
Abstract
Introduction
Hemangioma is a relatively common congenital vascular malformation in clinical practice, but rare in the hypopharynx. Because hemangiomas tend to grow continuously and may cause uncontrollable bleeding due to local stimulation, aggressive treatment is generally required.1,2 The common treatment methods of hemangioma include surgical resection, sclerotherapy, laser, corticosteroid, and propranolol.1,3–8
Due to the specificity of anatomical location, the exposure of hypopharyngeal hemangioma is always difficult, and the operative field is small. In addition, intraoperative hemorrhage is prone to occur and hard to stop. Therefore, the surgical treatment for hypopharyn geal hemangioma is always difficult and risky.8,9 Compared with surgical resection, local sclerotherapy injection has many advantages, such as simple operation and minimal invasion, and has been gradually widespread used in clinical practice.10,11
Lauromacrogol is a new type of vascular sclerosant in recent years; it has the effect of promoting vascular fibrosis and thrombosis, and has a slight anesthetic effect. Up to now, lauromacrogol is mainly used in the sclerotherapy of esophageal and gastric varicose veins. 12 For the past few years, we have used endoscopic-assisted lauromacrogol injection in the treatment of hypopharyngeal hemangioma and achieved satisfactory therapeutic effects.
Patients and Methods
This study was approved by the Ethics Committee of Affiliated Hospital of Jiangnan University. Informed consent was obtained from all individual participants included in the study.
Clinical Data
Clinical Data of 13 Cases of Laryngopharyngeal Hemangioma.
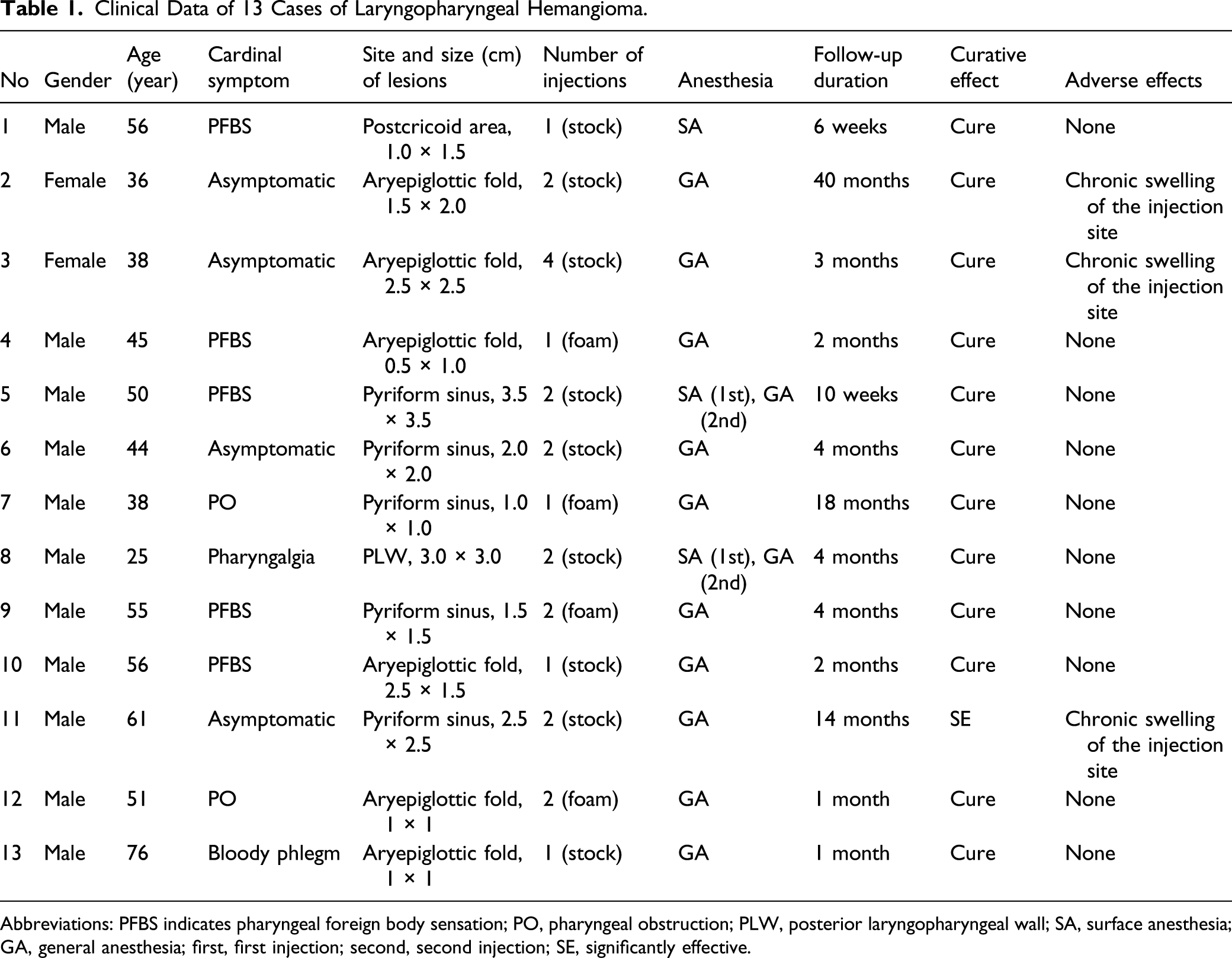
Abbreviations: PFBS indicates pharyngeal foreign body sensation; PO, pharyngeal obstruction; PLW, posterior laryngopharyngeal wall; SA, surface anesthesia; GA, general anesthesia; first, first injection; second, second injection; SE, significantly effective.
Therapeutic Procedures
The procedure was performed under surface or general anesthesia. For the patients undergoing surface anesthesia, 1% ephedrine and nitrofurazone nasal drops were used for nasal contraction and 1% tetracaine was used for nasal and pharynx spray 3 times with 5 minute intervals. After satisfactory anesthesia, the drug was injected through the mouth with a long needle bent to a suitable bend under the guidance of a flexible laryngoscope. For general anesthesia, the hemangioma was exposed with a suspension laryngoscope through the oral cavity and injected with a long needle under the guidance of a rigid laryngeal endoscope.
Of the 13 patients, 9 were injected with stock lauromacrogol solution and 4 with lauromacrogol foam. For lauromacrogol foam injection, the Tessari method was used to produce foam with a liquor–gas ratio of 1:4.13,14 Once the lauromacrogol foam was made, it was injected as soon as possible.
We used single-point injection to treat hemangioma with small volume. The injection needle was inserted into the most prominent part of the tumor. After blood was extracted, the medication was slowly injected into the tumor until the surface mucosa turned slightly white and a little drug leaked out. For larger-volume hemangiomas, multi-points injection was used which usually started from the periphery of the tumor, with 1 injection at each of the 4 edges of the tumor and 1 at the center of the tumor. After injection, if there was active bleeding, hemostasis was performed by pressing the bleeding site with a cotton ball soaked with 0.1% epinephrine. Patients were reexamined once a week postoperatively, repeated the injection 4 weeks later if there was any residual tumor.
Evaluation Criteria for Therapeutic Effect
By referring to the new response evaluation criteria in solid tumors (RECIST), 15 electronic laryngoscopy was performed 1 to 2 months after the last injection, and the therapeutic effect was evaluated according to the changes of tumor size and mucosal color: (1) Cure: the tumor completely disappeared and the mucosal color was normal; (2) Significantly effective: the tumor shrank by more than 50%, and the mucosa color was close to normal; (3) Improved: the tumor shrank less than 50%, and the mucosa color became lighter; and (4) Ineffective: the size and appearance of the tumor were not significantly changed.
Results
The 13 patients were followed up for 1 month to 40 months; 12 were cured and 1 was significantly effective. 5 patients received 1 injection, 7 received 2, and 1 received 4. 2 patients with large hemangioma underwent prophylactic tracheotomy due to obvious glottic swelling after injection. Because of diffuse swelling at the injection site (left aryepiglottic fold) and obvious epiglottis edema 15 minutes after the injection, one patient was forced to retain endotracheal intubation when returned to the ward. The intubation was removed on the second day after surgery when the local swelling was significantly reduced by electronic laryngoscopy. No dyspnea occurred in the other patients.
All 13 patients had different degrees of pharyngalgia or pharyngeal foreign body sensation after injection; no adverse reactions such as postoperative bleeding, local mucosal ulceration, fever, and allergy were found. 3 patients had chronic swelling at the injection site after injection. The 2 patients who underwent tracheotomy were successfully extubated after treatment.
Typical Case
A female patient of 36 years old who was hospitalized after the discovery of neoplasm in the throat during an electronic gastroscopy. The patient had no symptoms such as pharyngeal foreign body sensation, dysphagia, and bloody phlegm. Further electronic laryngoscopy revealed a purplish red neoplasm with uneven surface and unclear boundary in the left aryepiglottic fold and pyriform sinus, which invaded the interarytenoid area (Figure 1A). Laryngoscopy images of a patient with larygopharyngeal hemangioma undergoing lauromacrogol sclerotherapy. (A) Preoperative electronic laryngoscope showing a purplish red neoplasm in the left aryepiglottic fold and pyriform sinus which invaded the interarytenoid area. (B) Laryngoscopy image 1 month after the 1st injection. (C) 1 month after the second injection. (D) 2 months after the second injection. (E) 40 months after the second injection.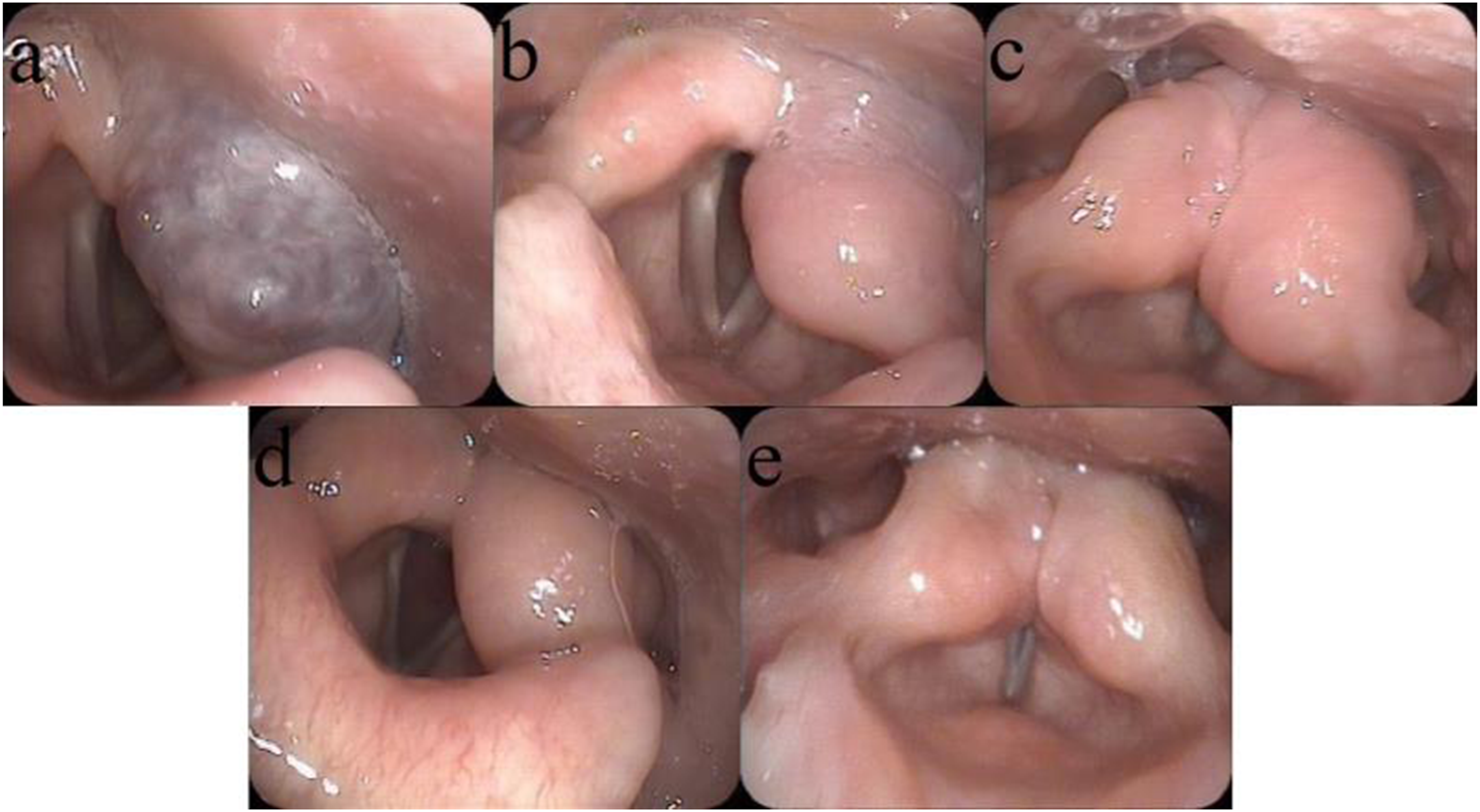
The injection was performed with the assistance of a suspension laryngoscope under general anesthesia, lauromacrogol was injected with a dose of 8 mL, and a prophylactic tracheotomy was performed after the injection. Four weeks after first injection, electronic laryngoscopy showed that the hemangioma was significantly reduced, but the left aryepiglottic fold was obviously swollen and the lilac neoplasm could still be seen in the postcricoid area and interarytenoid area (Figure 1B). Lauromacrogol was injected again under the suspension laryngoscope with a dose of 4 mL. One month after the second injection, electronic laryngoscopy showed obvious swelling of bilateral aryepiglottic fold and complete disappearance of hemangioma (Figure 1C). Two months after the operation, bilateral aryepiglottic folds were still mild swelling, but the color of surface mucosa was normal and the bilateral vocal cords moved well (Figure 1D). The patient was breathing well and stable, so the tracheal tube was removed. Now the follow-up lasted for 40 months, and no sign of recurrence was observed (Figure 1E).
Discussion
In the past, pingyangmycin was the most commonly used agent for sclerotherapy treatment of hemangioma. Pingyangmycin is a broad-spectrum anti-tumor drug, which can treat hemangioma mainly by inhibiting the DNA synthesis of vascular endotheliocyte, affecting the metabolic function of sinusoid endotheliocyte, and then causing vascular degeneration, necrosis, fibrosis, and finally causing tumor decline. However, the use of pingyangmycin injection in the treatment of hemangioma has the following disadvantages: (1) The incidence of adverse reactions and complications in the treatment of hemangioma by pingyangmycin injection was as high as 11.61%, mainly including local ulceration and necrosis, inappetence, fever, rash, anaphylactic shock, etc. (2) In addition, it may cause pulmonary fibrosis in multiple injections or at high cumulative doses.16-18 To a certain extent, the disadvantages mentioned above limit the clinical application of pingyangmycin in the treatment of hemangioma.
The chemical name of lauromacrogol is lauryl alcohol polyoxyethylene. As a new sclerosis agent, lauromacrogol can directly damage vascular endothelium, promote thrombosis, and further cause tissue fibrosis, thus causing vascular occlusion and tumor atrophy. In recent years, lauromacrogol has been applied in the treatment of hemangioma, and literature has reported significant efficacy without obvious adverse reactions.10,16,18 To the best of our knowledge, this study is the first English report on the treatment of laryngopharyngeal hemangioma with lauromacrogol injection. In the above-reported cases, all 13 patients were cured except for 1 patient with a little residual under the mucosa, and no other complications were found except swelling of the injection site.
Selection of Treatment Methods
The injection methods used in this study mainly included flexible laryngoscope-guided injection under surface anesthesia and suspension laryngoscope-assisted injection under general anesthesia. Among the patients in this group, 3 patients received flexible laryngoscope-guided injection under surface anesthesia. In 1 of the patients, the tumor disappeared after 1 injection. The other 2 patients switched to suspension laryngoscope-assisted surgery under general anesthesia due to the poor effects after the first injection.
Although flexible laryngoscope-guided injection under surface anesthesia has the advantages of simple operation and low cost, it also has the following disadvantages: (1) The operation process needs the patient’s close cooperation. If the patient is too nervous and the pharyngeal reflex is too sensitive, the injection is difficult to carry out. (2) Deep hemangioma is difficult to be accurately located during injection which may affect the efficacy of injection. (3) It is difficult to stop bleeding if intraoperative bleeding occurs. Compared with flexible laryngoscope-guided injection under surface anesthesia, local injection of hemangioma can be performed accurately assisted by suspension laryngoscope under general anesthesia, without the cooperation of patients. Once bleeding occurs at the injection site, local compression can be performed with a cotton ball containing epinephrine to effectively stop the bleeding. In addition, precise and multi-point injections can be carried out to the tumor, thus increasing the injection volume of sclerosing agent, enhancing the efficacy, and reducing the number of injections. Therefore, suspension laryngoscope-assisted injection under general anesthesia is suggested especially for cases with deep location and large volume.
Injection Method and Interval
Lauromacrogol can be injected as a stock solution, or can be made into a foam solution for injection. It has been reported that compared with the stock lauromacrogol solution, foam sclerosant has more advantages: First, the cavitation effect of foam increases the contact area between the sclerosant molecule and the vascular wall, and lauromacrogol foam is easy to stay in the blood vessel, which can slow the flow of drugs in the blood vessel and eventually increase the contact time between the drug and the vascular endothelial cells. Second, the foam has the effect of expelling blood and can drain blood from the tumor to avoid the blood dilution of lauromacrogol and increase its concentration in the tumor. 14 However, in a study of hepatic hemangioma, the results suggested that both lauromacrogol injection methods were safe and equally effective. 19 There have been no previous reports of lauromacrogol foam injection for laryngopharyngeal hemangioma. In this group of cases, only 4 patients received lauromacrogol foam injection, so it was not possible to evaluate the advantages and disadvantages of the 2 injection methods. However, when using lauromacrogol foam injection, the drug dose was significantly reduced, which was conducive to reducing treatment-related complications.
As for the interval time of lauromacrogol injection, Liu suggested that the interval between injections be 1 week. 10 But in clinical practice, we found that the local swelling of the tumor was severe 1 week after injection, and it was difficult to judge the effect and determine the sites and range of reinjection. According to our observation, the local swelling could be significantly subsided after 4 weeks. Therefore, we have chosen to re-inject at an interval of 4 weeks if needed.
Although our preliminary clinical studies have suggested that lauromacrogol injection has a good effect in the treatment of laryngopharyngeal hemangioma, this study has several limitations. First, because the incidence rate of hypopharyngeal hemangioma is very low, the sample size of this study is relatively small and there is no comparison group. Second, the follow-up time of some cases in this study is short, and the long-term treatment effect needs to be further observed.
Conclusion
In conclusion, lauromacrogol injection can be used as a safe and reliable method for the treatment of laryngopharyngeal hemangioma. However, the long-term efficacy, optimal injection dose, and injection interval need to be further studied.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by the Top Talent Support Program for young and middle-aged people of Wuxi Health Committee (BJ2020043).