
Abstract
Significance Statement
Facial nerve schwannoma is extremely uncommon. Despite its rarity, it is considered the most common facial nerve tumor and potentially affects any segment of the nerve. Presenting symptoms vary depending on the location of the neoplasm. Tumors pertaining to the extratemporal course of the nerve mainly appear as an asymptomatic parotid mass. We present a rare case of schwannoma of the zygomatic branch of the right facial nerve that was surgically resected, without facial nerve injury.
A 27-year-old man presented to our Ear, Nose and Throat (ENT) Department, with a 10-month history of an enlarging lump on his right zygomatic region. The patient’s medical history was clear, except for a G6PD deficiency. No history of pain, fever, or facial weakness was reported. On examination, there was a solitary, soft, superficial, mobile lesion in the right zygomatic prominence. The overlying skin was normal, and there was no cervical lymphadenopathy. A full ENT examination did not reveal any pathological findings. Laboratory tests were found to be within normal limits.
Further, radiographic investigation was planned. Computed tomography of facial bones demonstrated a round mass 2. 3 × 1.5 × 1 cm over the right zygomatic arch (Figure 1). Patient was informed about the findings and gave his consent for excision under general anesthesia. Intraoperative continuous facial nerve monitoring through a stimulating probe was used whenever needed. Beneath the mass, the zygomatic branch of the facial nerve was identified. The tumor was hard without, however, any evidence of infiltration into the surrounding tissues. The lesion was totally excised and the postoperative course was uneventful (Figure 2). The evaluation of the right facial nerve function was normal.
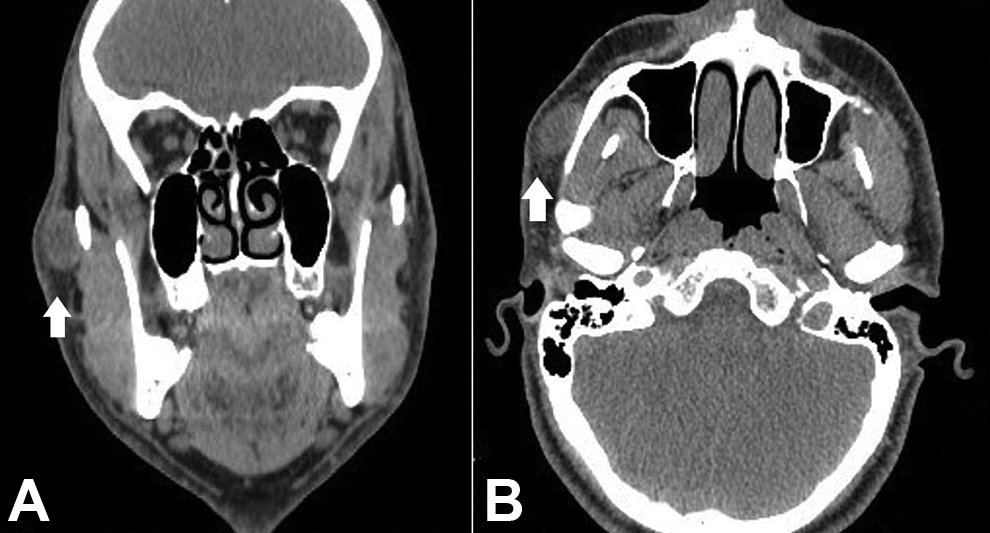
Coronal (A) and axial (B) CT images of facial bones showing a round lesion 2.3 × 1.5 × 1 cm over the right zygomatic arch (white arrows). CT indicates computed tomography.
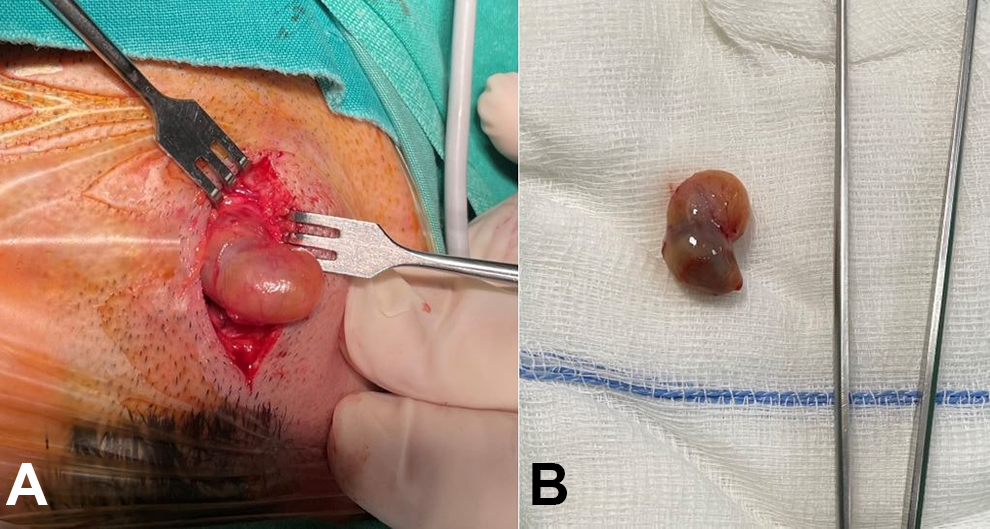
(A) Intraoperative image of the surgical excision. (B) Specimen of the lesion.
Histopathology and immunochemistry findings were consistent with a facial nerve schwannoma (FNS), with hemorrhagic cystic degeneration. Biphasic tumor with highly ordered cellular component (Antoni A) plus myxoid hypocellular component (Antoni B) was revealed, as well as a strong immunoreactivity for S100 (Figure 3).
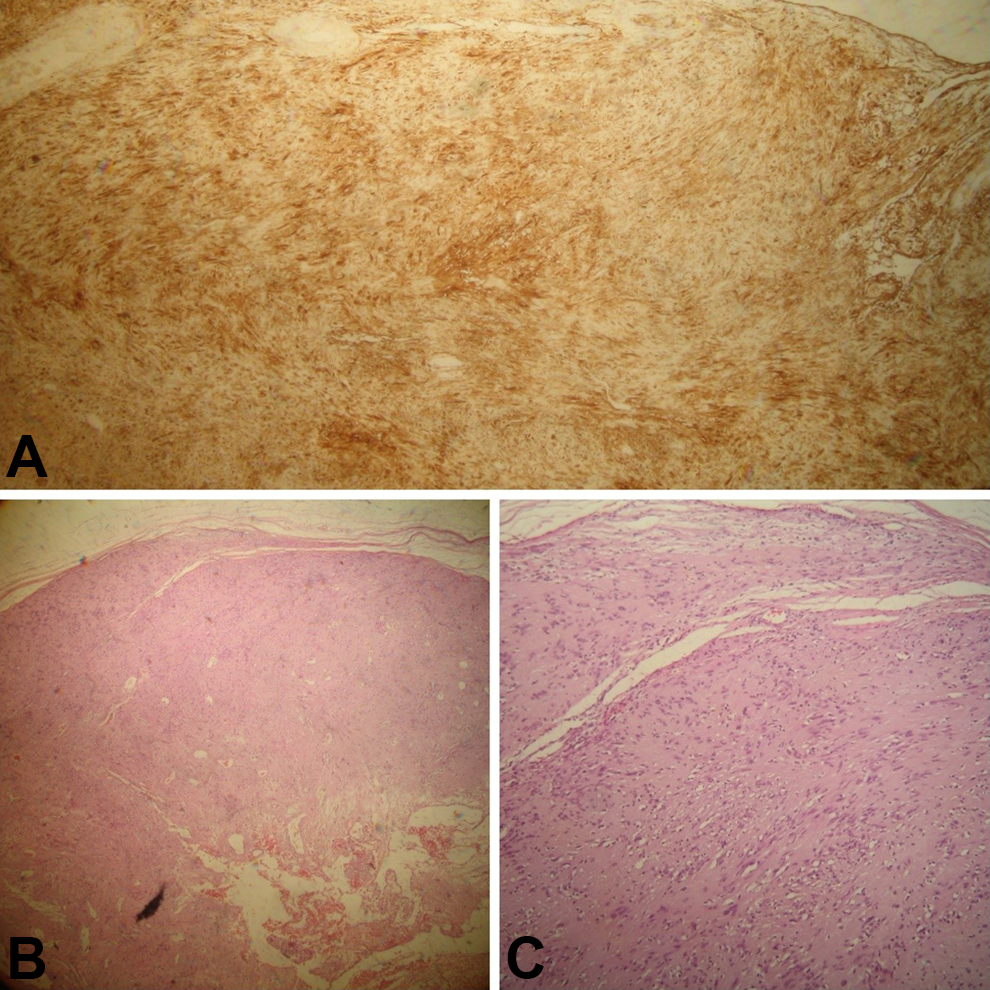
Histopathological examination of the lesion. (A) Immunohistochemical analysis shows diffuse positive staining for S100 protein indicating neural origin of the tumor (S100 immunostaining, magnification ×4). (B) Fibrous capsule underneath which is a proliferation of spindled Schwann cells, with areas of higher cellularity (Antoni A) and myxoid hypocellular (Antoni B) areas (H&E stained, magnification ×4). (C) Tumor capsule and Schwann cells (mainly Antoni A areas) (H&E stained, magnification ×10). H&E indicates hematoxylin and eosin.
Six-month follow-up did not reveal any recurrence, swelling, scar, or facial nerve palsy. Schwannomas are benign neurogenic, usually encapsulated, neoplasms that derive from the Schwann cells of the sheath of peripheral nerves, including the distal parts of most cranial nerves. 1,2 These tumors can be found anywhere in the body but are mostly described in the head and neck, especially in the maxillofacial area. 3 Facial nerve schwannomas are very rare. 1 They can include one or more portions of the facial nerve and are mainly unilateral. 4 Bilateral FNSs are associated with neurofibromatosis type 2. 4 They can be categorized into extratemporal (mainly refer to the intraparotid segment of the facial nerve) and intratemporal (tumors involving temporal segments of the facial nerve) types. 1 The majority (about 90%) are related to the intratemporal part of the nerve. 5 The clinical presentation of FNSs depends on their location with extratemporal tumors presenting as painless swellings of the parotid gland without facial nerve palsy. 1,5 Even less often, extratemporal FNSs that do not affect the parotid gland manifest themselves as asymptomatic swellings of the facial region. 1 Most common symptoms of an intratemporal FNS are sensorineural hearing loss, vertigo, tinnitus, and facial nerve dysfunction. 6 Generally, the preoperative diagnosis of an FNS is challenging. 1 Neurofibroma, granular cell tumors, lipoma, fibroma, leiomyoma, and salivary gland tumors should be taken under consideration for the differential diagnosis of the extratemporal tumors. 1,3 Cholesteatoma, middle ear cerebellopontine angle tumors should be eliminated, as far as the intratemporal FNSs are concerned. 4 The routinely performed imaging methods for the evaluation of the FNSs are high-resolution computed tomography of the temporal bone and gadolinium-enhanced magnetic resonance imaging. 1,4 Histopathologically, the schwannomas are encapsulated and may demonstrate cystic degeneration and hemorrhage. They also present with characteristic tissue patterns which are known as Antoni A and Antoni B areas. 7 Malignant transformation of schwannomas is extremely rare. 1,3 The best treatment option for the FNSs is the complete surgical excision, with facial nerve preservation. 1,4 Gamma knife radiosurgery is also another treatment option, especially for small or residual/recurrent tumors. 8
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.