
Abstract
Objective:
A proportion of patients with coronavirus disease (COVID) and severe respiratory manifestations of disease will require admission to intensive care for intubation and ventilation. When anticipating prolonged ventilation, the patient may proceed to surgical tracheostomy to afford safe respiratory wean. As surgical tracheostomy is an aerosol-generating procedure, it poses a high risk of viral transmission and ultimately may prompt anxiety and caution in participating staff members. We aimed to mitigate these risks by providing staff with appropriate training and experience, to improve their confidence as well as practical ability.
Methods:
We developed a multidisciplinary simulation training experience and checklist in order to optimize team performance during the high-stakes procedure. We evaluated staff confidence before and after the training with questionnaires.
Results:
Post-simulation, surgeons were more confident with donning the high level personal protective equipment, and nurses were more confident in performing their role.
Conclusions:
Simulation allows the multidisciplinary team an opportunity to practice high-risk procedures and prompts the team to assess staff knowledge base, troubleshoot queries, and teach roles and responsibilities in a safe environment. In the context of COVID-19, simulation encourages staff sense of preparedness and protection for true participation during a high-risk procedure.
Introduction
Severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) was identified in late 2019, originating from Wuhan City, China. SARS-CoV-2 has led to a global pandemic with coronavirus disease 2019 (COVID-19) rapidly and persistently affecting global health care. 1 The novel coronavirus has a high rate of transmissibility, with many of its’ carriers asymptomatic. The symptom profile of SARS-CoV-2 ranges from anosmia, mild upper respiratory tract infection to severe acute respiratory distress syndrome. 2 Of those patients requiring hospitalization due to respiratory deterioration, around 3% to 17% 3 will require mechanical ventilation or invasive organ support in critical care. Globally, there has been, throughout this pandemic, a very marked increased need for intensive care unit (ICU) capacity 4 and in some hospitals, this has been overwhelming. 5 In patients too weak to be extubated or in those who have failed trials of extubation, tracheostomy affords a safe way to manage these patients and allow them to step down from ICU freeing up crucial capacity. Additionally, to the normal accepted benefits of tracheostomy, 3 patients with SARS-CoV-2 have shown favorable outcomes including shorter length of ICU stay and reduction in overall time ventilated. 6 In one multicenter study, early tracheostomy in ventilated patients with COVID-19 was associated with shorter length of ventilated days and shorter stay on the ICU. 7 Other single-center studies support that early percutaneous tracheostomy in ventilated patients with COVID-19 facilitated quicker weaning of ventilation and a lower mortality rate. 8,9 However, surgical tracheostomy is recognized as a significant aerosol-generating procedure (AGP) and there is a high risk of transmission to participating staff, as the virus is concentrated in the sputum and upper airway secretions. 10
In the first wave at our institution (March-May 2020), 263 patients required ICU care and ultimately 62 needed tracheostomies. Although our unit was not overwhelmed, there was a pressing need during this first crisis to develop an efficient and safe tracheostomy pathway to promptly discharge patients from ICU. We developed a multidisplinary simulation training program, described below, to achieve these aims. Multidisciplinary implies an interprofessional approach to training, including participants from different medical specialties together with nurses, health care assistants, and operating department practitioners (ODPs). Subsequently, this training and care pathway has been utilized in the second wave in the United Kingdom between December 2020 and March 2021.
Simulation Training
Simulation training provides a safe environment for participants to practice clinical application of practical skills, effective communication, and respond to adverse or unexpected events within a high-fidelity training environment. This emersion facilitates rehearsal of high-risk procedures, allowing participants to exhibit their concrete knowledge and adapt to change alongside their peers. This experience considers the sociocultural influence of learning 11 and the value of building on concrete experience with practice and the opportunity to scaffold on existing knowledge. 12,13
As intubated patients with COVID-19 may be challenging to ventilate with a propensity to deteriorate quickly, it was paramount that the tracheostomy procedure was streamlined. A fast and smooth-running procedure optimizes safety for patients and staff. Simulation was considered for this procedure as it allows the identification of high-risk aspects and promotes discussion of how the team can appropriately compensate to maintain a safe environment. Simulation of the surgical procedure also allows staff to practice using high-level personal protective equipment (PPE). The identification of risk and the team’s compensatory actions was crucial when considering the high staff anxiety regarding the AGP risk of surgical tracheostomy.
Aims of Simulation Training for Surgical Tracheostomy
Simulation training was developed to allow staff to feel more prepared to participate in COVID tracheostomy. Familiarization with the surgical procedure and good knowledge of fellow staff roles should ensure smoother running of the theatre. Training with the high grade PPE required, including the powered air-purifying respirator (PAPR), aimed to alleviate staff anxiety in anticipation of the high-risk exposure. The physical barrier of high-level PPE can hinder effective communication in the theatre environment. Simulation including all members of the multidisciplinary team (MDT), specifically surgeons, anesthesiologists, health care assistants, ODPs, and nurses allowed for the development of optimal communication. Furthermore, an iterative approach was taken leading to the identification of the sufficient amount of equipment and staff required to perform the task safely and efficiently.
Materials and Methods
Development of the Simulation
Development of the simulation included pre-operative, intra-operative, and post-operative events. Chief among the preoperative considerations was to firstly establish patient suitability for tracheostomy. Patient factors considered prior to tracheostomy included clear evidence of patient improvement. These acceptable parameters were established through MDT consultant-led discussions between anesthetics, critical care, and otolaryngology. Parameters for patient improvement include reducing ventilation pressures and supplemental oxygen requirement (PEEP <10 H2O and FiO2 <0.4). The patient should no longer require proning as tracheostomy would limit the safety and practicality of this maneuver. 14 The patient should be hemodynamically stable with minimal vasopressor requirement. 15 Referral of the patient should fall within the optimum 10 to 21 days post-intubation. More recent evidence-based practice suggests that good patient outcomes are achieved by providing a tracheostomy at 8 to 14 days post-intubation. 6 Meta-analysis suggests that early tracheostomy (within 7 days of intubation) is associated with lower rates of ventilator-associated pneumonia and shorter duration of mechanical ventilation and stay on ICU. 16 The benefit of good patient outcomes should be balanced with risk of viral transmission to staff participants; patient viral load should be significantly lower 7 days post-infection. 17
Preoperative staff preparation first addressed familiarity with the tracheostomy procedure. An open floor to questions allowed discussion of the surgical procedure and the role of all theatre staff. A thorough knowledge of staff roles and of the surgical procedure meant greater preparedness for the simulation and true clinical scenario. Good knowledge of roles and procedure would anticipate fewer questions during the live simulation: this is important considering the communication barriers posed when wearing PAPR. Effective interdisciplinary communication during airway procedures for patients with COVID-19 has been recognized as important in reducing virus aerosolization. 18
Within our department, the set standard was for PAPR to be used by all participants during surgical tracheostomy. High level PPE is recognized as essential in airway associated AGPs for patients with COVID-19. 18 As this type of PPE is seldom used, it was considered important to increase all staff familiarity with safe donning and doffing. Prior to live simulations, staff were supervised donning and doffing with PAPR; supervisors were able to troubleshoot queries and correct technique. Figure 1 illustrates staff in full PAPR suits and Figure 2 illustrates the members of the MDT in PAPR and surgical gowns.

Surgeons in powered air-purifying respirator (PAPR) during simulation training.

Multidisciplinary team in powered air-purifying respirator (PAPR) and surgical gowns during simulation training.
As the theatre has a strict policy of no entry or exit intra-operatively, it was imperative to establish an exhaustive list of equipment for use throughout the procedure. This should include drugs, surgical, and anesthetic equipment. A comprehensive checklist of equipment was developed with opinion from both senior surgeons and anesthesiologists.
Certain steps of the surgical tracheostomy pose very high aerosol generating risk. Adaptations to the typical surgical tracheostomy procedure should account for this in patients ventilated secondary to SARS-CoV-2 pneumonitis.
15
Such adaptations included: Minimal use of diathermy with preferred use of cold instruments. Additional use of muscle relaxant. Prior to making the tracheal window, the endotracheal tube (ETT) was further advanced with the cuff inflated. The cuff was then hyperinflated below the planned tracheal window. Ventilation was stopped. The thorax was allowed to passively decompress for 10 seconds, then the circuit disconnected. The surgeon made the tracheal window at the smallest diameter they were confident to do so. After the tracheal window was made, the anesthesiologist deflated and withdraw the ETT under direct vision of the surgeon until the cuff was just above the tracheal window. The ETT remained in the proximal trachea until the tracheostomy tube was sited, tracheostomy cuff inflated, and the ventilatory circuit connected to the tracheostomy. Given the anticipated challenging airway in SARS-CoV-2 patient cohort, this operating procedure ensured that the ETT could be rapidly repositioned below the tracheal window if necessary. Timeliness during this particularly high aerosol generating step of surgery was emphasized to the MDT.
18
ETT removal was considered an AGP. The tube was removed rapidly and disposed into a bag which was sealed. Consultant surgeon led the operation. Anesthesiologist. Tracheostomy sutured in situ.
Pre-simulation discussion and teaching highlighted those aspects of the procedure that have high AGP risk. This ensured all theatre participants were aware of the high-risk stages and the imperative to work quickly and safely at these points.
Post-operatively, the theatre maintained a strict no entry or exit policy for 20 minutes (in accordance with local Infection Control advice and the specific air changes per minute in the theatre suite) after which the patient was transferred to intensive care by two senior anesthesiologists. Staff would then safely doff PAPR and shower on site. The theatre environment was deep cleaned between each case. Aspects of post-tracheostomy care were altered to account for staff risk and airway safety. These included delaying the first postoperative tracheostomy tube change until day 7 and regular checks for cuff leak.
Considering the complexity of the patients and risk to staff involved in the procedure, the use of formal protocol for tracheostomy in patients with COVID-19 has been used internationally. 19 These have often focused on determining appropriate timing, contraindications, PPE, surgical technique, and postoperative management. 19 A checklist of the preoperative considerations and intraoperative steps is detailed in Figures 3 and 4.
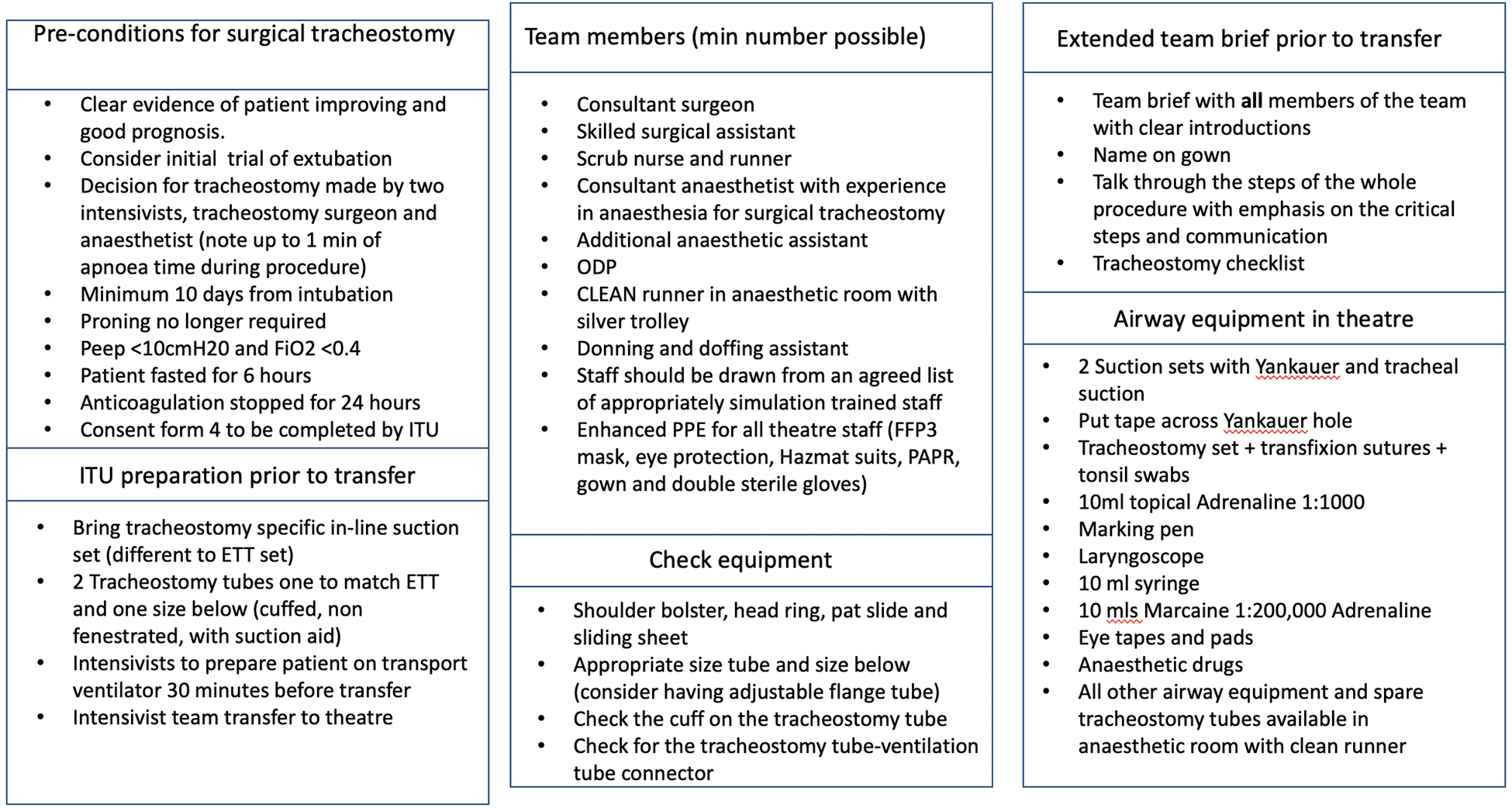
Preoperative checklist.
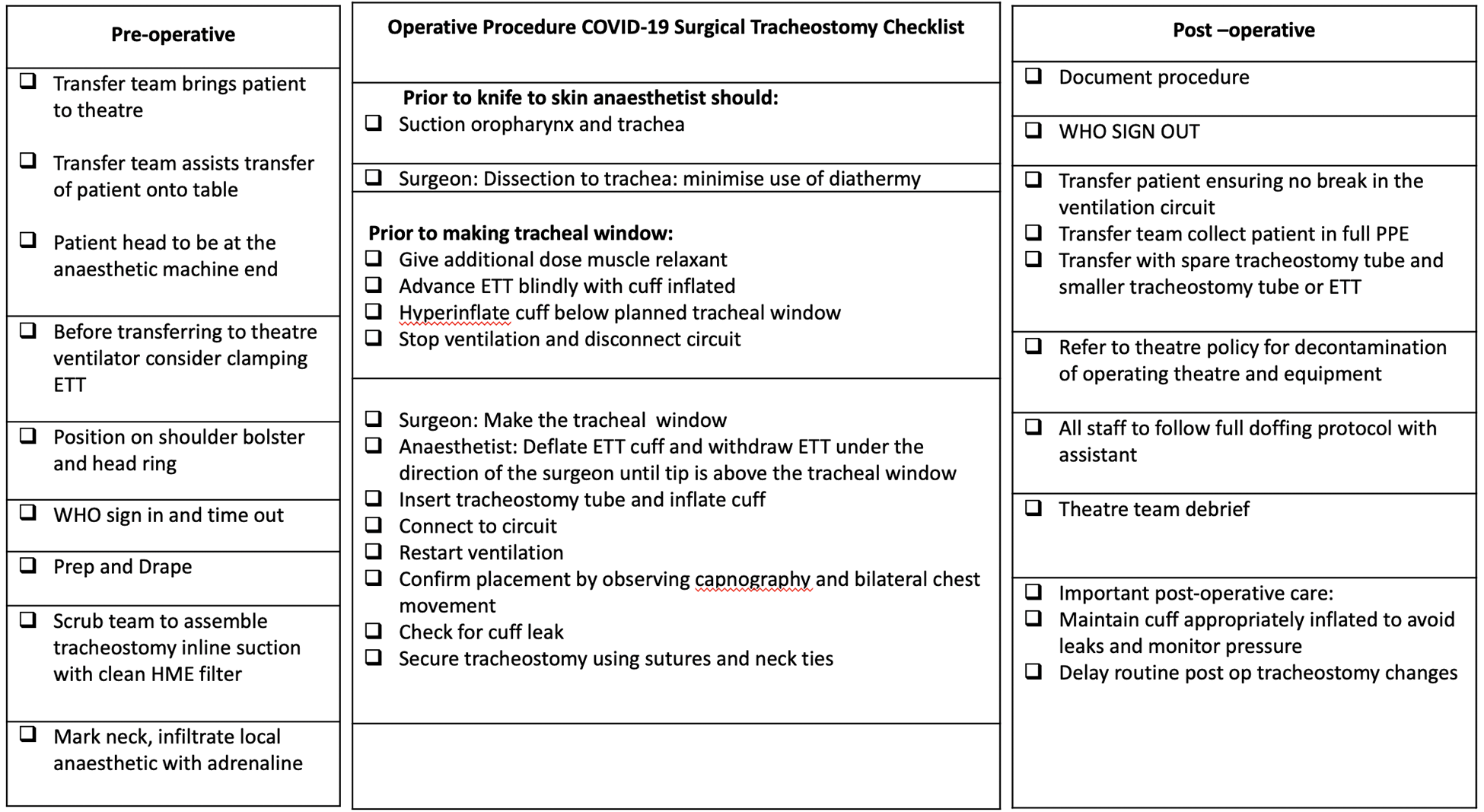
Theatre preparation and intraoperative checklist.
Post-simulation Review
Comprehensive feedback in the form of questionnaire was provided to all disciplines of the theatre team, including ODPs, nurses, surgeons, and anesthesiologists. Feedback focused on staff familiarity and confidence with the surgical procedure alongside their confidence with donning and doffing of PAPR. More open questions examining the usefulness of the simulation allowed for thematic analysis of staff opinion and preparedness for SARS-CoV-2 surgical tracheostomy.
Questionnaire Fields
Prior to simulation training
Prior knowledge and experience with indications for surgical tracheostomy, surgical equipment, and steps required for tracheostomy; steps of anesthesia and patient ventilation intraoperatively; and experience with donning and doffing.
Post-simulation training
Knowledge base of COVID-related risks of AGPs, specific examples of AGPs intraoperatively, and rationale for PPE and for PAPR during surgical tracheostomy.
Knowledge base and experience of appropriately fitted FFP3 mask, donning, and doffing procedure.
Confidence with:
preparedness for carrying out one’s own role safely during surgical tracheostomy,
protection against AGPs and SARS-CoV-2 during the surgical procedure,
the role of individual staff during the surgical procedure, including surgeon, anesthesiologist, scrub nurse, ODPs, health care assistant/runner,
participating as a member of the MDT during surgical tracheostomy,
open question to identify the benefits of the simulation training,
open question asking if participant feels more confident to fulfil their role during surgical tracheostomy, and
question to ask if the staff member would recommend the simulation training to their colleagues.
Results and Analysis
During the first wave, 94 members of staff participated in the simulation training. Twenty-one surgeons were trained, 19 male and 2 female; 14 consultant surgeons; and 7 senior registrars (ST5+). Surgeons have been stratified according to previous experience of surgical tracheostomy: 10 to 30, 30 to 50, 50 plus (expert).
Twelve anesthesiologists participated, 7 male and 5 female. Thirteen ODPs, 4 male and 9 female. Thirty-seven nurses, who would take the role of either scrub nurse or “runner,” 25 female and 12 male. Eleven health care assistants, who would typically take the role of “runner,” of which 7 were male and 4 female.
Questionnaires were circulated to 34 members of staff who participated in the simulation training: surgeons, 11 anesthesiologists, 6 nurses, 11 ODPs, 3 and health care assistants. 3 In order to compare pre-simulation and post-simulation subjective confidence, we performed statistical analyses for responses to particular aspects of the questionnaire.
Donning and doffing of PAPR for surgical tracheostomy, questions compared: Pre-simulation: “Experience with donning and doffing” Post-simulation: “Donning procedure,” “Doffing procedure” Possible response: no knowledge, basic knowledge, good knowledge, expert
Analysis of surgeon participant responses to the questionnaire showed a significant improvement in donning and doffing after the simulation training, Mann Whitney test; P = .03; P < .05. Subset analysis between surgical grade, using stratification according to previous number of tracheostomies completed, showed no statistical difference to suggest improved confidence.
Confidence in specific role for surgical tracheostomy, questions compared:
Surgeon:
Pre-simulation: “Surgical steps for tracheostomy”
Post-simulation: “The role of the surgeon during COVID surgical tracheostomy”
Anesthesiologist:
Pre-simulation: “Steps of anesthesia intraoperatively for surgical tracheostomy”
Post-simulation: “The role of the anesthesiologist during COVID surgical tracheostomy”
Nurse:
Pre-simulation: “Surgical equipment required for tracheostomy, steps of anesthesia intraoperatively for surgical tracheostomy, ventilation intraoperatively during surgical tracheostomy”
Post-simulation: “The role of the scrub nurse during COVID surgical tracheostomy”
ODP:
Pre-simulation: “Surgical equipment required for tracheostomy, steps of anesthesia intraoperatively for surgical tracheostomy, ventilation intraoperatively during surgical tracheostomy”
Post-simulation: “The role of the ODP during COVID surgical tracheostomy”
Health care assistant/runner:
Pre-simulation: “Surgical equipment required for tracheostomy, steps of anesthesia intraoperatively for surgical tracheostomy, ventilation intraoperatively during surgical tracheostomy”
Post-simulation: “The role of the runner during surgical tracheostomy”
Possible response: no confidence, little confidence, good confidence, high confidence
Analysis of nursing participant responses to the questionnaire showed a statistically significant increase in confidence for their role in the surgery after completing the simulation (Mann-Whitney test; P = .389; P < .05). Health care assistants showed a decrease in subjective confidence (Mann Whitney test; P = .0389; P < .05). All other groups of staff showed no significant difference in confidence to participate in their specified role following the simulation training.
Overall confidence in the procedure and participating as part of the MDT with COVID surgical tracheostomy showed no statistically significant difference following the simulation. Responses were analyzed using the Kruskal-Wallis test with a post-test Dunn multiple comparison test. Participants across all roles reported on average “good confidence” after the simulation.
Open questions prompted staff to express subjective benefits of the simulation training. Popular positive responses included: Increased feeling of preparedness for the surgical procedure, Increased familiarity with donning and doffing, Increased confidence and team working ability, Greater familiarization with fellow staff roles, Better understanding of points with high AGP risk, and Reduction in staff panic regarding the procedure.
Final subjective questions asking whether staff felt more prepared to participate in surgical tracheostomy and if they would recommend the training were answered “yes” 100% and 97%, respectively.
Discussion
Simulation as a method of teaching can range from low fidelity with simple bench side models to high fidelity immersive training. This may include virtual reality technology, or patient simulators set in a high-fidelity clinical environment such as the operating theatre. High fidelity simulation thus allows training of the clinician in technical skill, communication, and interdisciplinary teamwork in a safe environment with no risk to patient safety. Surgical training requires a varied skill set, including practical craftsmanship and nontechnical skills (NTS) of communication and crisis management. 20 Considering the multiple domains of skill demanded of a surgeon, simulation can be applied to their training to develop both technical and soft skills.
The traditional apprenticeship model of surgical training is becoming increasingly challenging to sustain in the context of reduced operating hours and training structured by multiple rotational placements. 21 Further exacerbating these issues is the current pandemic: surgeons have minimal elective operative time and thus the opportunity for training is heavily limited.
Subsequently, simulation training is being recruited more frequently to allow trainee surgeons to consistently develop their technical skills. Analysis of the reliability and validity of simulation for surgical training has identified that it encourages the development of “soft” skills that usually only come with time and experience in theatre. 21 The utility of simulation for both junior and senior surgeons for training of communication skills and crisis management is becoming increasingly accepted. 22
Sutherland’s meta-analysis, examining the reliability and benefit of simulation for surgical training, indicated that simulation showed limited benefit for the development of technical skill. 23 Rather, Sutherland suggested that simulation showed clear benefit for the development of good communication between surgeons and other staff disciplines in the theatre environment. 24 Meling and Meling identified that following surgical simulation, the participant surgeons had shorter operative time. 25
A review of multidisciplinary simulation has focused on crisis management in operative theatres and intensive care. 26 This review suggested MDT simulation training optimizes aspects of communication, teamwork, and leadership in simulated crisis scenarios, however there was limited observation of outcomes in a true clinical environment. Further review recognizes multidisciplinary simulation is effective in the development of NTS, specifically communication, teamwork, leadership, and situation awareness. 27 Recommendation was made to include the entire multidisciplinary operating room team in future simulation training.
Simulation training for percutaneous tracheostomy in ventilated patients with COVID-19 has been facilitated in 2020. 28 This team recognized the high-risk nature of this procedure and developed a training module for surgeons to introduce the method and relevant PPE with a high-fidelity patient model. The training highlighted the challenging aspects of the procedure, allowing participants to rehearse in a simulated high-pressure environment and prompted a new surgical checklist.
Our team utilized questionnaires to analyze staff confidence following the simulation training. The use of questionnaires to establish staff confidence after interprofessional simulation training was a novel concept established by our team. Although subjective responses indicated a positive experience with greater confidence post-simulation, there was limited statistically significant increase in confidence across staff. Following the simulation, on average all staff reported “good confidence” for participating in the surgical procedure.
Key Findings
Surgeons showed a statistically significant improvement in confidence with donning and doffing after the simulation.
Nurses showed a statistically significant increase in confidence for participating in their role after the simulation. Health care assistance showed a decrease in confidence for participating in their own role following the simulation.
All participants on average had “good confidence” for overall confidence for participating in the surgical procedure after the simulation.
No other staff discipline had a significant change in confidence in all domains of the questionnaires. We acknowledge that the simulation was developed by senior surgeons who are most familiar with constructing training and assessment for fellow doctors. Perhaps we should have anticipated that simulation training is relatively familiar to surgeons compared to other staff participants. A suggestion we made to widen the impact of the simulation training and to improve staff confidence across all disciplines was to repeat the interprofessional simulation training for the same staff cohort. Prior to the repeat sessions, we propose informal troubleshooting sessions. At each troubleshooting session, a senior member of each staff discipline should be present to respond to questions with good context and experience. Further questionnaires after the repeated simulation training would be offered to establish staff confidence.
Exposure to the simulation may have introduced previously unknown scenarios and processes, particularly for staff such as health care assistants, many of whom were redeployed from their home specialties to theatres during the first surge. We recommend using a multidisciplinary approach to future simulation development, ideally recruiting staff from all disciplines to teach during the training. This would allow for a more inclusive training, which may draw upon role-specific experience in order to optimize a multidisciplinary teaching environment.
Our trust participated in the national audit analyzing the outcomes of patients post-COVID tracheostomy. 15 Review of patient outcomes at our trust during the first peak of infections (March-May 2020) was positive. At our trust, 8% (5 patients) died following tracheostomy and 91% (57 patients) were still alive at the point of the survey, in comparison to the national average of 12% and 88%, respectively; 92% were weaned off mechanical ventilation successfully (52% national average). Zero patients at our trust had tracheostomy cause of death following the procedure (3% national average). Staff infection rates at our trust within 14 days following surgical tracheostomy remained at zero in both the first and second peak (December 2020-March 2021).
Following the implementation of simulation training for COVID tracheostomy, we have been able to repeat this teaching during the second peak of the pandemic. The necessity of repeat facilitation and refresher courses has been essential considering many staff have changed hospital trusts or departments since the first peak. This training has allowed staff to familiarize themselves with their role, other members of the MDT, and the interdisciplinary human factors to consider in this high-risk procedure. With an established simulation pathway in place, throughout the second wave, staff have been trained rapidly, with the supplementary accepted checklist to aid staff in practice and real life. Together this has aided the smooth reintroduction of a tracheostomy referral pathway for surgical teams and critical care colleagues: appropriate patients can be referred without delay. Early appropriate tracheostomy allows weaning of mechanical ventilation and ultimately accelerating step down from high dependency areas, thus relieving some of the heavy pressure currently on ICUs.
Although the pandemic proceeds, we will continue to provide refresher courses and simulation training for staff participating in COVID tracheostomy. As described, feedback indicates that staff appreciate the opportunity to simulate surgical practice as an MDT. Considering the high-stake surgical procedures involved with many ENT emergencies, we plan to develop further simulation training opportunities. Improving the interdisciplinary knowledge of staff roles and optimizing communication in the theatre environment are essential to maintain patient safety.
Conclusions
Simulation offers a high-fidelity training environment for multiple clinical disciplines and scenarios. Regarding surgery, simulation allows the MDT an opportunity to practice high-risk procedures and prompts the team to assess staff knowledge base, troubleshoot queries, and teach roles and responsibilities in a safe environment. In the context of COVID-19, simulation encourages staff sense of preparedness and protection for true participation during a high-risk procedure. This is of particular importance considering the high levels of staff anxiety and the necessity to maintain safe participation for staff and patients.
Footnotes
Authors’ Note
Rebecca Towning was the primary author of all drafts and involved in questionnaire development and data collection. Catherine Rennie involved in questionnaire development and reviewed all drafts of the article. Mark Ferguson involved in questionnaire development, statistics, and reviewed all drafts of the article.
Acknowledgments
The authors thank Talisa Ross, MRCS, Imperial College Healthcare NHS Trust, for assistance with collection of tracheostomy patient data.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.