
Abstract
Objectives
This study aimed to investigate the perilymph metabolism by analyzing the 3D real IR MR findings in acoustic neuroma (AN) after intravenous administration of gadolinium (Gd).
Methods
Eleven patients (6 men and 5 women) diagnosed with AN were included, and 3D real IR MRI was performed 4 hours after intravenous Gd injection. The signal intensity and details of inner ear, tumor, and internal auditory canal (IAC) by MRI were analyzed.
Results
Four patients had tumors confined to the IAC, and 5 had tumors that extended to the cerebellopontine angle cistern. The signal intensity of the cochlea, vestibule, and IAC fundus was conspicuously enhanced in 3D real IR images than the control side. One patient had a tumor in the cochlea, in which the signal intensity of the semicircular canal and vestibule was increased. One patient had an intravestibular tumor in which the signal intensity of the semicircular canal was increased and the cochlea had endolymphatic hydrops in the affected ear.
Conclusions
The synchronously increased signal intensity in the inner ear and IAC may indicate that IAC may serve as a channel for removal of the perilymph in the inner ear; the blockage by the tumor may have changed the hydrodynamics of the perilymph to cause a longer retention of Gd in the inner ear.
Introduction
The stable metabolism of perilymphatic fluid is crucial for the inner ear function, and diagnosis and treatment of many inner-ear diseases were based on the metabolism of perilymphatic fluid. There have been several reports indicating the sources and metabolism of perilymphatic fluid; however, it remains uncertain. Previously, the sources of the perilymph were reported from blood vessels of the membranous labyrinth1,2 and cerebrospinal fluid (CSF) via the cochlear aqueduct,3,4 the openings in the osseous spiral lamina,5,6 and in the internal auditory canal (IAC). 7 Controversially, Waltner (1948) believed that there is no active flow between the CSF and perilymph, and Kommoss and Giebel (l978) could not confirm CSF flow into the perilymph through the cochlear aqueduct. Namely, the communications between perilymph and blood vessels, cochlear aqueduct, and IAC require further exploration.
Recently, intravenous injection of gadolinium (Gd) (IV method) was widely used to visualize endolymphatic hydrops (EH) by entering the perilymph without entering the endolymph. Meanwhile, IV method can demonstrate the condition of the bilateral labyrinth, independent of the condition of the round window membrane 8 ; it will hint potential information of perilymph when there is a difference between two sides. Therefore, the IV method can be used as a method to explore the perilymph metabolism. An acoustic neuroma (AN) is a slow-growing benign tumor of the vestibular portion of the VIIIth cranial nerve. The tumor can be located in the vestibule, cochlea, or IAC,9,10 blocking the transport of lymph fluid at the various locations. It may contribute to the investigation of perilymph metabolism. Moreover, several researchers have shown that the signal intensity of ipsilateral labyrinthine lymph fluid is increased in most cases of AN on 2D and 3D FLAIR, 8 which may indicate the altered lymph fluid metabolism in AN.
Therefore, to investigate the metabolism of perilymphatic fluid, we analyzed 3D real IR images after intravenous administration of Gd obtained in 11 patients with AN in detail.
Materials and Methods
Patients
Eleven patients (6 males and 5 females) with AN were included with a mean age of 50.5 ± 16.7 years old. The basic characteristics of the 11 patients were analyzed. None of the patients had received stereotactic radiosurgery or surgery. The approval number of the ethics committee was 2014007, and all patients signed informed consent forms.
IV Gd Injection and MRI Acquisition
All patients underwent IV injection of a double dose (0.4 mL/kg body weight) of Gd-HP-DO3A; 4 hours later, MRI was performed. For the IV method, all scans were performed on a 3T MRI scanner (Verio; Siemens Health care, Erlangen, Germany) using a 32-channel phased array receive-only coil. T2-space and 3D real-IR sequence MRIs were applied to collect images. The parameters for the 3D-real-IR sequence were as follows: voxel size = 0.17 × 0.17 × 0.6 mm; scan time = 15 min and 20 seconds, repetition time = 6000 milliseconds, echo time = 181 milliseconds, inversion time = 1850 milliseconds, slice thickness = 0.6 mm, field of view = 160 × 160 mm, and matrix size = 768 × 768.
Results
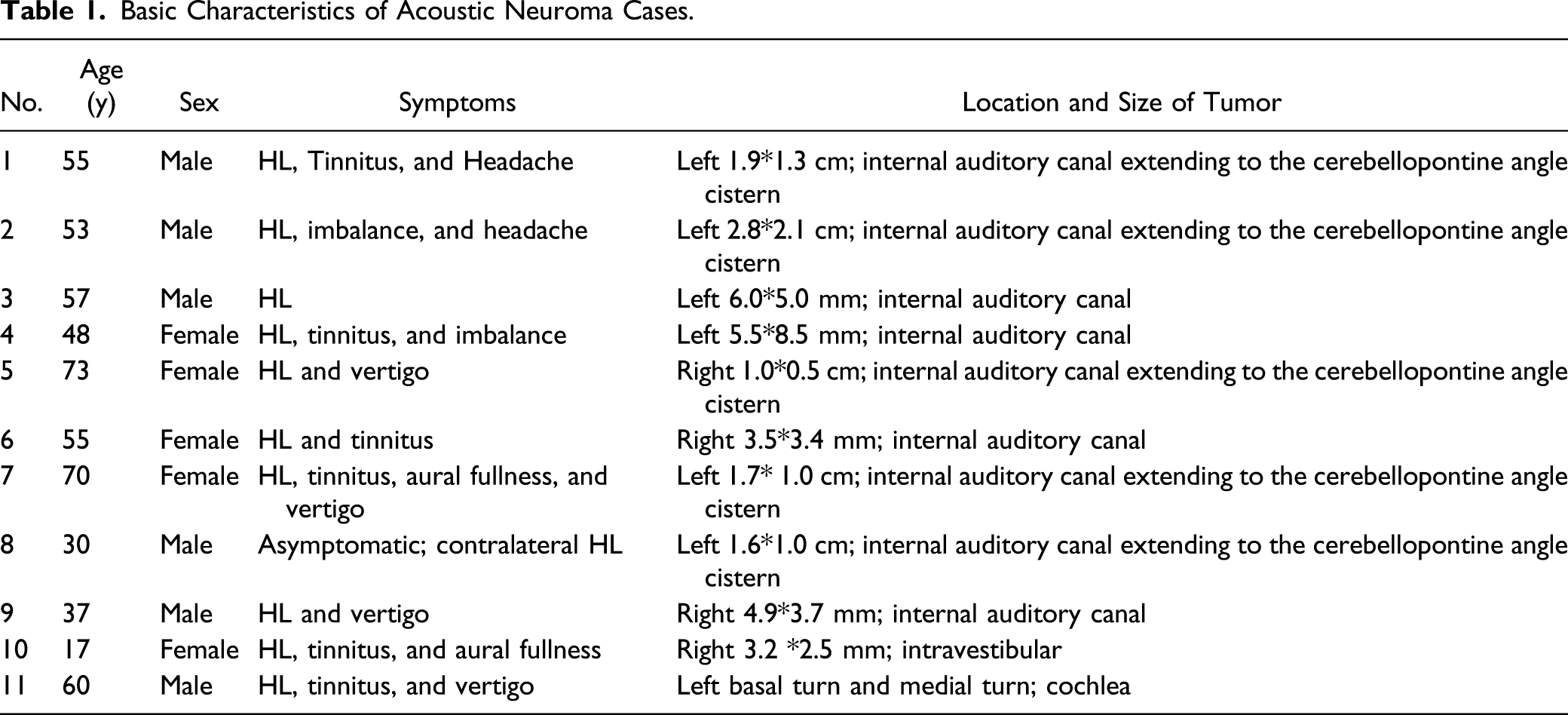
Basic Characteristics of Acoustic Neuroma Cases.
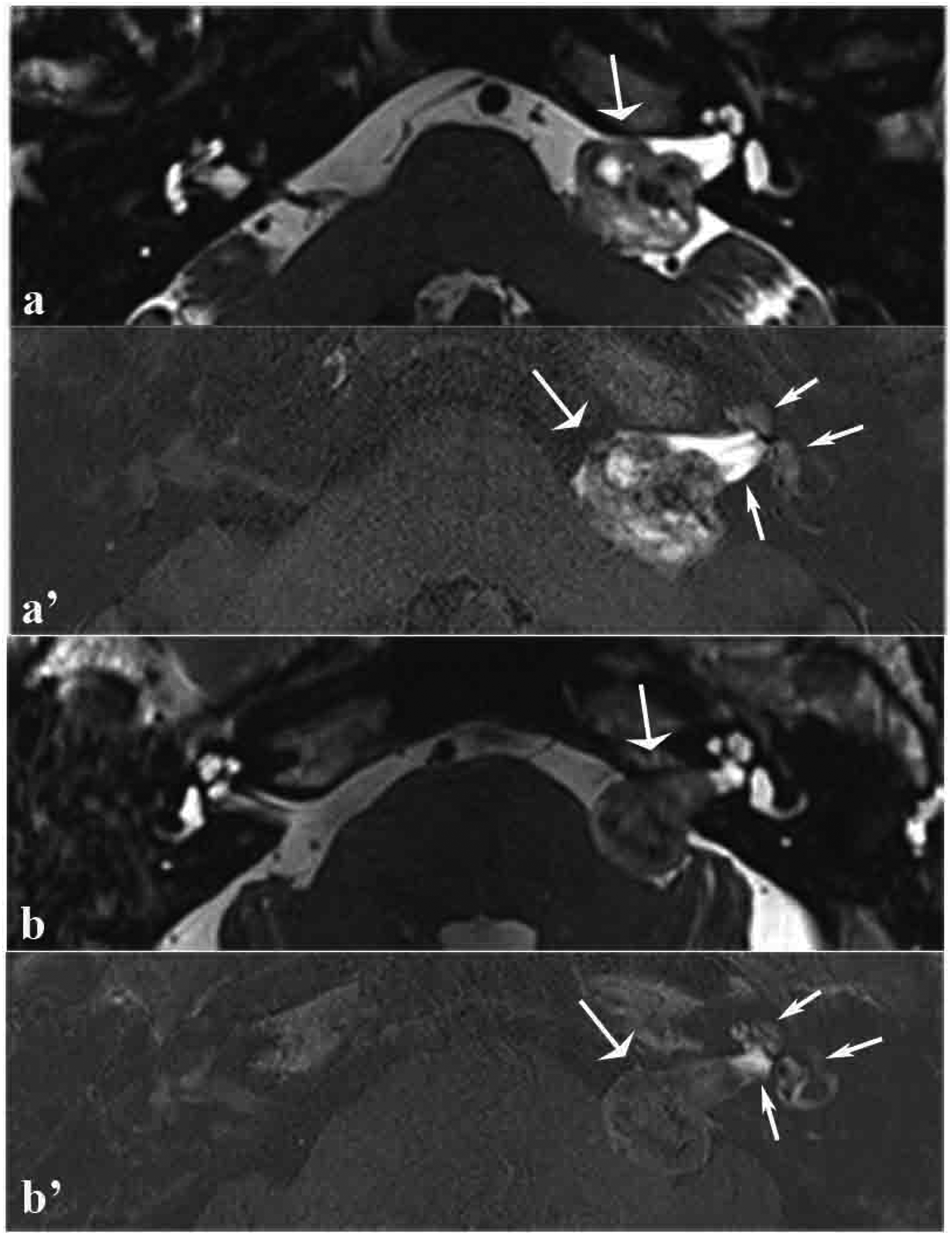
MRI scans of 2 patients with tumors in the left internal auditory canal that extended to the cerebellopontine angle cistern. (a and b,)T2-space sequence MRI scan showing filling defects in the internal auditory canal and cerebellopontine angle (broad arrow). (a’ and b’) 3D real IR MRI scan showing that the signal intensity in the cochlea, vestibule, and internal auditory canal proximal to the cochlea was higher than that observed in the contralateral side and that the signal intensity of the tumor increased unevenly and less significantly (thin arrow).
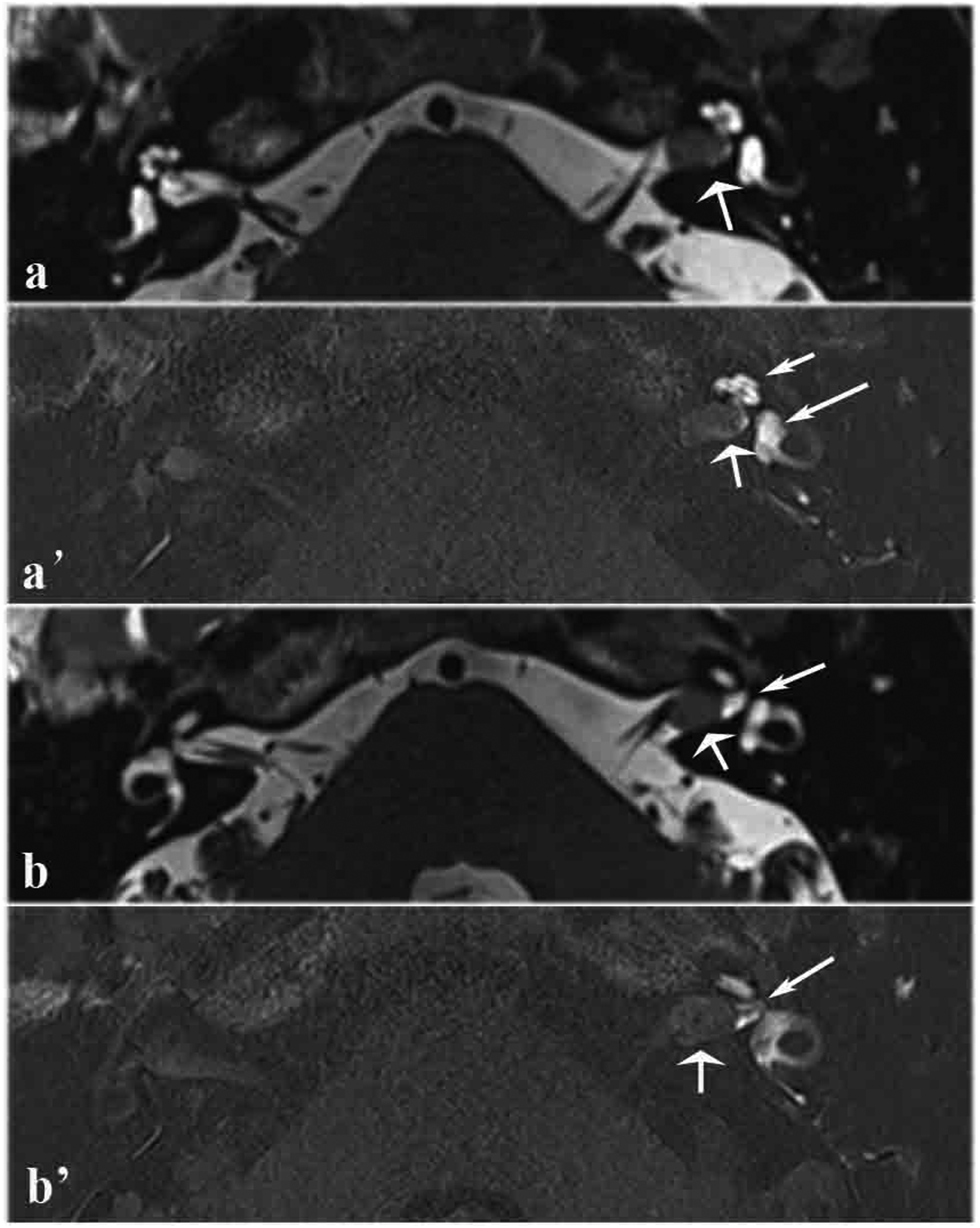
MRI scans of a patient with a tumor in the left internal auditory canal. (a) T2-space sequence MRI scan showing filling defects in the internal auditory canal (broad arrow). (a’) 3D real IR MRI scan showing elevated signal intensity in the cochlea and vestibule (thin arrow). (b) T2-space sequence MRI scan showing filling defects in the internal auditory canal, while the fluid among the nerve adjacent to the fundus of the internal auditory canal was not affected (broad arrow). (b’) 3D real IR MRI scan showing elevated signal intensity in the fluid among the nerve adjacent to the fundus of the internal auditory canal (thin arrow).
A 17-year-old patient had intravestibular schwannoma that manifested as fluctuating hearing loss (125, 250, 500, and 1000 Hz; 10∼60 dB) for 8 months; it was later accompanied by ipsilateral constantly active ear fullness and tinnitus without vertigo. A T2-space sequence MRI scan showed filling defects in the vestibule (Figure 3A). A 3D real IR MRI scan showed significantly increased signal intensity in the semicircular canal (Figure 3B), and significant cochlear EH in the affected ear (Figure 3C). No ELH was observed in other 10 patients. MRI scans of a patient with a right intravestibular tumor. (A) T2-space sequence MRI scan showing filling defects in the vestibule (arrow). (B) 3D real IR MRI scan showing the signal intensity of the semicircular canal was higher on the affected side than on the contralateral side (arrow). (C) 3D real IR MRI scan showing significant ELH in the ipsilateral cochlea (arrow, red circle).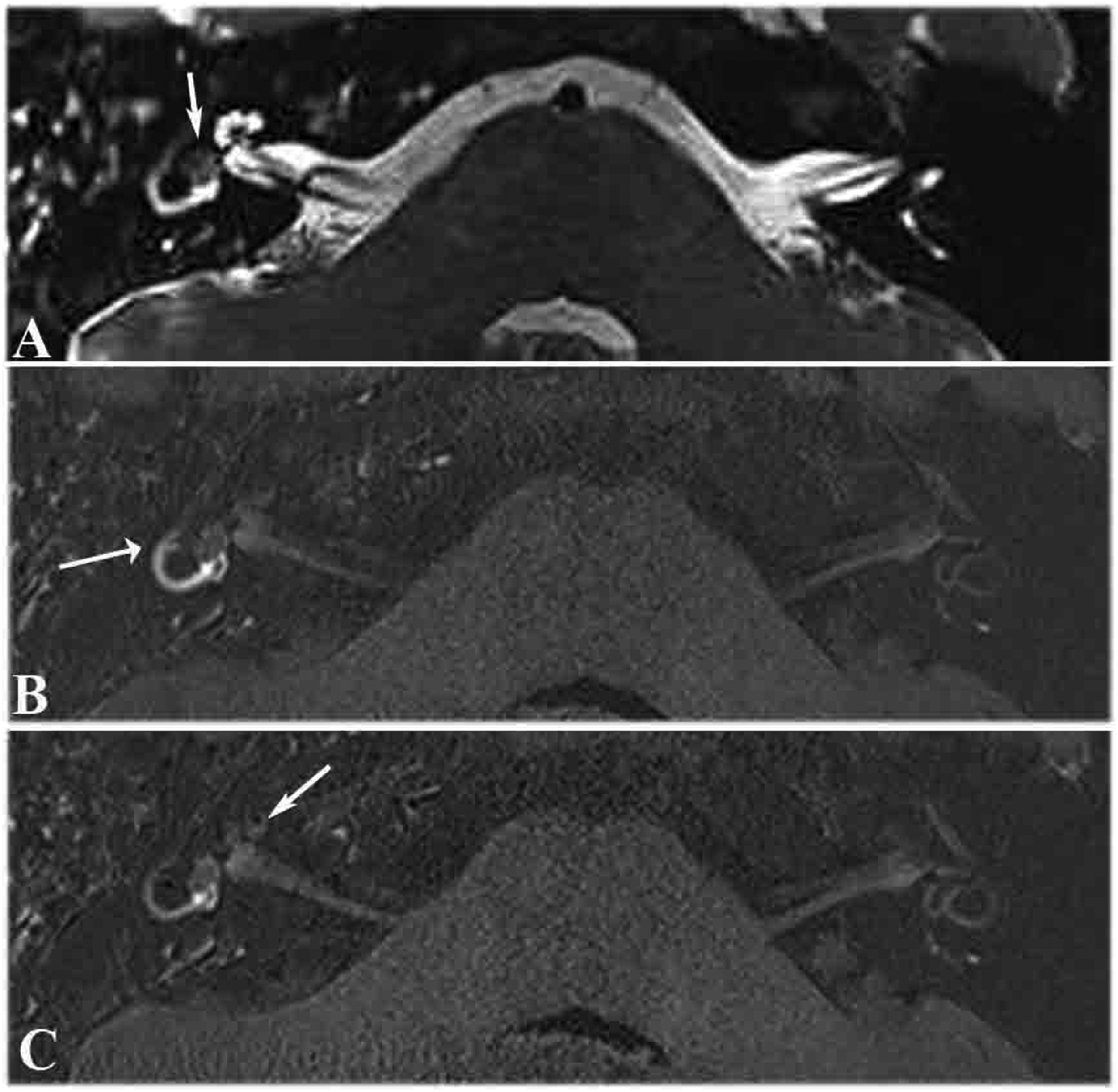
One patient had a tumor in the cochlea, in which the tumor showed cochlear filling defects on T2-SPACE images (Figure 4A), and the signal intensity of the semicircular canal and vestibule was increased on 3D real IR MRI. The patient had hearing loss for 10 years, and vertigo for 4 months (Figure 4B). MRI scans of a patient with a left cochlear tumor. (A) T2-space sequence MRI scan showing filling defects in the cochlea (arrow). (B) 3D real IR MRI scan showing the signal intensity of the semicircular canal and the vestibule was higher on the affected side than on the contralateral side (arrow).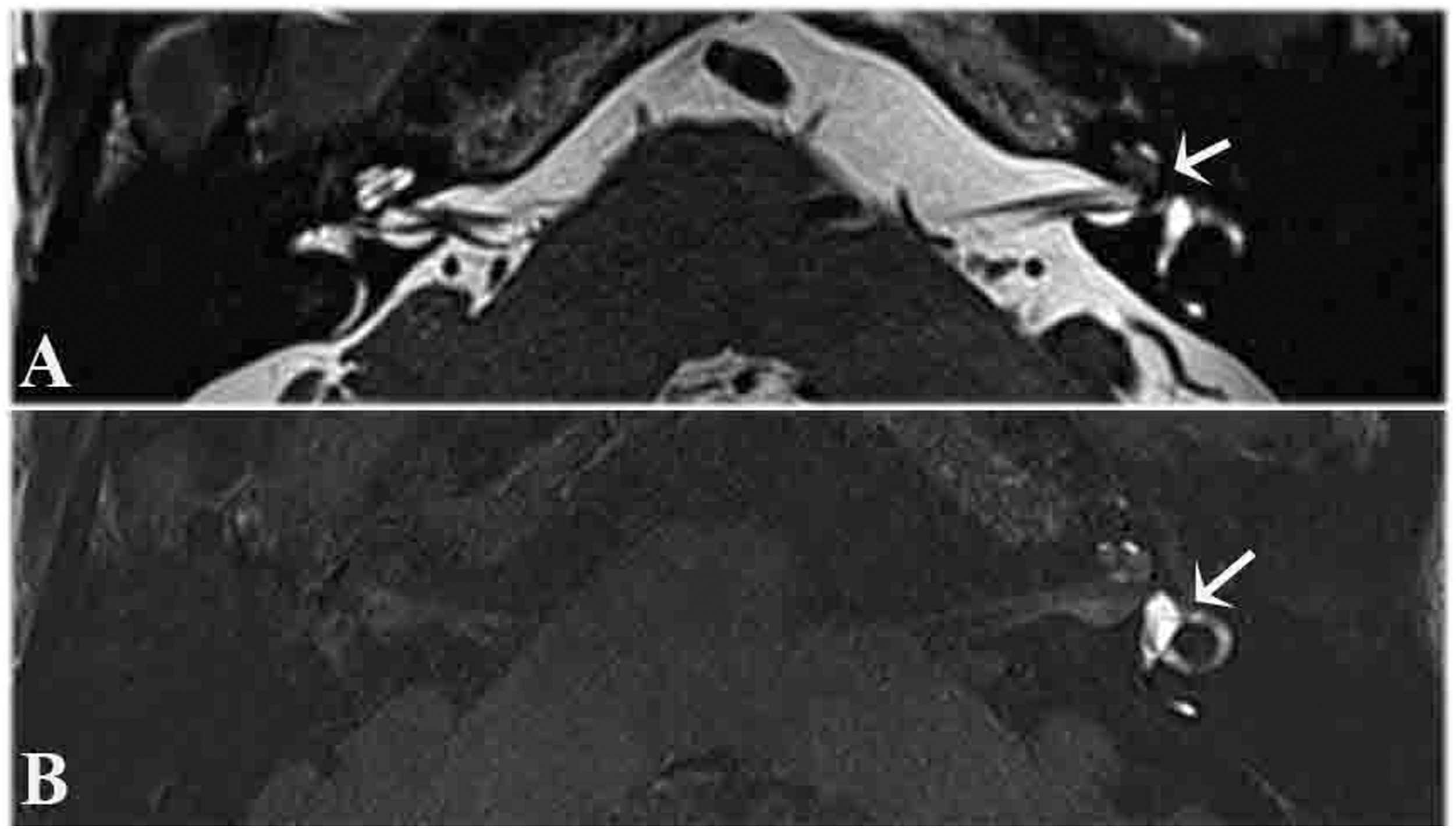
Discussion
When 3D real IR imaging was performed 4 hours after intravenous Gd injection, it is possible to clearly visualize the tumor, IAC, cochlea, and vestibule; and allows the differentiation of the endolymphatic and perilymphatic spaces; and enables a comparison between the affected and unaffected sides.11,12 In our study, this method was performed in 11 patients with AN to demonstrate the MR findings and explore the perilymph metabolism after intravenous administration of Gd.
The CSF and perilymph had similar components; previous studies reported a communication between CSF and perilymph via cochlear aqueduct. According to Kellerhals, about 20% of perilymph is derived from CSF and the remainder from the labyrinthine blood vessels 13 ; blockage of the cochlear aqueduct may reduce the flow or diffusion from CSF to the perilymph or vice versa. Moreover, several studies demonstrated a membrane between CSF and perilymph, forming a barrier between CSF and the perilymph. Nevertheless, its existence remains controversial. In our study, the cochlear aqueduct had no contrast enhancement on 3D-real-IR images, which may indicate no perilymph flows into the CSF through the cochlear aqueduct.14,15 However, whether the CSF flows or not into the perilymph via the cochlear aqueduct3,4 cannot be verified by our images. We speculated that the channel between CSF and the perilymph via the cochlear aqueduct is unidirectional. Moreover, some researchers speculated that the cochlear aqueduct is obstructed with age,16,17 which may result in no-contrast enhancement of the cochlear aqueduct.
The increased signal intensity of inner ear on 3D-real-IR images by the IV method may indicate the blood vessels of the membranous labyrinth can support the perilymph.1,2 The signal intensity of the inner ear perilymph and the fundus of the IAC significantly increased in AN that extended to the cerebellopontine angle cistern. The homogeneously increased signal intensity of the inner ear perilymph and the fundus of the IAC may indicate the IAC transports the perilymph from the inner ear for metabolism. AN might obstruct the reflux of the perilymph, resulting in elevated signal intensity of the inner ear and the fundus of the IAC. Kimura 18 found that CSF connected the inner ear via the perineural space and vascular space in the IAC. When the cochlear aqueduct is blocked, this collateral circulation is established for compensation. This view may be contributive to explain our findings.
By closely observing MRI findings, for the case with intravestibular schwannoma, the elevated signal intensity observed in the semicircular canal may indicate the perilymph can flow from semicircular canals to the vestibule and cochlea. For the patient with tumor in the cochlea, the signal intensity of the semicircular canal and vestibule was increased. It may indicate that the perilymph flows from semicircular canals and vestibule to the cochlea. 19 Overall, we speculate the pathway of perilymph flow in the AN patients from the semicircular canals through the vestibule to the cochlea, and finally flows through the IAC for metabolism.
Acoustic neuroma has variable clinical symptoms and can mimic other inner ear disorders, such as Meniere’s disease. 20 The coincidence of EH and extralabyrinthine tumors has been previously reported. 8 However, no EH was observed in the extralabyrinthine tumors evaluated in our study. Therefore, the causal relationship between EH and extralabyrinthine schwannoma remains unclear. For the case with intravestibular schwannoma, significant cochlear EH was identified in the affected ear. We speculate that tumors in the vestibule obstruct the longitudinal flow of endolymph, resulting in altered intralabyrinthine fluid flow. 21 The theory of longitudinal flow of endolymph holds that the endolymph secreted by the stria vascularis and vestibular dark cells flows through the endolymphatic duct and is then absorbed by the endolymphatic sac.22,23 However, the disruption of the vasculature by inflammation or other disturbances of endolymph homeostasis can also result in hydrops.
Apparently, there are some limitations in our study: the sample size is small, and AN presents in many different ways. We just speculated the circulatory pathway of the perilymph on the basis of the 3D real IR MRI. Therefore, further study is needed.
Conclusion
In conclusion, the elevated signal intensity observed in the semicircular canal with intravestibular schwannoma and the elevated signal intensity in the semicircular canal and vestibule with intracochlear schwannoma may indicate the perilymph flows from the semicircular canals and flows through the vestibule to the cochlea. The synchronously increased signal intensity in the inner ear and IAC may indicate that IAC may serve as a channel for removal of the perilymph in the inner ear; the blockage by the tumor may have changed the hydrodynamics of the perilymph to cause a longer retention of the Gd in the inner ear. Discovery of the metabolism of perilymphatic fluid may be contributive for the treatment of many inner-ear diseases.
Footnotes
Declaration of Conflicting Interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by National Natural Science Foundation of China (No. 81670933) and Natural Science Foundation of Shanghai (No. 20ZR1409600).