
Abstract
To explore the correlation between the width of the bony cochlear nerve canal (CNC) and long-term auditory rehabilitation after unilateral cochlear implantation (CI) in pediatric patients with congenital deafness and bilateral cochlear nerve canal stenosis (CNCS). A retrospective review was performed on 10 patients with bilateral CNCS and bilateral congenital profound hearing loss who each underwent unilateral cochlear implantation. The width of the CNC was determined on computed tomography (CT) imaging and following CI, auditory and speech performance following CI were graded using categories of auditory performance (CAP), speech intelligibility rating (SIR), and the meaningful auditory integration scale (MAIS) at 24 months following implantation. No correlation was noted between CAP score and CNCS at 24 months post CI (P > .05). A positive correlation was noted between SIR score and CNC width (ρ = .81, P < .05). Similarly, a positive correlation was noted between MAIS and CNC width (ρ = .71, P < .05). The width of the CNC in patients with CNCS is positively correlated with some long-term auditory and speech outcomes after CI.
Introduction
The bony cochlear nerve canal (CNC) transmits the cochlear nerve from the fundus of the internal auditory canal (IAC) to the base of the cochlear modiolus. Cochlear nerve canal stenosis (CNCS), first reported in 2000, is associated with varying degrees of sensorineural hearing loss (SNHL), but presents most commonly as a profound loss. 1 CNCS is typically diagnosed on computed tomography (CT) imaging, where a threshold of less than 1.5 mm is generally used for the cochlear nerve canal (CNC) to be considered stenotic. MRI may show a hypoplastic or aplastic cochlear nerve. 2 Associated abnormalities include inner ear malformations and syndromic hearing loss, although these are present in a minority of patients with CNCS. 3
Hearing rehabilitation in patients with CNCS depends in a large part on contralateral hearing status. When a bilateral profound loss is present, cochlear implantation (CI) is the preferred method of hearing rehabilitation. 4 CI outcomes in patients with CNCS have not been fully elucidated. In an earlier report, patients with CNCS undergoing CI demonstrated increased electrocochleography thresholds, with many patients deriving significant benefit. 5 This indicates that CIs are effectively able to stimulate the cochlea and produce a measurable neural response in these patients, but that they require a higher current to do so.
In this study, we discuss our experience with a series of patients with bilateral CNCS who underwent unilateral CI for hearing rehabilitation. We correlate long-term speech and language outcomes, as measured by categories of auditory performance (CAP), speech intelligibility rating (SIR), and infant-toddler meaningful auditory integration scale (IT-MAIS) with the diameter of the cochlear nerve canal.
Materials and Methods
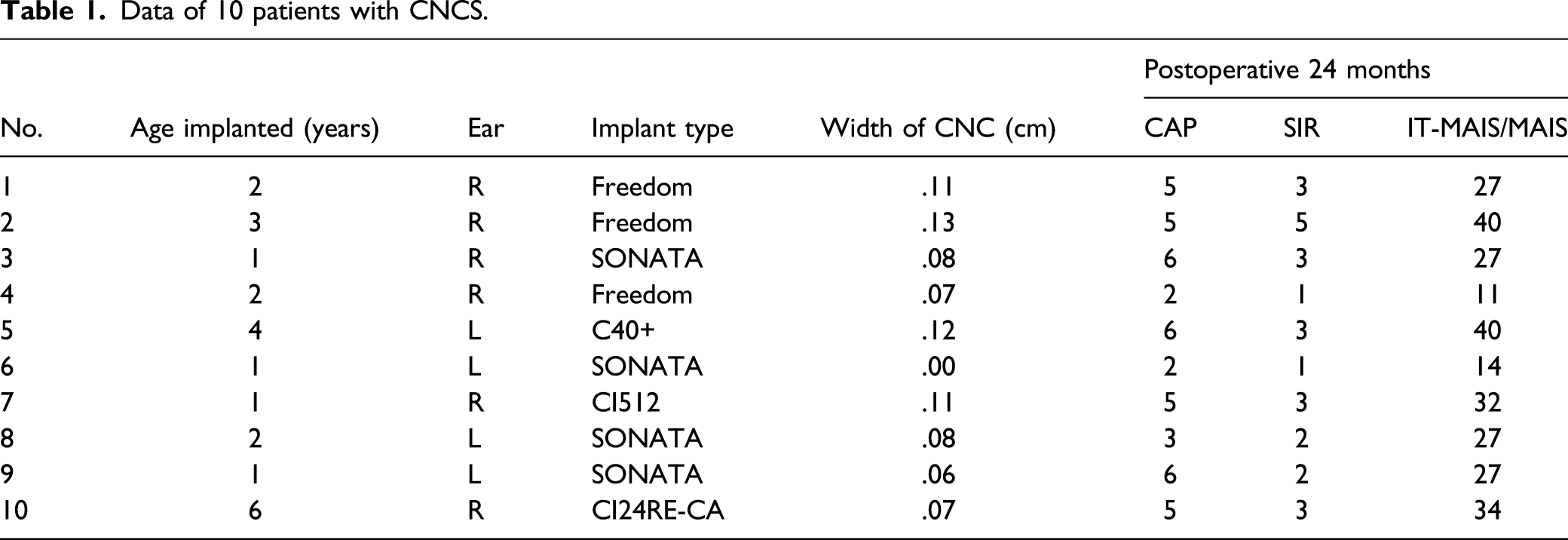
Institutional review board approval was obtained for this study. Inclusion criteria were patients with bilateral profound hearing loss, bilateral CNCS on CT imaging, and normal inner ear morphology who underwent unilateral CI (shown in Figure 1). The choice of ear to be implanted was determined by a consensus between audiology and otology based on a variety of factors individualized to each patient within the study population. Factors included residual hearing amenable to hearing aid use in one or both ears and CNC diameter; in general, the ear with a larger CNC diameter was implanted. Exclusion criteria were medical comorbidities and presence of inner ear malformations. A retrospective review was performed of patients meeting criteria within the study period December 2012 to May 2017; 10 patients were identified (shown in Table 1). Stenosis of the bony cochlear nerve canal (CNC). In this patient, the CNC measures 1.1 mm (normal, >1.5 mm). Data of 10 patients with CNCS.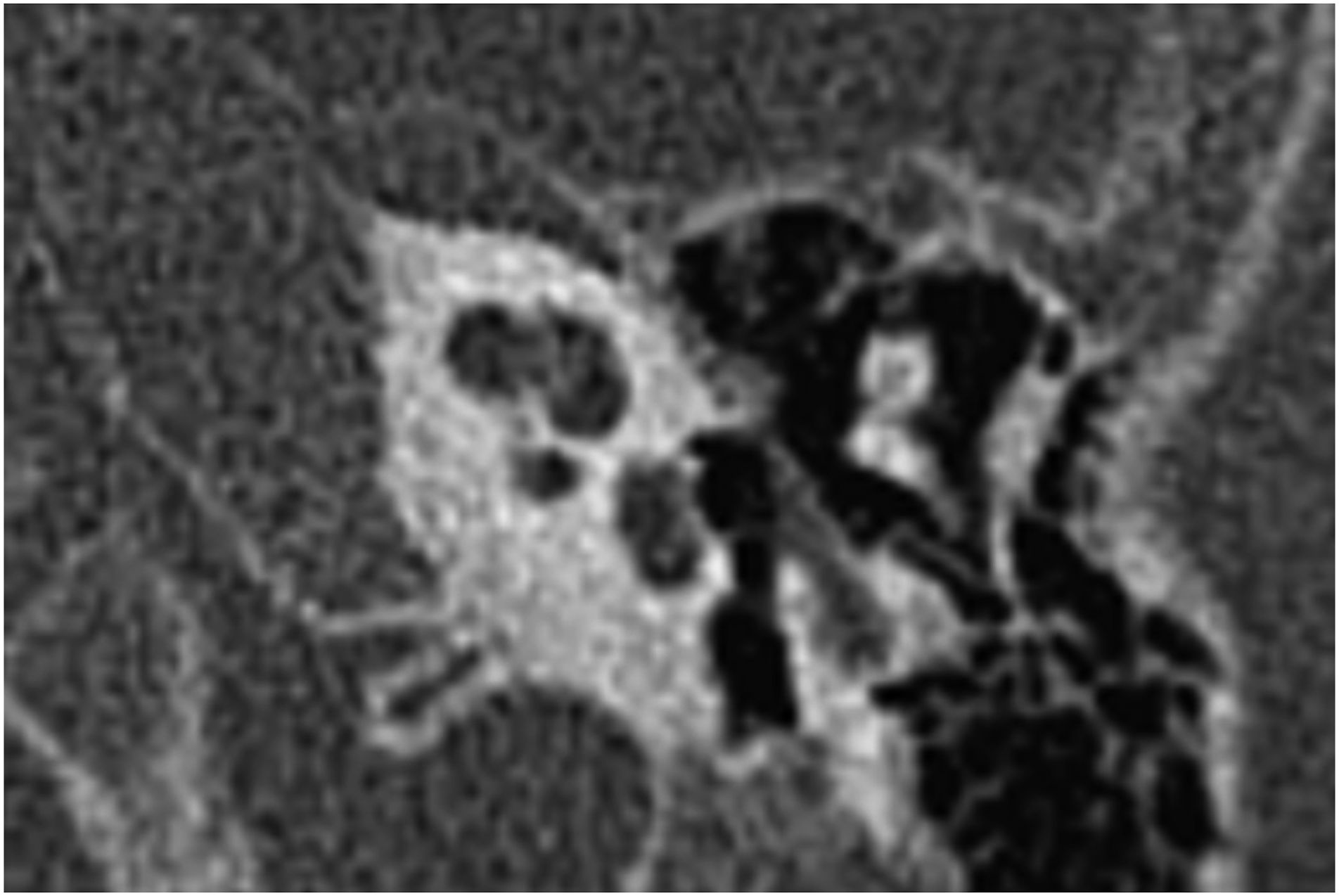
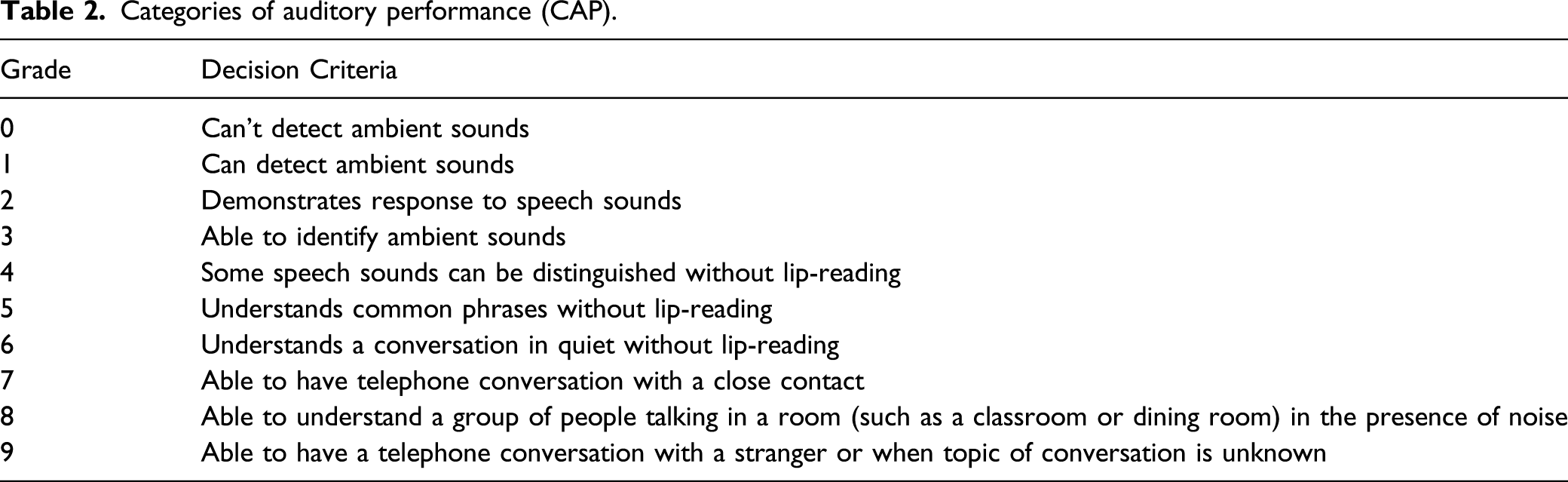
Categories of auditory performance (CAP).
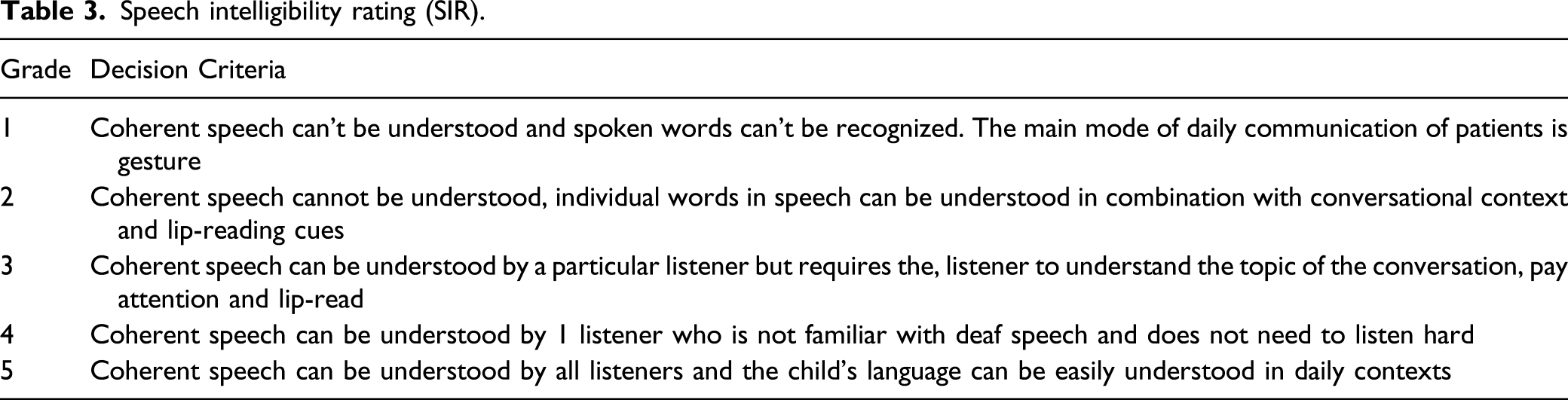
Speech intelligibility rating (SIR).
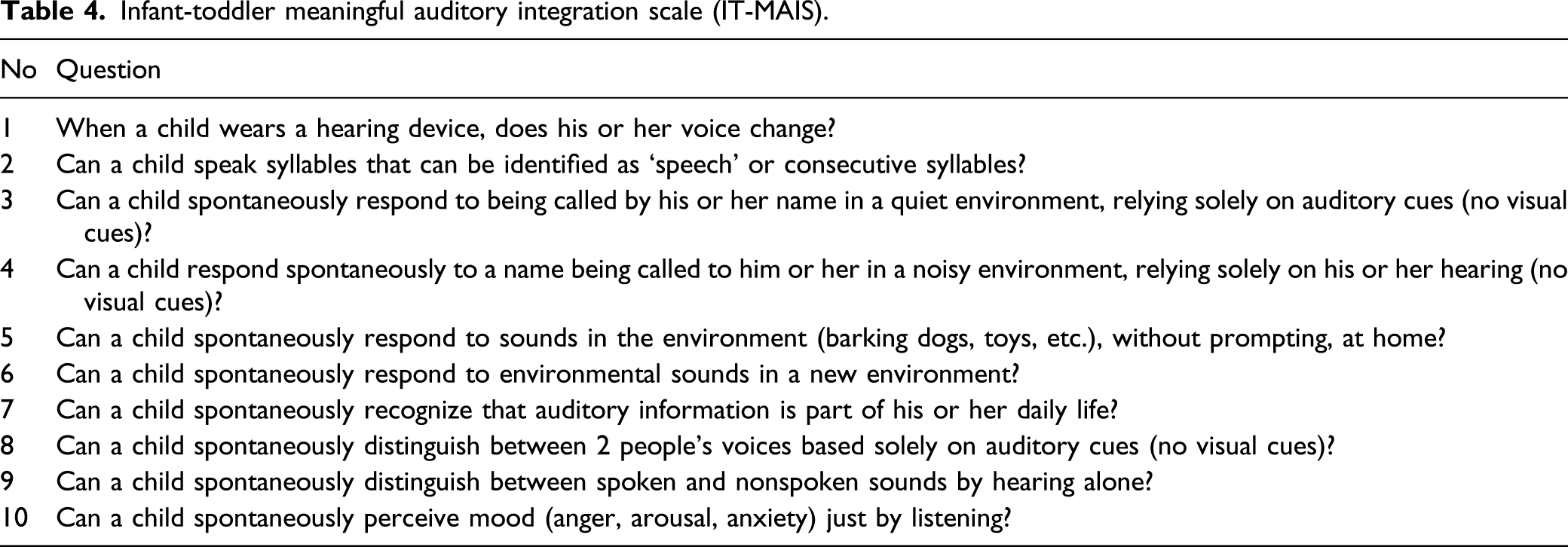
Infant-toddler meaningful auditory integration scale (IT-MAIS).
Spearman correlation was performed with SPSS 22.0 (IBM, Armonk, New York) to investigate the relationship between CNC diameter and test parameters.
Results
Ten patients (7 male and 3 female) with bilateral CNCS and bilateral profound hearing loss underwent unilateral cochlear implantation at a mean age of 2.3 years (standard deviation [SD], 1.6 years). The mean CNC diameter on preoperative CT imaging as was .83 mm (SD 0.04 mm). Both Cochlear (NSW, Australia) and Med-EL (Innsbruck, Austria) devices were used. The right ear was implanted in 6 patients, and the left ear was implanted in 4. There were no perioperative complications noted.
Correlation between width of cochlear nerve canal and CAP, SIR, and MAIS/IT-MAIS scores.
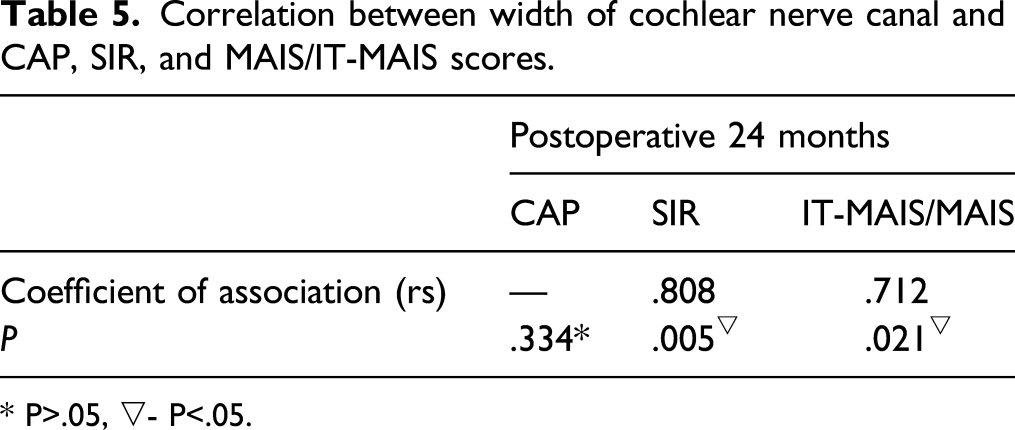
* P>.05, ▽- P<.05.
Discussion
Cochlear nerve canal stenosis (CNCS) is associated with congenital hearing loss and can occur unilaterally or bilaterally. When CNCS is present bilaterally, the most common presentation is congenital deafness. CNCS has been associated with cochlear nerve hypoplasia and aplasia as well as labyrinthine abnormalities.
In this series, patients with bilateral CNCS, normal inner ear morphology, and without medical or syndromic comorbidities underwent unilateral cochlear implantation for rehabilitation of deafness. We found that these patients generally derived significant benefit from unilateral CI. Performance in this cohort approximated results seen in CI performed in congenitally deaf peers without CNCS. 6
We further sought to correlate post-implant auditory and speech performance with the diameter of the CNC. The speech intelligibility rating scale and meaningful auditory integration scale were both significantly positively correlated with cochlear nerve canal diameter (rs=.81 and .71, respectively). Categories of auditory performance demonstrated no correlation. This suggests that patients with a larger cochlear nerve canal diameter may demonstrate better post implant performance. This finding is similar to the observation that patients with smaller CNC diameters demonstrate poorer word performance. 7 Although the observed correlation does not imply causation, it is possible that a larger CNC diameter transmits more intact cochlear nerve fibers from the internal auditory canal to the cochlea. This would certainly be a possible explanation for the improved results noted in patients with larger CNC diameters. Another explanation is that electrophysiologic differences within the cochlea and/or auditory nerve associated with CNC diameter, independent of cochlear nerve fiber count, lead to better auditory performance.
MAIS/IT-MAIS is a scale used for children over 3 years of age and children under 3 years of age, respectively, to evaluate meaningful use of sound in daily life by hearing-impaired children. SIR is a scale used to rate the overall intelligibility of a patient’s speech. CAP is a scale used to rate the outcomes of pediatric CI patients in daily life. These 3 scales provide complementary information about the specific and global benefits of implantation in children. Our findings demonstrated a positive correlation between CNC diameter and MAIS/IT-MAIS, SIR and no correlation between CNC diameter and CAP. This may be explained by the fact that our patient population remains relatively heterogeneous and auditory perceptive performance demonstrated significant variability across subjects. However, better overall performance, as well as better speech, was noted for patients with larger CNC diameters. This may generally suggest improved overall outcomes after implantation with larger CNC diameters.
We did not note any perioperative or postoperative complications in this short series. Previous research has suggested that patients with CNCS undergoing CI have a higher incidence of facial nerve stimulation, but this was not observed in our study. 8
The present research is valuable for patient counseling. In clinical practice, if a cochlear nerve canal significantly smaller than the generally accepted threshold of 1.5 mm for CNC stenosis is encountered, a patient’s family may be counseled that cochlear implant outcomes are more guarded. However, contrary to some prior reports, CNCS is not an absolute contraindication to cochlear implantation. Rather, the findings in the present work are in agreement with previous research, suggesting that cochlear implant outcomes in patients with CNCS lie along a spectrum of varying degrees of performance. 9
One limitation of the study is that magnetic resonance imaging (MRI) was not performed for the patients. If MRI results had been uniformly available, the observed performance could also be correlated with the appearance or diameter of the cochlear nerve within the IAC. While the authors’ institutions now routinely utilize MRI as part of the evaluation process for pediatric patients undergoing CI, our referral network includes many practice locations where MRI is difficult to impossible to perform prior to the patients arriving at our tertiary centers. Therefore, it is beneficial for referring centers without MRI access to note that pediatric patients with profound loss and CNCS on CT imaging may well be CI candidates, regardless of MRI status. Another limitation of the study is the lack of consistent longitudinal follow-up on these patients, including long-term follow-up after 24 months post-implantation, as this could potentially reveal eventual improvements in poor performers. Finally, a prospective investigation of patients with CNCS with hearing loss could shed further light on the overall auditory performance and help select the best candidates for cochlear implantation in this population.
Conclusion
Cochlear nerve canal stenosis (CNCS) is associated with profound hearing loss. When deafness associated with bilateral CNCS is present, an increased CNC diameter in the ear to be implanted is associated with better auditory performance. The CNC is easily seen on computed tomography imaging, and should be measured prior to implantation to aid in patient counseling.
Footnotes
Author Contributions
Si Zhang provided substantial contributions to the conception of the work, drafted the work, gave final approval of the version to be published, and agrees to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved. Line Wang provided substantial contributions to the design of the work, drafted the work, gave final approval of the version to be published, and agrees to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved. Sushing Gong provided substantial contributions to the acquisition, analysis, and interpretation of the data for the work, drafted the work, gave final approval of the version to be published, and agrees to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved. Pao Liu provided substantial contributions to the acquisition, analysis, and interpretation of the data for the work, drafted the work, gave final approval of the version to be published, and agrees to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved. Xinyu Song provided substantial contributions to the acquisition, analysis, and interpretation of the data for the work, drafted the work, gave final approval of the version to be published, and agrees to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved. Qimei Wang provided substantial contributions to the conception of the work, drafted the work, gave final approval of the version to be published, and agrees to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved. Wie Wang Zhang provided substantial contributions to the design of the work, drafted the work, gave final approval of the version to be published, and agrees to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved. Hannah Landsberger provided substantial contributions to the conception of the work, revised the work critically for important intellectual content, gave final approval of the version to be published, and agrees to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved. Kevin A. Peng provided substantial contributions to the conception and design of the work, drafted the work, gave final approval of the version to be published, and agrees to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported in part by Beijing Municipal Science and Technology Commission (Applied Technology Research and Development Project) (No. Z191100007619043).
Ethical approval
This study was conducted ethically in accordance with the World Medical Association Declaration of Helsinki. This study protocol was reviewed and approved by the IRB of the Beijing Friendship Hospital, Capital Medical University, approval number 2020-P2-125-01.
Informed consent
Written informed consent was obtained from the subjects’ parents.