
Abstract
A ganglion cyst of the temporomandibular joint is a benign lesion that may present as a mass on the anterior wall of the external auditory canal and should be differentiated from other skull base pathology prior to management.
Introduction
Ganglion cysts are rare masses of the external auditory canal (EAC). 1 -4 Typically, they present as a preauricular mass emanating from the temporomandibular joint (TMJ) with symptoms of pain and swelling. Less commonly, the presentation is a defect or lesion of the anterior ear canal wall. 5 We present the diagnosis and management of a TMJ ganglion cyst involving the EAC. This study was deemed exempt by the institutional review board of Loyola University Medical Center.
Case Report
A 70-year-old male was referred to the senior author for a right EAC lesion. The patient reported aural fullness with otorrhea, which resolved after a course of oral antibiotics. There were no symptoms associated with the TMJ nor a palpable mass in the preauricular region. Microscopic otoscopy of the right ear showed a curious cystic lesion attached to the anterior wall of the medial EAC. The lesion was soft upon palpation. An audiogram demonstrated a mild sloping to moderately severe sensorineural hearing loss in the right ear. Computed tomography (CT) showed a 7 × 5 mm soft tissue density along the anterior wall of the osseous EAC (Figure 1).
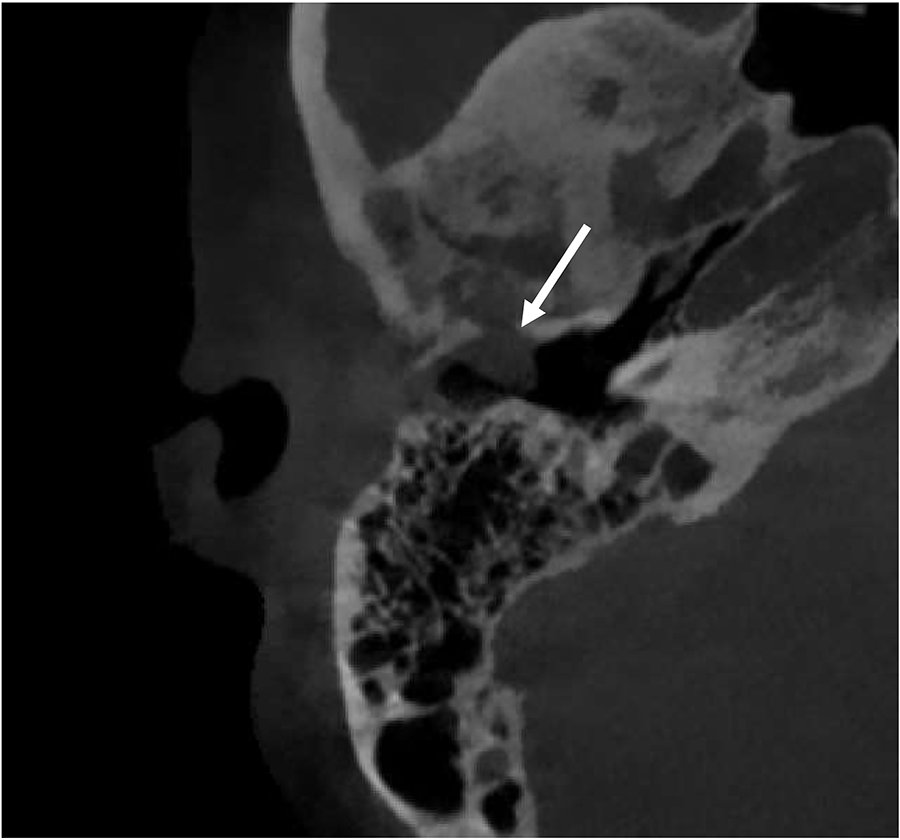
Axial computed tomography (CT) demonstrating the soft tissue mass in the right external auditory canal (EAC) with anterior bony erosion (arrow).
The patient was taken to the operating room for diagnosis and surgical management. Using an endaural approach, the ear canal skin was incised around the mass. The bony ear canal wall was drilled with a series of diamond bits. Eventually, the mass was pedicled on a stalk emanating from a canaliculus in the anterior superior portion of the bony ear canal. The lesion was removed en bloc with a cuff of normal skin around it. Temporalis fascia was used to cover the defect.
Histological examination revealed normal epidermis with an underlying solid and cystic lesion (Figure 2). The solid components varied from myxoid to densely collagenous. The cyst component contained mucinous material without a true epithelial lining. There were focal areas of fibrosis representing organization. Additional immunohistochemical stains showed no epithelial lining. The final diagnosis was a ganglion cyst.
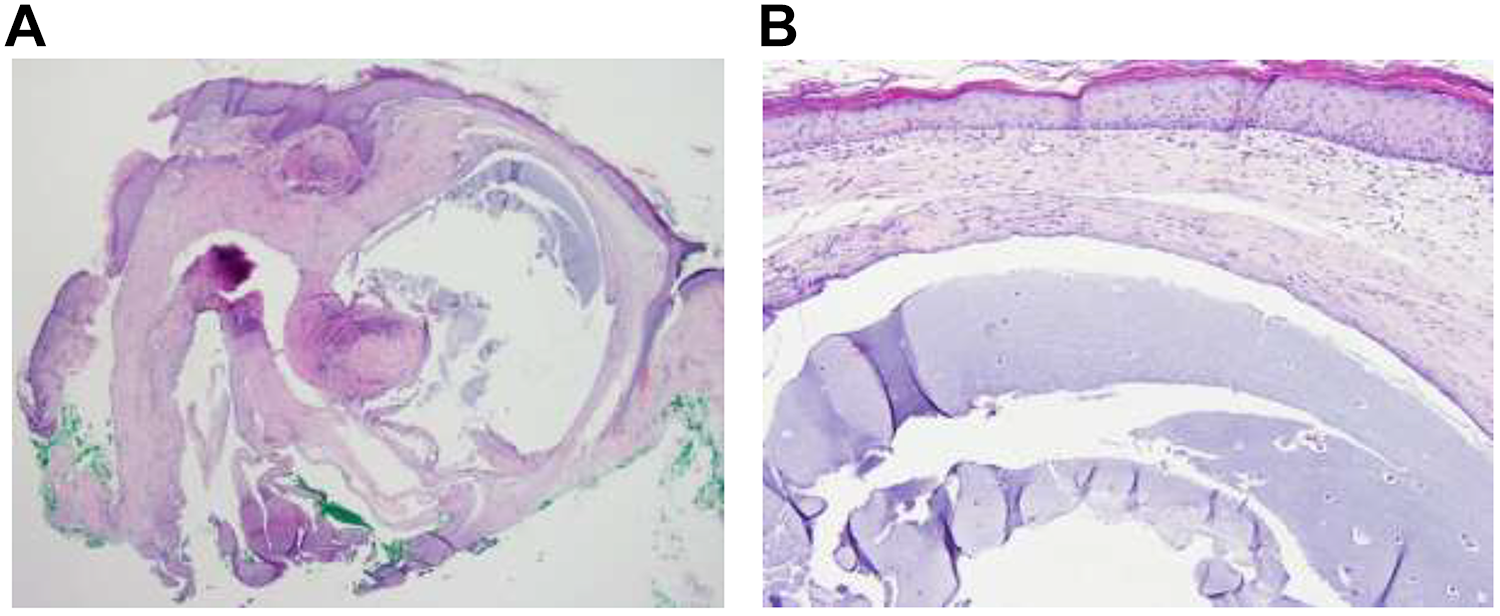
(A) The resected lesion at low power shows normal epidermis with loose, myxoid solid component and adjacent cystic component. Extension of the myxoid material into the surrounding tissue incites the reactive myofibroblastic proliferation. (B) The cyst has no true epithelial lining but a dense collagenous outer layer. No significant nuclear atypia or mitoses are present.
Follow-up visits at 1 and 4 months showed a well-healed ear canal with no evidence of residual or recurrent cyst.
Discussion
Ganglion cysts of the TMJ are benign lesions typically found in young adults with a higher incidence in females. 4 The pathophysiology of ganglion cysts is thought to be chronic and repetitive trauma leading to myxoid degenerative changes in the connective tissue. 3 One of the distinguishing pathologic features of ganglion cysts is the lack of an epithelial lining. 2
The classic location of a TMJ ganglion cyst is the preauricular region. 4 Less frequently, it presents as a mass in the EAC. 4 Common symptoms include TMJ swelling and pain. Patients may also complain of trismus, tinnitus, and otorrhea, which raise greater concern for EAC involvement. 4
The most common benign lesions of the EAC are osteomas and exostoses, although, an exhaustive differential diagnosis for an EAC mass consists of benign, malignant, and infectious or inflammatory etiologies (Table 1). 3,5 Ganglion cysts are soft upon palpation and may fluctuate in size when opening and closing the mouth. 1
Differential Diagnosis of Masses in the External Auditory Canal.a
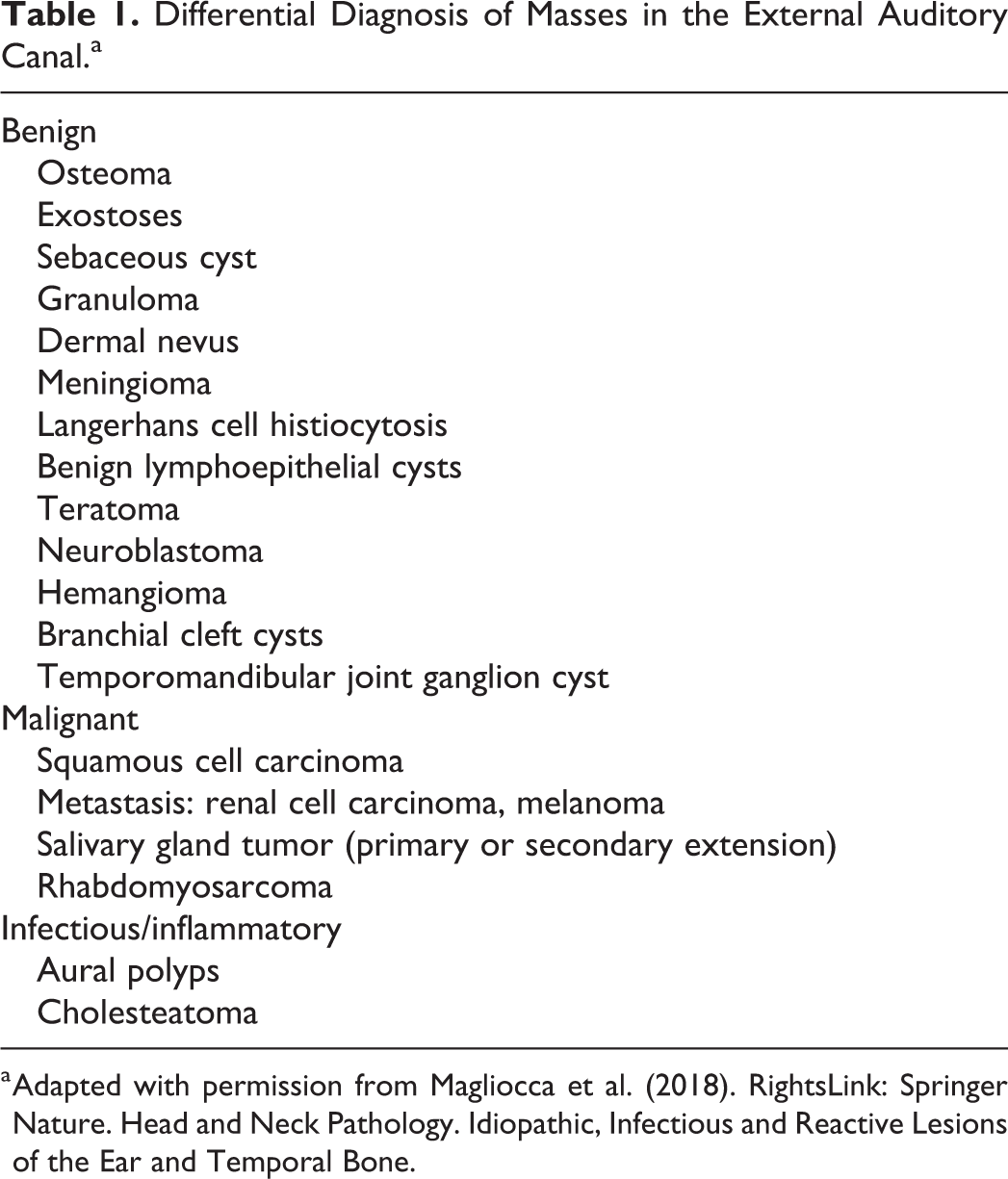
a Adapted with permission from Magliocca et al. (2018). RightsLink: Springer Nature. Head and Neck Pathology. Idiopathic, Infectious and Reactive Lesions of the Ear and Temporal Bone.
An audiogram and CT help determine the management of ganglion cysts when discovered in the EAC. A conductive hearing loss may be present if the ear canal is obstructed but is otherwise unlikely. Radiologic imaging is needed to ascertain the extent of the lesion and the amount of bony erosion. In addition to 2 prior case reports, our patient’s CT showed a direct bony erosion from the TMJ into the EAC.
Surgical management can be diagnostic and therapeutic. A preoperative transcanal biopsy was performed in 2 cases. 3,4 If there is uncertainty about the nature of the lesion, a biopsy is reasonable. However, obtaining imaging first is imperative to rule out a skull base lesion. We performed a simple endaural approach with canalplasty and placement of a fascia graft over the TMJ communication. Surveillance alone is an option if the patient is asymptomatic, as in the case report by Esmaili et al. 1 More aggressive approaches, including resection of the mandibular condyle and partial resection of the TMJ capsule, may be necessary for larger and more symptomatic lesions. 3
Ganglion cysts of the EAC are rare, with this case being the fifth reported in the literature. Typically, a TMJ ganglion cyst presents as a preauricular mass with trismus and/or pain. When presenting as a mass in the EAC, aural fullness is the most common symptom and examination shows a small cyst on the anterior wall. Hearing is not affected in most of these patients unless there is complete canal obstruction. Imaging with CT aids in diagnosis and helps determine the extent of bony erosion. Given the benign nature of ganglion cysts, we believe a conservative surgical approach should be implemented for symptomatic patients and surveillance for those asymptomatic.
Footnotes
Authors’ Note
Aaron M. Domack contributed to design, manuscript drafting and revision. Aayushma Regmi contributed to pathology photos and descriptions. John P. Leonetti contributed to manuscript drafting and revision. IRB exempt.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.