
Abstract
Objectives:
The aim of this study is to assess the association between atrial fibrillation (AF) and sudden sensorineural hearing loss (SSNHL).
Methods:
This study was conducted by searching the longitudinal health insurance database of the Taiwan National Health Insurance Program for relevant information from January 1, 2000, to December 31, 2011. Patients with AF were matched with non-AF controls with a 1:1 strategy according to propensity scores. Multiple logistic regression analyses were performed to determine the risk of SSNHL.
Results:
In total, 14 698 patients with AF were matched with the same number of non-AF patients as controls. After propensity score matching, the use of antiplatelet or anticoagulation medications and the occurrence of SSNHL were found to have a significant difference between AF and non-AF patients. The occurrence of SSNHL was found to be higher in men, those of 45 to 74 years old, and patients with hypertension in both AF and non-AF groups. Multiple logistic regression analyses revealed that male gender, age between 45 and 74 years, hyperlipidemia, and hypertension are risk factors for SSNHL. The use of aspirin was found to reduce the rate of SSNHL (odds ratio [OR]: 0.67, 95% CI: 0.49-0.94, P = .019), but AF was not found to be a risk factor for SSNHL (OR: 0.89, 95% CI: 0.64-1.23, P = .467).
Conclusion:
The association between AF and SSNHL is not significant.
Introduction
Sudden sensorineural hearing loss (SSNHL) is an acute ear disease that requires immediate medical attention. It is defined as an idiopathic hearing loss of more than 30 dB of the ear with the problem compared to the healthy one in at least 3 consecutive tests during a 72-hour period. 1 Its annual incidence rate is 4 to 160 cases per 100 000 population. 2 In Taiwan, the incidence rate determined by a population-based study is 8.85 per 100 000 population for men and 7.79 for women with an increased tendency over age. 3 The etiologies of sudden hearing loss may include virus infections, 4 autoimmune diseases, 5 and vascular insufficiency. 6 Several observational studies have demonstrated an association between stroke and SSNH. 7,8
Atrial fibrillation (AF) is the most common cause of cardiac arrhythmia. Atrial fibrillation has a prevalence rate of 0.95% in the United States and is more common in men than in women. 9 It is the major factor contributing to cardiovascular morbidity and mortality. 10 One of the most serious complications of AF is an embolic cerebrovascular accident. A large observational study of the Framingham Heart Project reveals a 4- to 5-fold increased risk of stroke in patients with AF. 11 Furthermore, patients with permanent AF are found to have a higher risk of stroke than those with paroxysmal AF. 12
There have been reports on the association between SSNHL and vascular diseases. In a case–control study, Mosnier et al reported vascular involvement as the etiology of some cases of SSNHL. 13 In another study, Yamasoba et al found that SSNHL is associated with slow blood flow of the vertebrobasilar system. 14 Although AF has been associated with an increased risk of cerebrovascular accident, the association between AF and SSNHL is unknown. Therefore, we conducted a population-based study to determine whether there is an association between AF and SSNHL.
Patients and Methods
Data Source
The National Health Insurance (NHI) program enrolls more than 99% of the total population in Taiwan. Hospitals and clinics, which provide holistic healthcare services, submit standardized claims of health care services to obtain reimbursement through the program. The National Health Research Institutes construct and manage the National Health Insurance Research Database (NHIRD) to record the claims. National Health Insurance Research Database contains registration files and original claim data of all enrollees and is one of the largest health care databases in the world. 15,16 With a stratified multistage sampling method, a sub-database of NHIRD was created in 2000. This database is referred to as longitudinal health insurance database 2000 (LHID 2000) and contains standardized claims of one million randomly selected people, representing approximately 5% of NHI beneficiaries in 2000.
Patients for this population-based, case–control study were retrospectively selected from LHID 2000 from January 1, 2000, to December 31, 2011, based on codes of the International Classification of Diseases, Ninth Edition, Clinical Modification (ICD-9-CM). This study was approved by the institutional review board of the Taipei City Hospital (approval no. TCHIRB-10904016-E).
Study Patients
Patients with AF (ICD-9-CM code 427.31) and SSNHL (ICD-9-CM code 388.2) were investigated. AF patients were those with at least 2 outpatient visits and at least one hospitalization for unstable AF. Patients with SSNHL were those with at least one outpatient visit and one hospitalization due to sudden deafness. To reduce the likelihood of including patients with congenital heart diseases related to AF, 167 423 patients younger than 18 years were excluded. Twenty-two patients in the AF group with no recorded gender information and 91 patients with a diagnosis of SSNHL before AF were also excluded. A total of 14 711 patients with AF were identified (Figure 1). Controls included 817 753 patients without AF after exclusion of the aforementioned patients. Comorbidities such as hypertension, hyperlipidemia, and diabetes mellitus were identified from the data of more than 3 ambulatory care claims or 1 inpatient claim in a year. To reduce the confounding effects of anticoagulants or antiplatelets on the occurrence of SSNHL, patients who used these drugs for more than 28 days consecutively before the diagnosis of SSNHL were identified. Patients with a 28-day prescription for a disease were considered as having a chronic condition of such. The non-AF patients were selected by propensity scores adjusted for age, sex, and cardiovascular disease risk factors including hypertension (ICD-9-CM code: 401), hyperlipidemia (ICD-9-CM code: 272), and diabetes mellitus (ICD-9-CM code: 250). Thirteen patients with AF could not be matched with controls. Consequently, 14 698 patients with AF and 14 698 matched non-AF controls were included in this study.
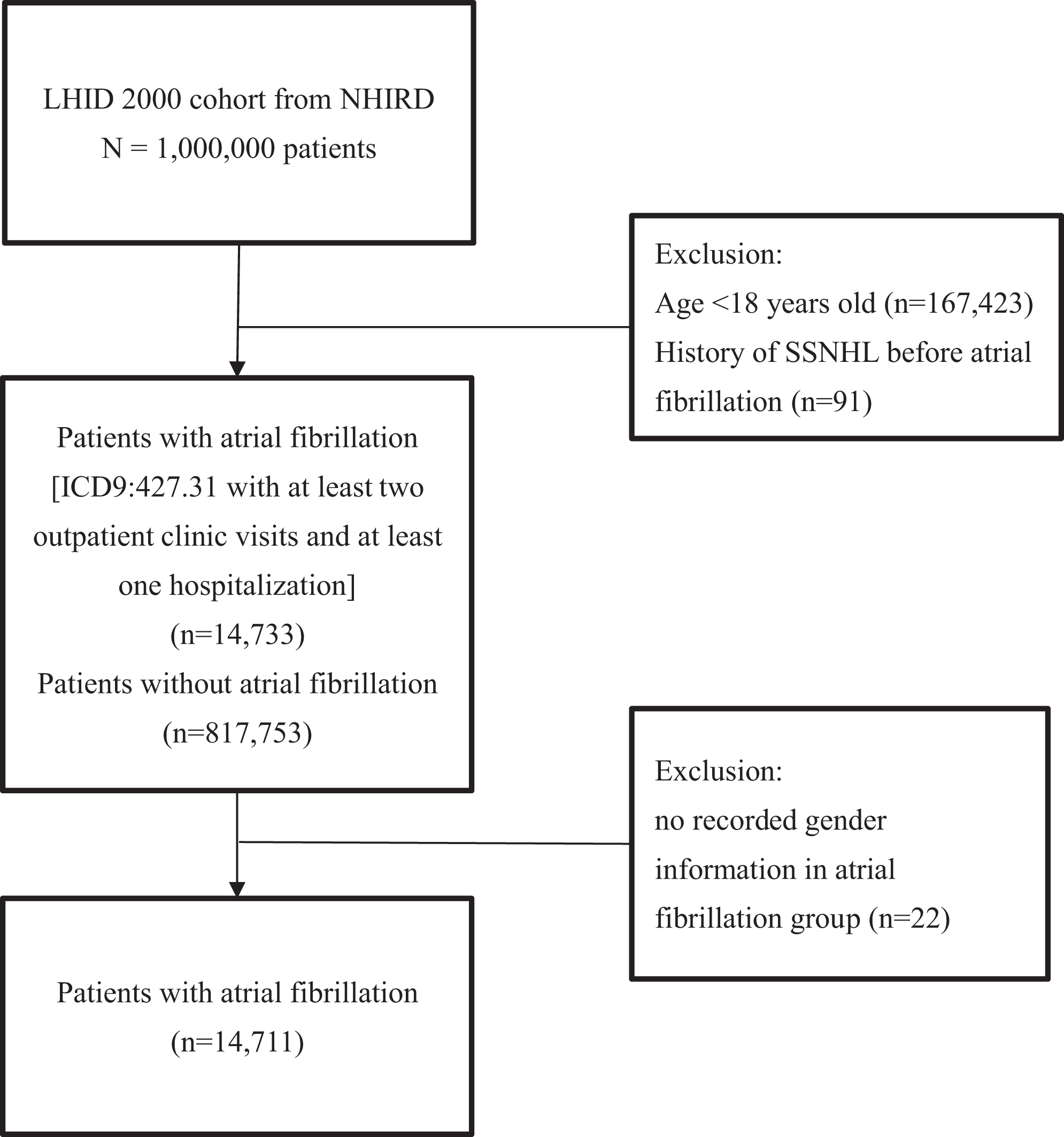
Flowchart for identification of patients with atrial fibrillation. ICD indicates International Classification of Diseases; LHID 2000, longitudinal health insurance database 2000; NHIRD, National Health Insurance Research Database; SSNHL, sudden sensorineural hearing loss.
Statistical Analysis
The SAS software (SAS System for Windows, version 8.2, SAS Institute Inc.) was used for statistical analyses. Descriptive statistics and the χ2 test for independence were used to compare the differences between patients with and without AF. The following parameters were compared: gender, age (<45 years old, 45-54 years old, 55-64 years old, 65-74 years old, >75 years old), comorbidity (hypertension, diabetes, and hyperlipidemia), and anticoagulants and antiplatelets (aspirin, clopidogrel, and warfarin). The 2-sample t test was also used to compare the aforementioned parameters. The Fisher exact test was used to determine whether there were nonrandom associations between those with and without an anticoagulation medication. Multiple logistic regression was used to assess the association between AF and SSNHL. A P value ≤.05 is considered as significant.
Results
After the 1:1 propensity score matching, only the use of antiplatelet or anticoagulation medications and the occurrence of SSNHL had a significant difference between AF and non-AF patients (aspirin: 79.09% vs 47.17%, clopidogrel: 23.57% vs 9.55%, warfarin: 26.54% vs 2.71%, occurrence of SSNHL: 0.54% vs 0.77%; Tables 1 and 2). In the AF group, the occurrence of SSNHL was higher in male patients and in those who were between 45 and 74 years old or those who had hypertension. In the non-AF control group, in addition to these factors, patients with hyperlipidemia and diabetes mellitus were found to have a higher rate of SSNHL. None of the medications including aspirin, clopidogrel, and warfarin affected the rate of SSNHL in both AF and non-AF groups (Tables 3 and 4). However, the use of aspirin was found to reduce the rate of SSNHL after logistic regression (odds ratio [OR]: 0.67, 95% CI: 0.49-0.94, P = .019). Results of logistic regression analyses also confirmed that male gender, age between 45 and 74 years, hyperlipidemia, and hypertension were significant risk factors for SSNHL, but AF was not found to be a risk factor for SSNHL (OR: 0.89, 95% CI: 0.64-1.23, P = .467; Table 5).
Baseline Characteristics of Patients Before Propensity Score Matching.
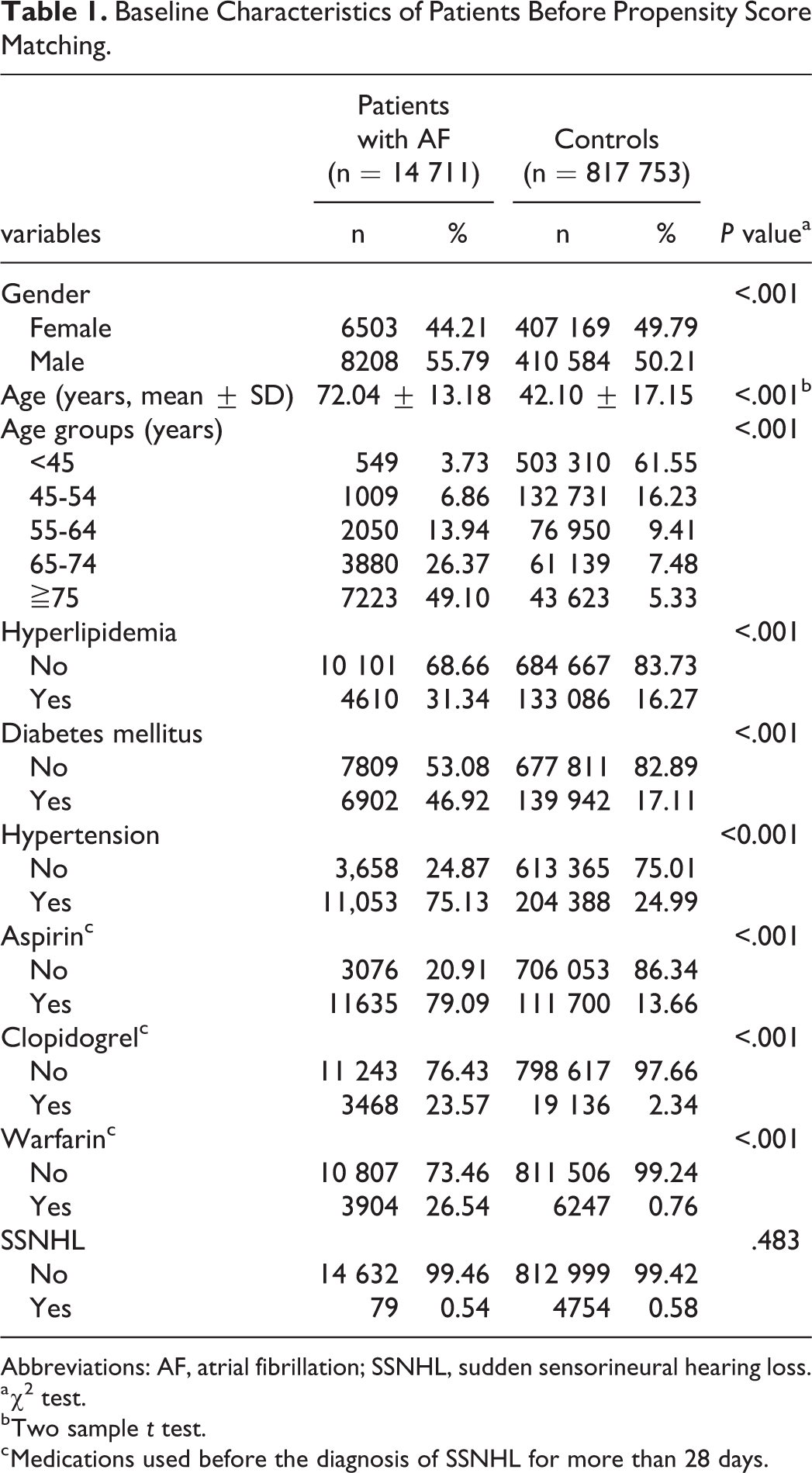
Abbreviations: AF, atrial fibrillation; SSNHL, sudden sensorineural hearing loss.
a χ2 test.
b Two sample t test.
c Medications used before the diagnosis of SSNHL for more than 28 days.
Baseline Characteristics of Patients After Propensity Score Matching.
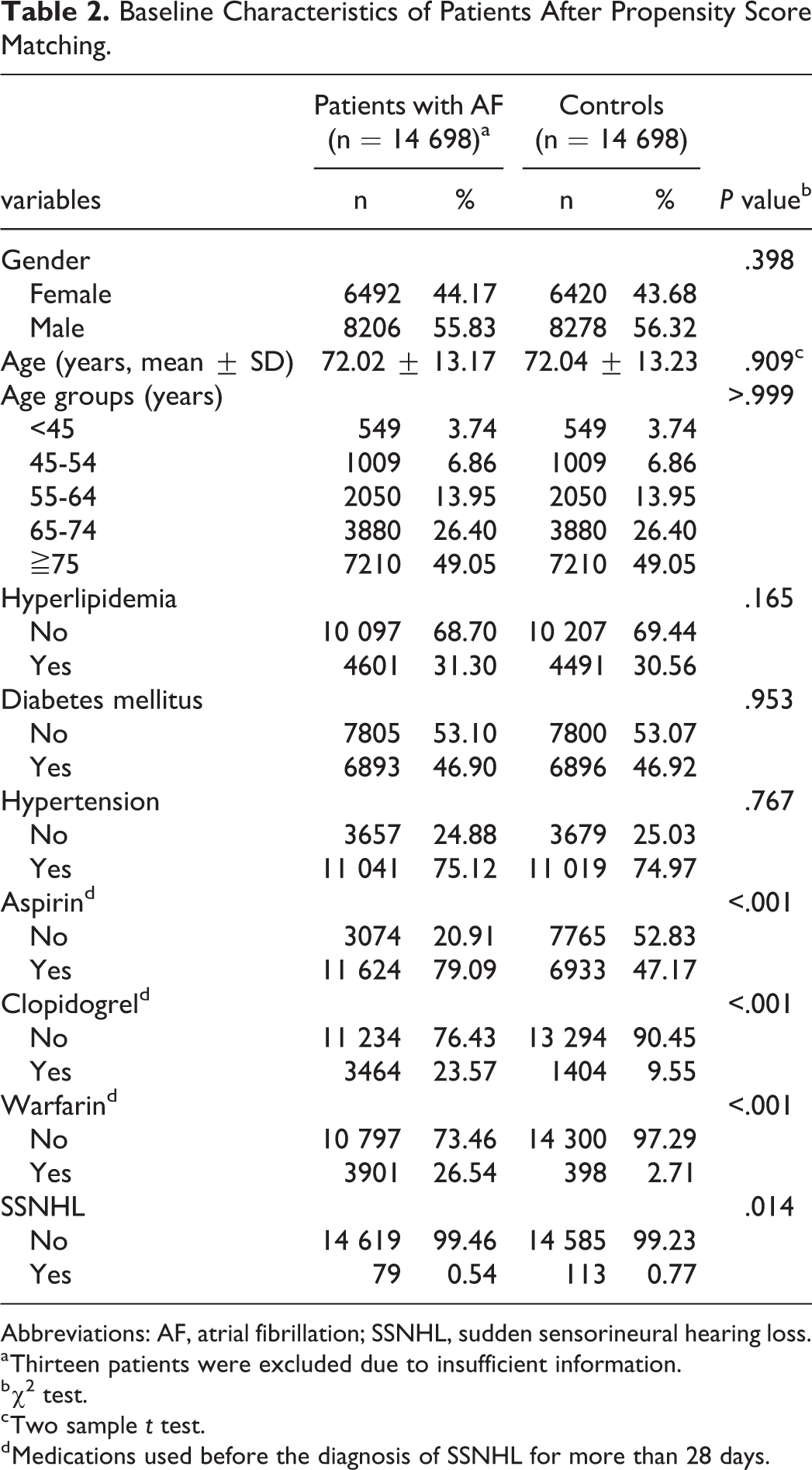
Abbreviations: AF, atrial fibrillation; SSNHL, sudden sensorineural hearing loss.
a Thirteen patients were excluded due to insufficient information.
b χ2 test.
c Two sample t test.
d Medications used before the diagnosis of SSNHL for more than 28 days.
Characteristics of AF Patients With and Without SSNHL After PSa Matching.
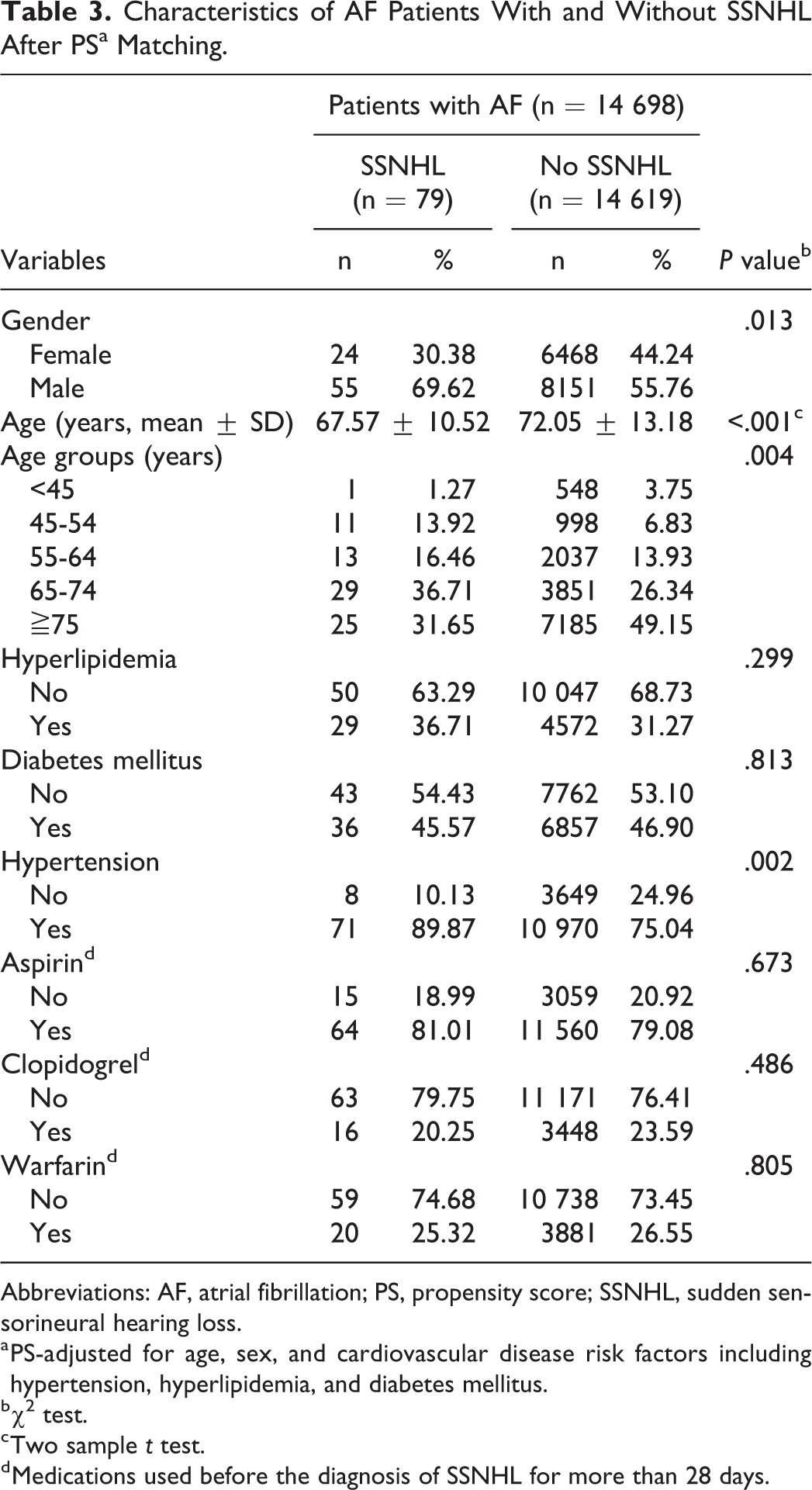
Abbreviations: AF, atrial fibrillation; PS, propensity score; SSNHL, sudden sensorineural hearing loss.
a PS-adjusted for age, sex, and cardiovascular disease risk factors including hypertension, hyperlipidemia, and diabetes mellitus.
b χ2 test.
c Two sample t test.
d Medications used before the diagnosis of SSNHL for more than 28 days.
Characteristics of Non-AF Patients With and Without SSNHL After PSa Matching.
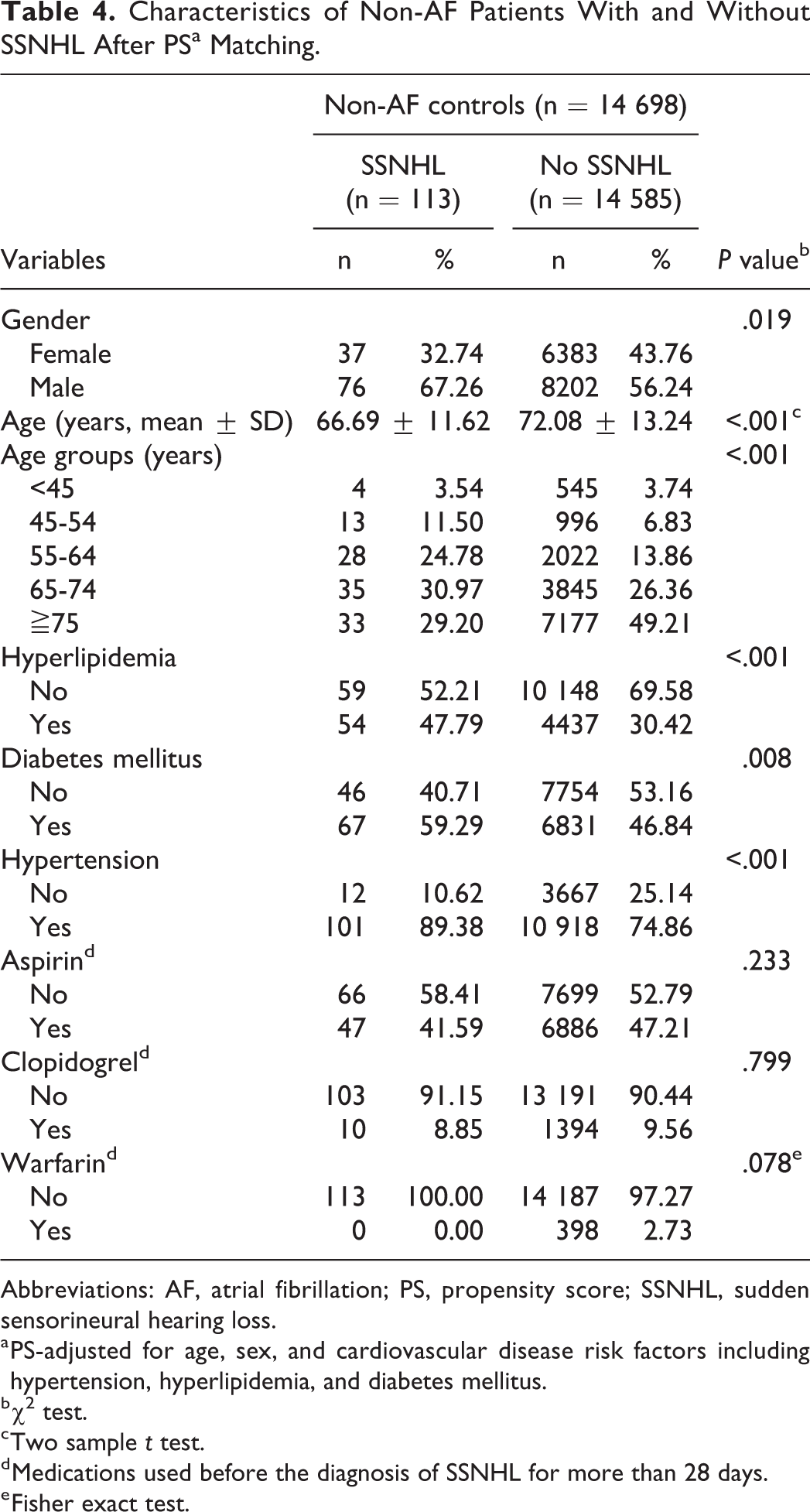
Abbreviations: AF, atrial fibrillation; PS, propensity score; SSNHL, sudden sensorineural hearing loss.
a PS-adjusted for age, sex, and cardiovascular disease risk factors including hypertension, hyperlipidemia, and diabetes mellitus.
b χ2 test.
c Two sample t test.
d Medications used before the diagnosis of SSNHL for more than 28 days.
e Fisher exact test.
Multiple Logistic Regression of Risk Factors for SSNHL.
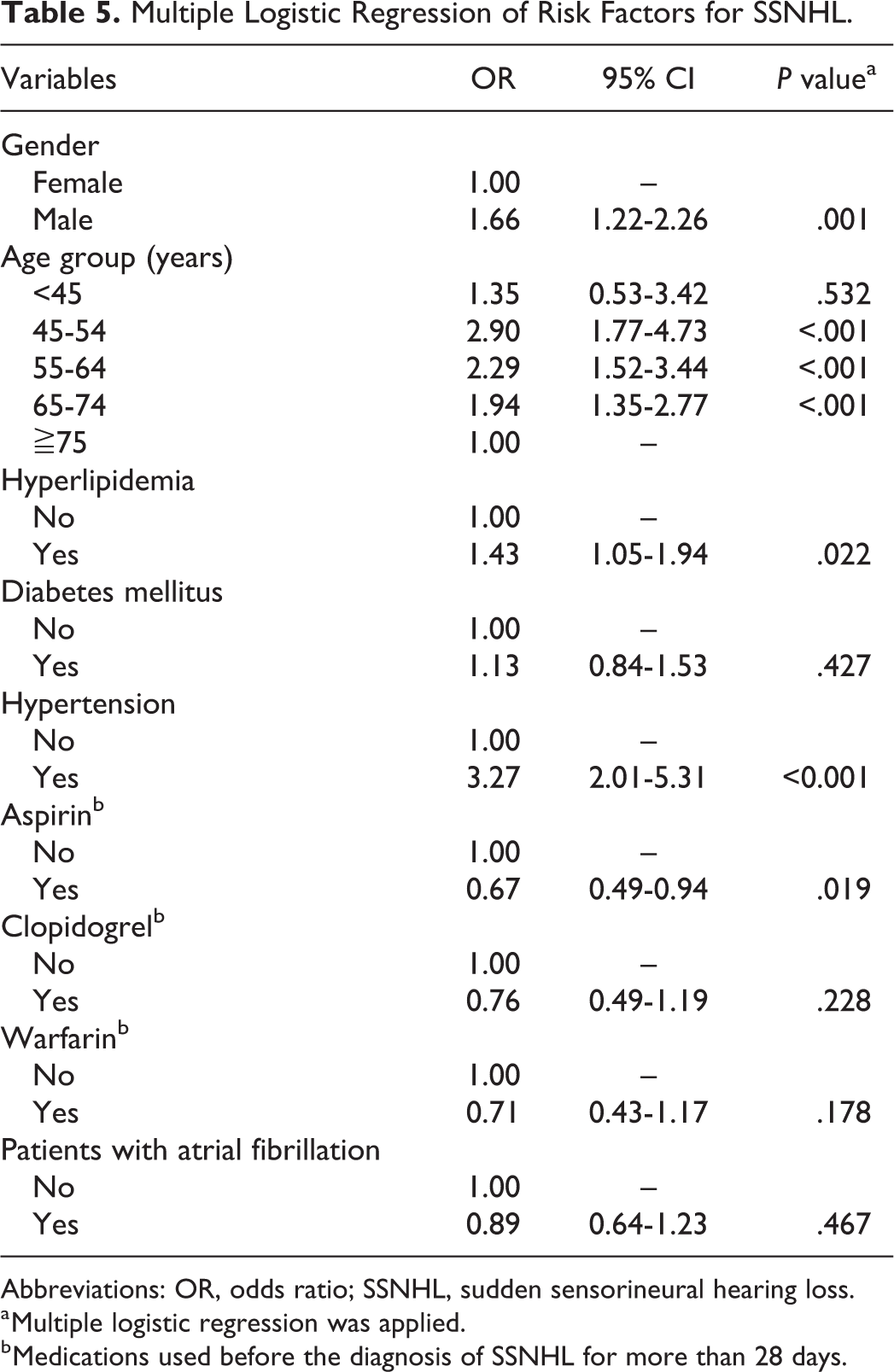
Abbreviations: OR, odds ratio; SSNHL, sudden sensorineural hearing loss.
a Multiple logistic regression was applied.
b Medications used before the diagnosis of SSNHL for more than 28 days.
Discussion
In this study, the rate of SSNHL was found to be higher in patients with hyperlipidemia or hypertension, and AF was not found to be a risk factor for SSNHL. As antiplatelet or anticoagulation medications such as aspirin, clopidogrel, and warfarin are commonly used by AF patients, logistic regression analyses were performed to assess their effects on SSNHL. After adjusting for comorbidities, aspirin was found to reduce the risk of SSNHL (Table 5).
Results of several previous case studies suggest that an embolic event is a cause of SSNHL. 17,18 Furthermore, some symptoms of sudden onset and most cases of unilateral SSNHL are similar to those of ischemic stroke. 19 Atrial fibrillation has been shown to increase the risk of stroke by 4- to 5-fold due to embolic events. 11 In this study, AF was not found to be a risk factor for SSNHL. Therefore, our results do not support the hypothesis that an embolic event is a cause of SSNHL.
Hyperlipidemia, diabetes mellitus, hypertension, and smoking are well recognized as contributing factors to atherosclerosis. 20 Rajati et al found that SSNHL patients have increased thickness of the intima media of carotid arteries compared to non-SSNHL patients and postulated that subclinical atherosclerosis leads to SSNHL. 21 In the present study, hyperlipidemia and hypertension were found to increase the risk of SSNHL as we have previously observed, 6 and aspirin was found to reduce the risk of SSNHL. These observations support the hypothesis that atherosclerosis is associated with SSNHL. As one-third of AF patients have a concomitant atherosclerotic coronary artery disease 22 and take aspirin routinely to prevent vascular complications, it is conceivable that AF patients have a lower incidence of SSNHL. However, a meta-analysis study showed that aspirin increases the mortality rate in patients with nonvalvular AF. 23 Further randomized control studies are warranted to confirm the effect of aspirin on SSNHL.
Another significant finding in our study is that patients in the age range of 45 to 74 have a higher incidence of SSNHL (Table 5). The peak age range is 45 to 54, which is 5 years younger than that of the study of a Japanese population performed in 1972 and 1987 24 and 10 years younger than that of the study of a Taiwanese population reported in 2002. 3 A busy lifestyle is considered as a cause of increased incidence of SSNHL in younger individuals. 25 The difference in the peak age of incidence between ours and the other study from Taiwan may be due to the highly selected study population in our study.
The strengths of our study are that the diagnoses of AF and SSNHL were conducted by physicians accredited by official authorities and that the propensity score matching was adjusted for several risk variables to minimize the effects of confounding factors. Also, our study was a population-based study with a large sample size to ensure that the statistical power was sufficient. Limitations of this study are as follows. As it is an observational study of a highly selected population, the results may not be generalized. In addition, the claim information in the database is mainly for reimbursement, not for research; therefore, some important epidemiologic data, such as physical activities and history of smoking, are missing. Because this study was initially designed to assess the association between AF and SSNHL, the effect of medications on SSNHL was not the primary end point, and their dose–response effect was not thoroughly investigated.
Conclusions
Patients with AF were not found to have a higher rate of SSNHL than non-AF patients. Factors including male gender, age between 45 and 74 years, hyperlipidemia, and hypertension were associated with SSNHL. In addition, the use of aspirin was found to be associated with a reduced risk of SSNHL.
Supplemental Material
Supplemental Material, sj-pdf-1-ear-10.1177_01455613211042566 - Atrial Fibrillation Is Not Associated With Sudden Sensorineural Hearing Loss
Supplemental Material, sj-pdf-1-ear-10.1177_01455613211042566 for Atrial Fibrillation Is Not Associated With Sudden Sensorineural Hearing Loss by Trong-Zong Chen, Bi-Hua Cheng, Hsiao-Yun Hu, Chia-Chi Chang, Shu-Yi Lin and Hung-Meng Huang in Ear, Nose & Throat Journal
Footnotes
Authors’ Note
This study was approved by the Institutional Review Board of the Taipei City Hospital (approval no. TCHIRB-10904016-E).
Acknowledgements
The authors thank the staff of the Center for Public Health, Department of Education and Research, Taipei City Hospital, Taiwan for their valuable contributions in data management and statistical analysis.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.