the false vocal cord; and presentation at the rare adulthood stage. In addition, such a complaint of hemoptysis has not been previously reported. Although adult laryngeal lymphangioma is rare and the location at the false vocal cord is even rarer, otolaryngologists should consider lymphangiomas as a differential diagnosis for false vocal cord lesions.
Footnotes
Acknowledgments
The authors wish to thank the patient for participating in this study.
Author’s Note
The patient’s permission was obtained.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Chi-Mei Medical Hospital.