
Abstract
Introduction
Interstitial thermal ablation can be performed for treating both benign and malignant neoplasm lesions in the head and neck.1-6 In general, the success of interstitial thermal ablation depends upon accurate insertion of the ablation probe into the target lesion, real-time monitoring of the effects of the treatment, and subsequent evaluation of the extent of thermal tissue damage. 6 In order to optimize the safety of the thermal ablation, magnetic resonance (MR) thermography is typically implemented during the procedure.
Magnetic resonance thermography is a validated non-invasive imaging technique that can provide accurate temperature monitoring during thermal ablation.6,7 Several MR thermography methods have been developed, including sequences based on proton resonance frequency (PRF), the diffusion coefficient, T1-and T2-relaxation times, magnetization transfer, and proton density.7,8 In particular, PRF techniques exploit temperature-induced effects of chemical shift, in which the temperature difference is directly proportional to the phase difference. This method provides accurate temperature measurements in the range of interest for thermal ablation. 8
The purpose of this study is to objectively characterize the image quality of phase contrast MR thermography sequences in patients with head and neck tumors for planning interstitial thermal ablation procedures.
Materials and Methods
Patients
This single-institution retrospective study included adult patients with head and neck tumors who underwent magnetic resonance imaging (MRI) exams that included MR thermography sequences. Patients with cutaneous and orbital neoplasms, as well as lipomatous tumors, were excluded from this study. Institutional review board approval was obtained for this study.
MRI Parameters
Axial MR thermography images were acquired on a 3T MRI system (Ingenia dStream; Philips Healthcare, Best, the Netherlands) using a head and neck neurovascular coil in conjunction with routine clinical head and neck MRI sequences. The MR thermography sequence used the following parameters: TR: 30 ms, TE: 10 ms, flip angle: 19.5°, slice thickness: 3.0 mm, number of excitations: 1, matrix size: 252 × 126, and field of view: 240 mm.
Signal-to-Noise Ratio Calculation
Signal-to-noise ratio (SNR) was calculated for each of the head and neck lesions depicted on MR thermography images according to the following equation

Contrast-to-Noise Ratio Calculation
For each head and neck lesion, contrast-to-noise ratio (CNR) was calculated from MR thermography images according to the following equation

Statistical Analysis
The ranges and standard deviations of the lesion area, SNR, and CNR were determined in each patient. In addition, the Pearson correlation coefficients between SNR and CNR and between lesion area and SNR were calculated. A P-value of less than .05 was considered to be statistically significant.
Results
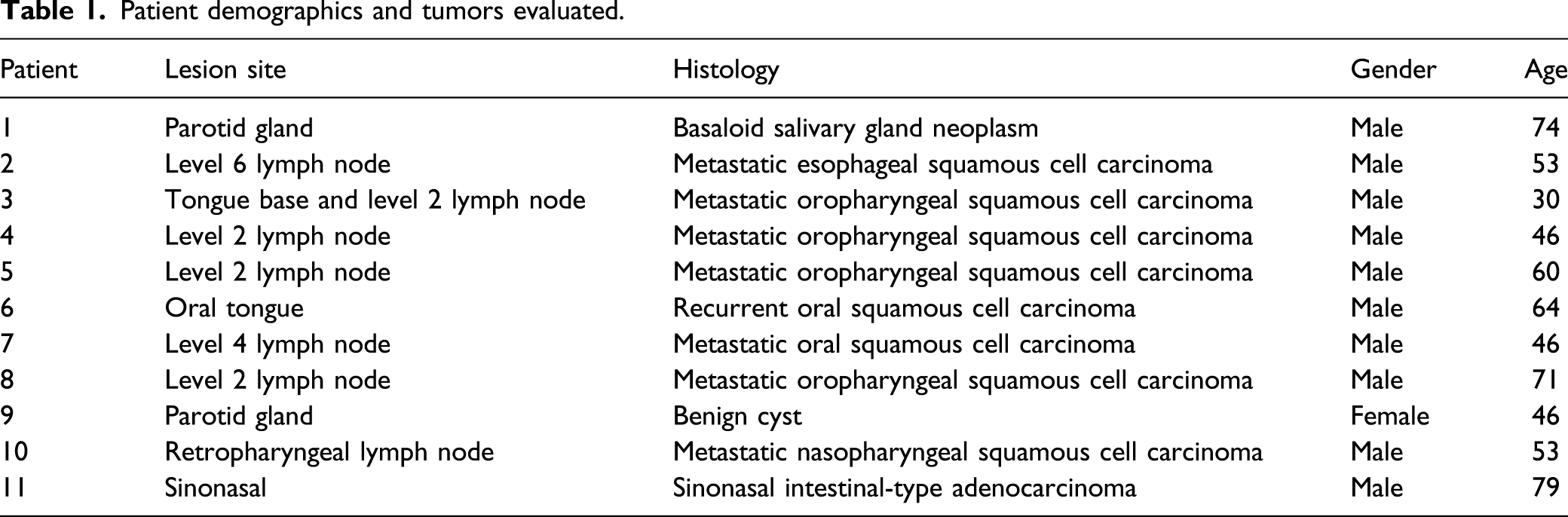
Patient demographics and tumors evaluated.
Lesion size, SNR, and CNR.
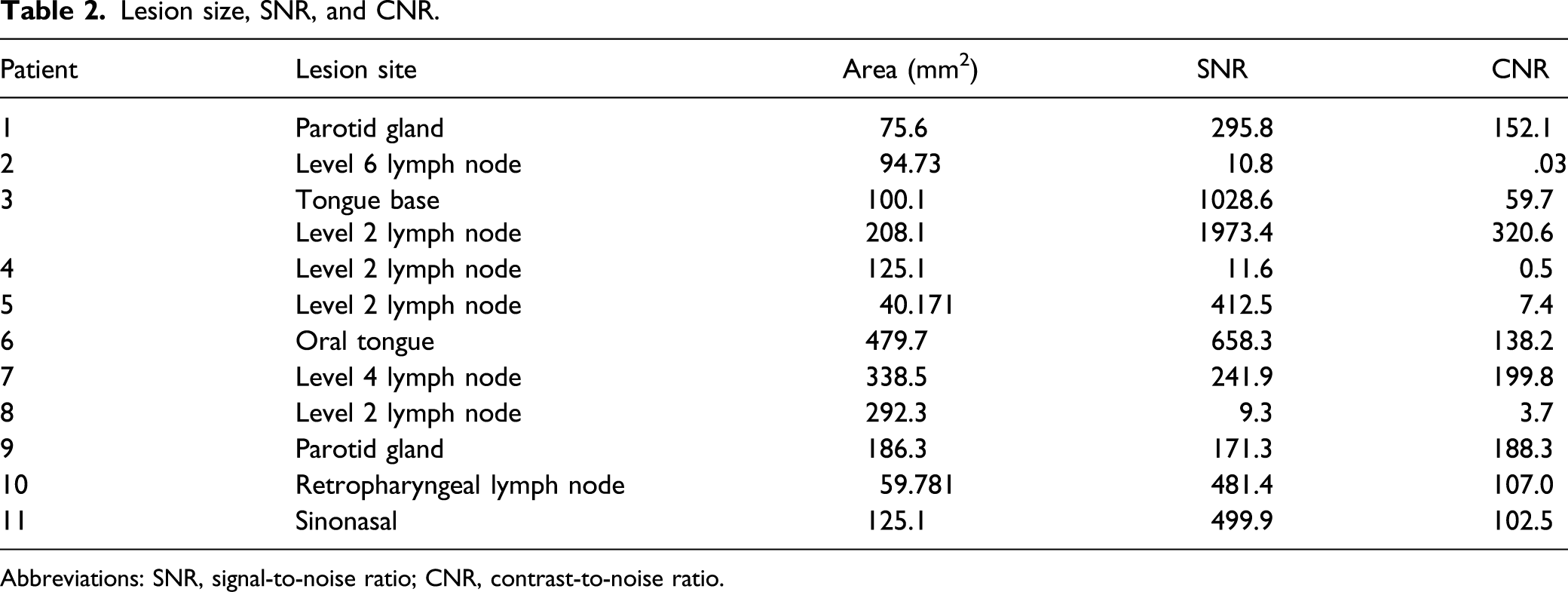
Abbreviations: SNR, signal-to-noise ratio; CNR, contrast-to-noise ratio.
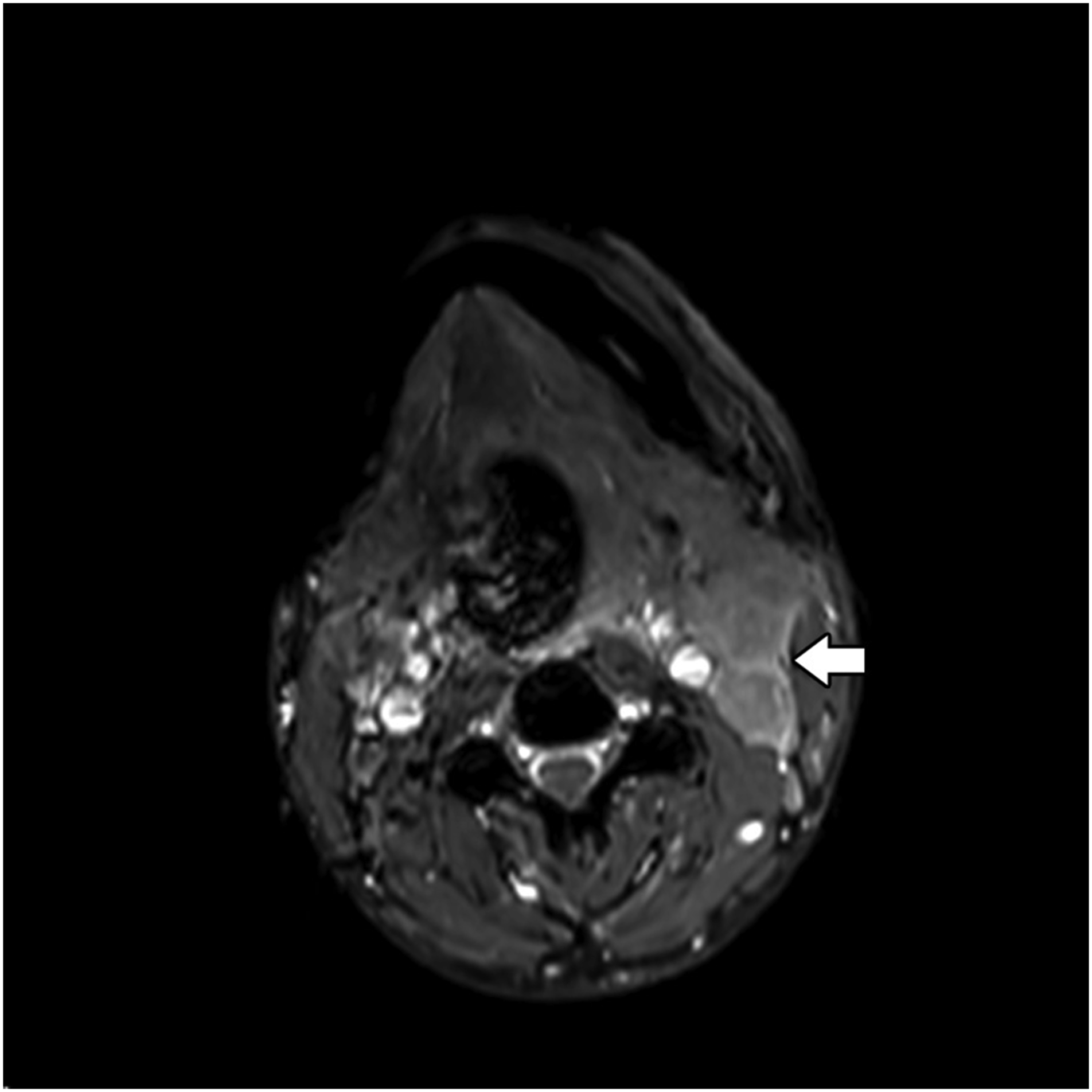
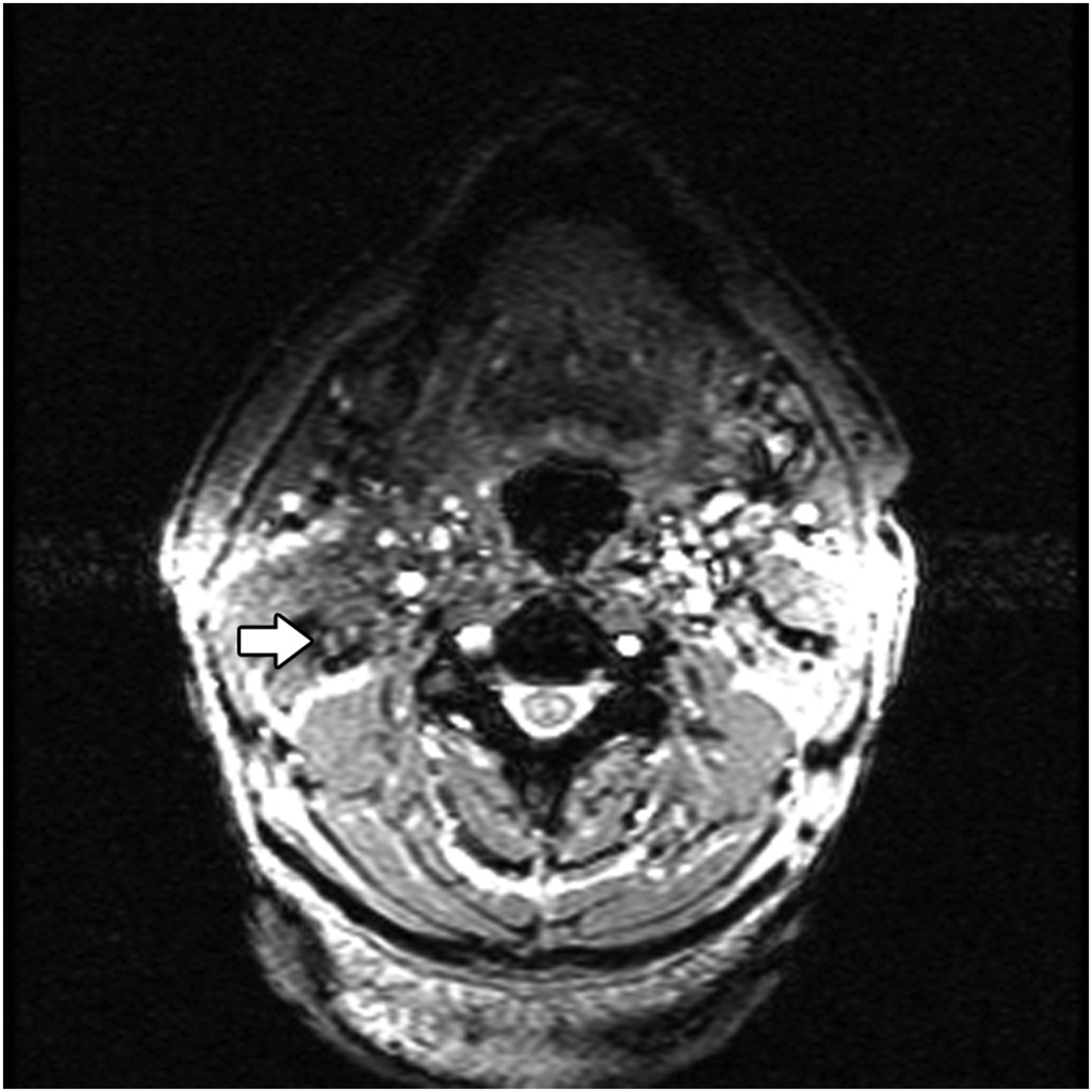
Axial MR thermography image shows left level 2 lymphadenopathy (arrow) with SNR of 1973.4 and CNR of 320.6. The images are sharp and homogeneous. Abbreviations: MR, magnetic resonance; SNR, signal-to-noise ratio; CNR, contrast-to-noise ratio.
Axial MR thermography image shows right level 6 lymphadenopathy with SNR of 10.8 and CNR of .03. The images are inhomogeneous and there is noticeable pulsation artifact. Abbreviations: MR, magnetic resonance; SNR, signal-to-noise ratio; CNR, contrast-to-noise ratio.
Discussion
This study shows that the image quality of MR thermography of head and neck lesions can vary considerably in terms of SNR and CNR, which are important parameters for performing MR thermography-guided interstitial tumor ablation. Therefore, it is important to obtain this sequence as part of a thermal ablation planning scan to ensure that its quality would be adequate for use during the procedure. For example, lesions with SNR of less than 100 have a temperature uncertainty of greater than 3°C, 11 which was the case for 25% of the lesions in this series.
Interestingly, there was substantial variability among lesions in similar regions, such as the level 2 lymph nodes. On the other hand, good image quality could be achieved in different areas of the head and neck, such as the sinonasal region, despite the possibility of degradation from susceptibility effects at the air-soft tissue-skull base interfaces. In addition, it does not appear that lesion size significantly affects the SNR measurements. However, there was a significant correlation between SNR and CNR of the lesions. Thus, one of these parameters could potentially be used as a surrogate for the other in order to save time and effort for the quality assessment. In particular, SNR could be considered a more relevant parameter because anatomic imaging is otherwise used for the probe insertion and the lesions tend to be more conspicuous on T1-weighted and T2-weighted sequences.
Aside from adipose tissue, the PRF thermal coefficient is relatively unaffected by tissue type and has a minor dependence on thermal history even for coagulated tissue. 12 Thus, it is unlikely that the variability of SNR and CNR measurements were attributable to the particular lesion histology in this series since fat-containing lesions were excluded. Other factors can affect temperature measurements with PRF, including echo time, tissue susceptibility, electrical conductivity, and external field drift.
A limitation of this study is that not all the tumors in this series would be suitable candidates for thermal ablation in actual practice, regardless of the MR thermography image quality. For example, proximity to critical structures and the size of some of the lesions may dissuade against thermal ablation. Nevertheless, this study provides an overview of potential target lesions at different anatomic sites within the head and neck. Another issue is that only factors might determine overall image quality besides CNR and SNR, such as the possibility of patient motion.
Conclusion
Although phase contrast MR thermography image quality is generally adequate for delineating various tumors in different areas of the head and neck, there can be wide variability in the image quality. Therefore, it is important to include and evaluate the quality of the thermography sequence as part of the MRI performed for thermal ablation planning in order provide reliable temperature mapping.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported in part by the University of Chicago Comprehensive Cancer Center, the National Cancer Institute Education and Career Development program R25 Cancer Nanotechnology in Imaging and Radiotherapy (R25CA132822) and the Cancer Research Foundation.