
Abstract
Endovascular embolization (EE) has become an effective method for the treatment of intractable epistaxis (IE). However, complications such as facial pain, headaches, aphasia, hemiplegia, and transient blindness can also occur during or after surgery. In this article, we report a rare case of IE with residual intravascular guidewire after EE. Open surgery was used to remove the guidewire. However, to avoid serious complications such as massive hemorrhage, only part of the guidewire was removed.
Introduction
Epistaxis is the most common emergency in otorhinolaryngology. 1 It is estimated that up to 60% of individuals experience the condition in their lifetime. 2 A subset of patients cannot be effectively controlled and will progress to intractable epistaxis (IE). Local compression, nasal packing, endoscopic hemostasis, surgical ligation, and endovascular embolization (EE) are commonly used treatment methods for IE. In 1974, Sokoloff et al first described EE as a new treatment for IE. 3 However, complications such as hemiplegia, blindness, headache, and facial edema may arise after embolization. 4 In this article, we report a case of IE who was treated by EE. However, the intravascular guidewire was left in the vessels after embolization extended from the innominate artery (IA) to the maxillary artery (MA). Open surgery instead of interventional surgery was used to remove the guidewire. To avoid serious complications, only part of the guidewire was removed.
Case Report
A 39-year-old male patient with IE received EE at a local hospital 2 months before admission. The responsible vessel was successfully embolized during that operation, and no further epistaxis occurred. However, the superselective guidewire could not be removed after the operation and had remained in the vessels since the surgery. The guidewire could be clearly seen in the IA, the right common carotid artery (CCA), and the right external carotid artery (ECA) on computed tomographic angiography in a local hospital (Figure 1). Carotid Duplex ultrasonography in our hospital revealed that a linear hyperecho could be seen in the lumen from the IA, the right CCA, and the right ECA to the MA. Part of the guidewire from the proximal CCA to the distal CCA floated in the vessel (Figure 2A), while other parts were relatively fixed, and no floating was seen (Figure 2B). The patient had been previously healthy, no positive signs were found in the physical examination on admission, and the laboratory examination results were normal.
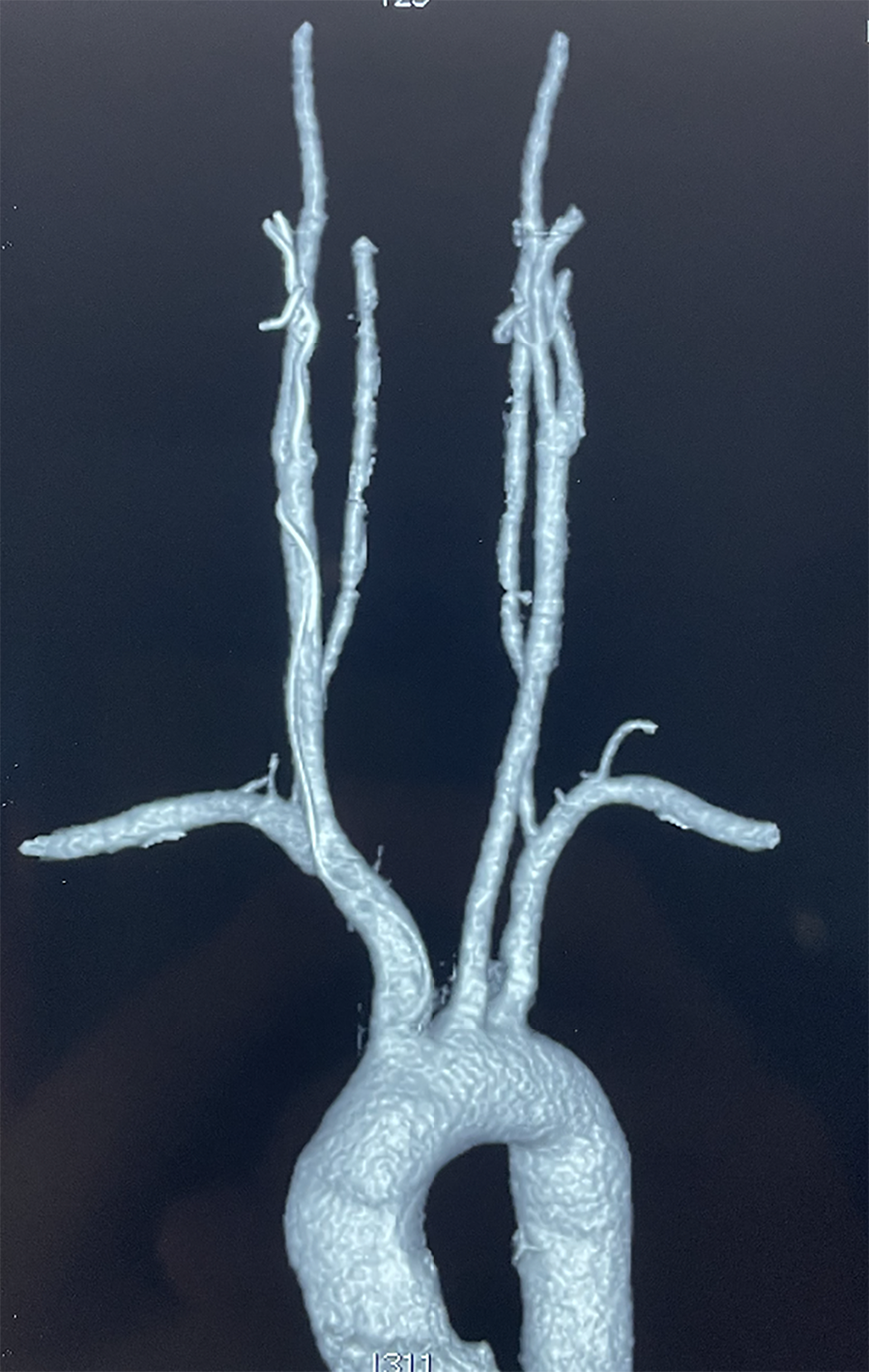
The guidewire can be clearly seen in the innominate artery (IA), the right common carotid artery (CCA), and the right external carotid artery (ECA).
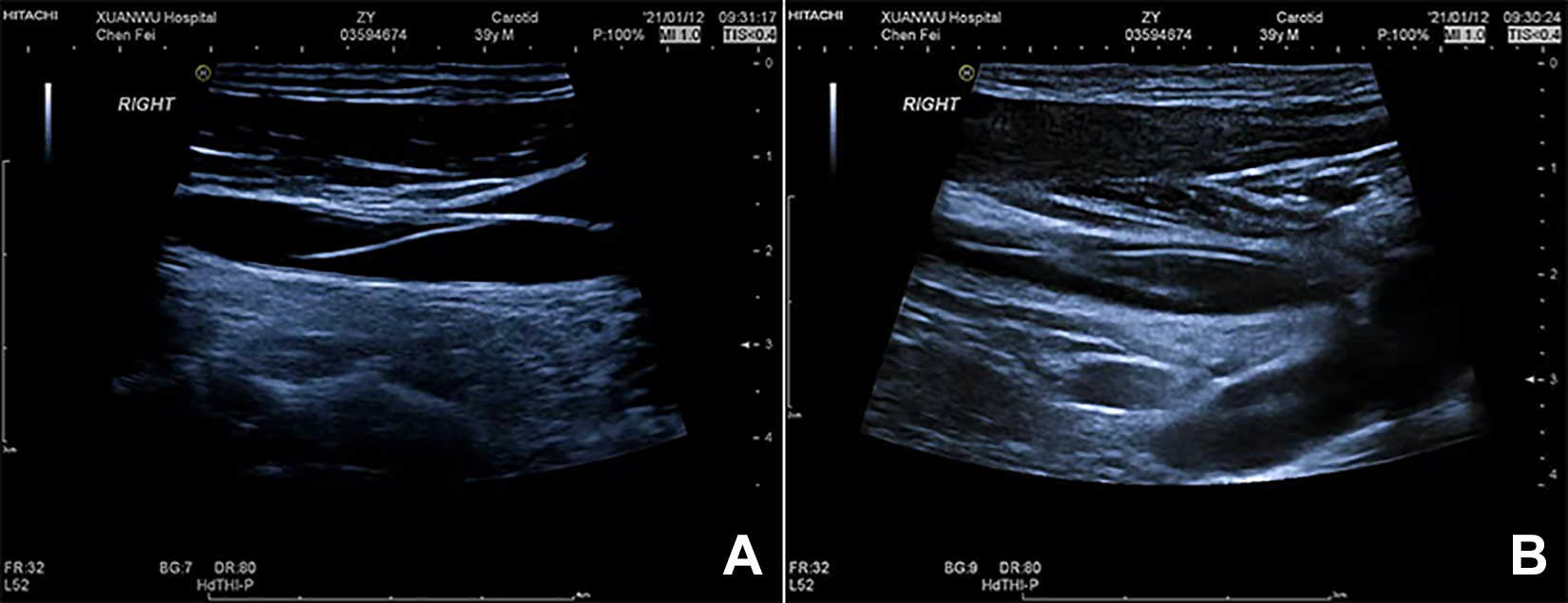
A, The part of the guidewire extended from the proximal common carotid artery (CCA) to the distal CCA was floating. B, The part of the guidewire extended from the right external carotid artery (ECA) to the maxillary artery (MA) was relatively fixed.
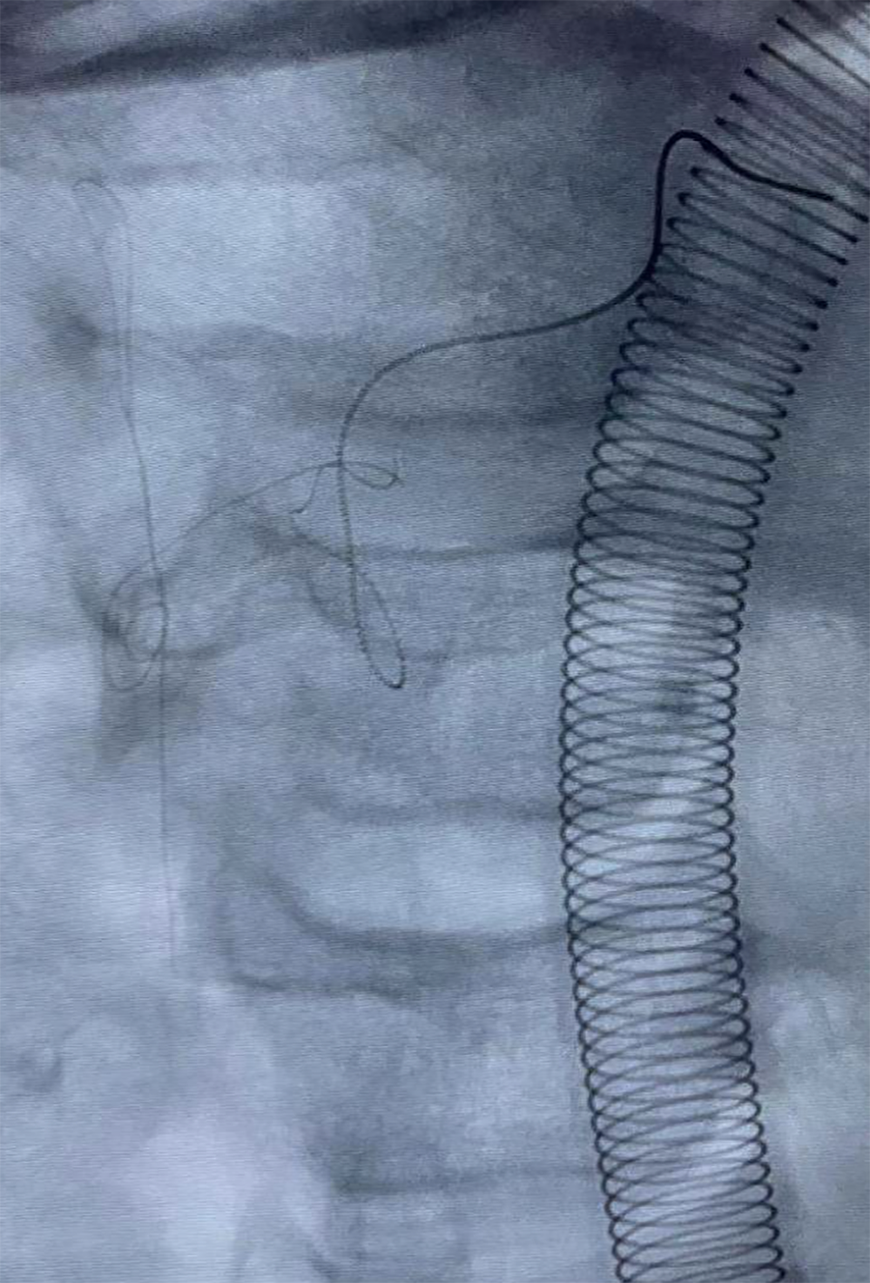
After completing the comprehensive preoperative examination and confirming this patient had no surgical contraindications, open surgery under general anesthesia was performed. At the beginning of the operation, we further clarified the position of the guidewire under fluoroscopy (Figure 3). A nearly 1-cm longitudinal incision was made on the ECA, and the guidewire could be clearly seen in the artery. The part of the guidewire below the incision was easily pulled out (Figure 4), while the part of the guidewire above the incision could not be pulled at all. We then cut the guidewire at the level of the incision and closed the wound layer by layer. Fluoroscopy after surgery confirmed that the guidewire above the incision was left in the artery (Figure 5). The patient was discharged 5 days after surgery and has had no complaints of any discomfort thus far.
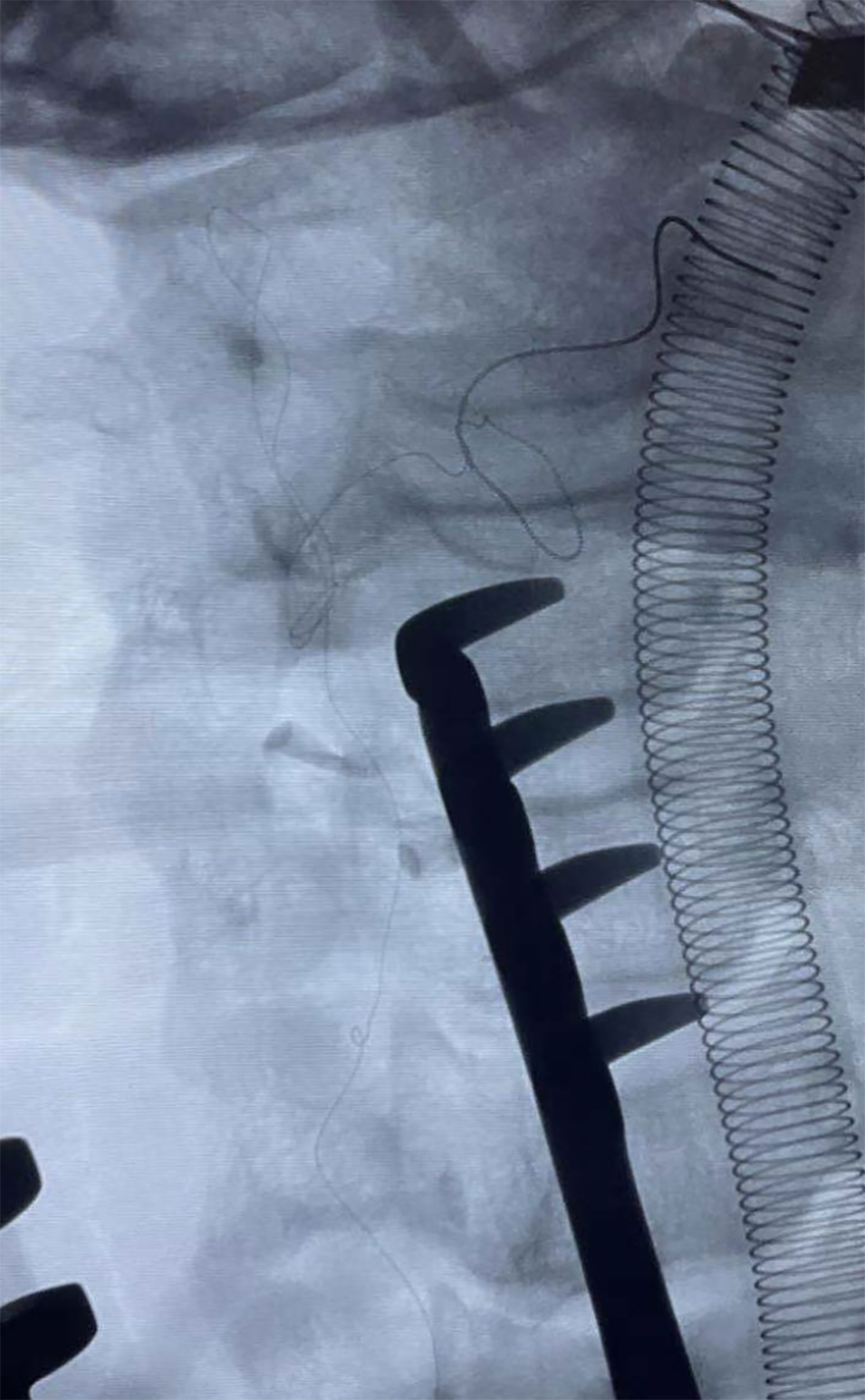
The intravascular guidewire was extended from the innominate artery (IA) to the maxillary artery (MA).
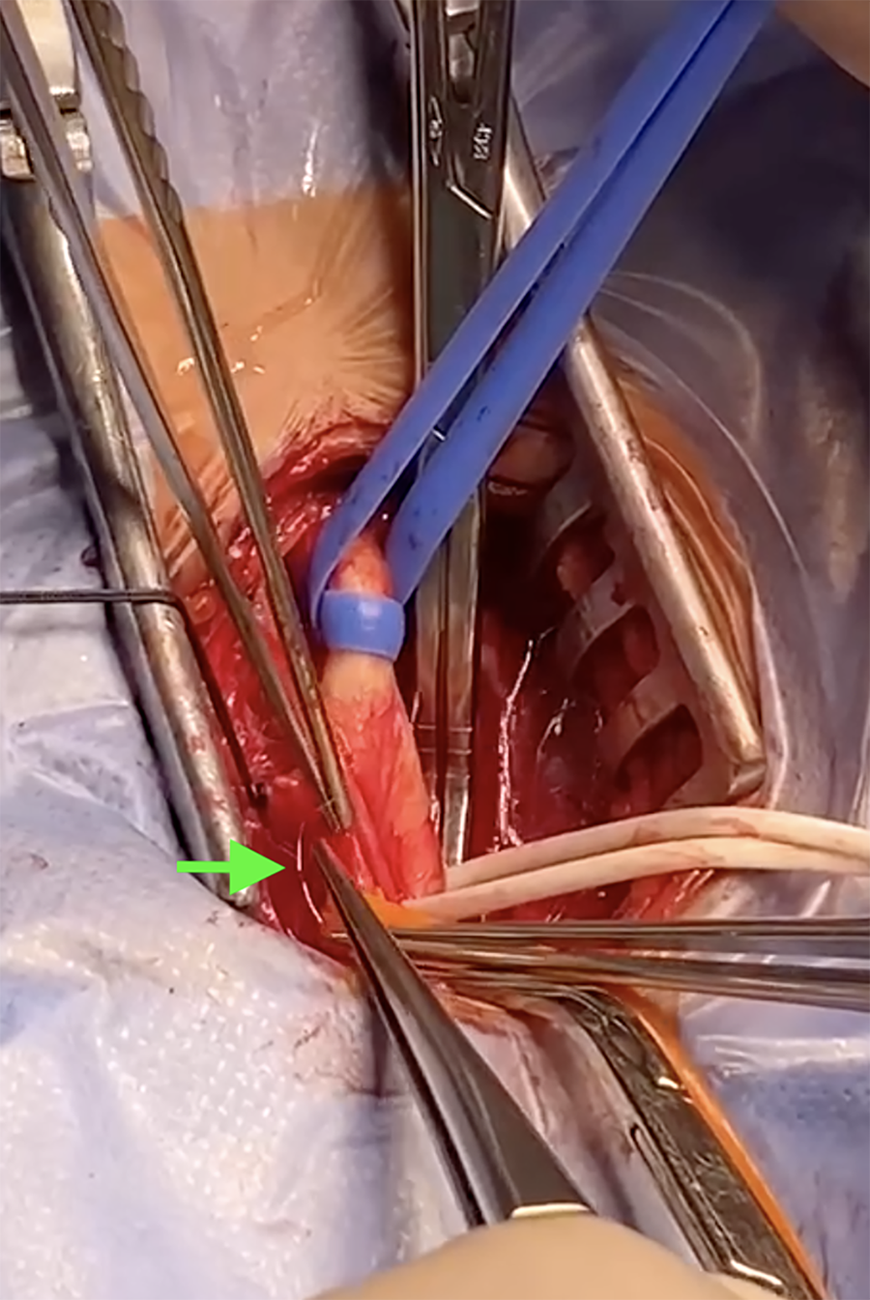
The part of the guidewire below the incision was pulled out from the artery.
The guidewire above the incision was left in the artery.
Discussion
Epistaxis is a common case in the emergency department. Causes of epistaxis include oral anticoagulants, seasonal variation, air humidity changes, and vascular malformation. 5 Most patients with epistaxis can be effectively controlled by conservative measures and do not need hospitalization. Unfortunately, some of them will progress to IE, which can be a life-threatening situation and requires timely treatment.
Based on the source of the bleeding site, epistaxis can be divided into 2 types: anterior and posterior. Most epistaxis cases arise from the anterior septal area, while IE cases are mainly posterior in clinical practice. 6 IE is more common in adult patients, and management of IE poses a huge challenge. Local compression and nasal packing may be used as the initial attempts to control bleeding, but the success rates of these methods are not encouraging and can even lead to serious complications. Surgical ligation of the ECA was first performed by Hyde in 1925. 7 Since then, the sphenopalatine artery, internal maxillary artery, and anterior ethmoid artery have gradually become alternative vessels of ligation and can provide targeted therapy for IE. However, complications including acute sinusitis, orbital injury, and rebleeding after surgery can still occur.
In the past few decades, EE has gained wide popularity as a treatment for IE. 8,9 Some otolaryngology surgeons have considered EE to be the preferred treatment for IE due to its advantages, such as less trauma, short operation time, and quick rehabilitation after embolization. Studies have shown that the success rate of EE can reach more than 90%. 10,11 Even with the advantages mentioned above, complications after EE cannot be ignored and can be divided into minor complications and major complications. 12 Minor complications include fever, headache, facial pain, facial edema, groin hematoma, and paresthesias. Major complications include tissue ischemia, monocular blindness, hemiparesis, and stroke. We report a rare case in this article. The patient received embolization at a local hospital before admission. After embolization, the superselective guidewire was left in the vessels and could not be removed. Computed tomographic angiography showed that the guidewire was extended from the IA to the MA.
With the continuous development of endovascular surgery, the field of intervention continues to expand; therefore, the accompanying complications and accidents also increase. Metal foreign bodies remaining in the vascular cavity are clinically rare, and the causes are mostly iatrogenic. In cases of IE, guidewires remaining in the carotid artery after EE are very rare. A foreign body in the CCA can directly affect the blood entering the skull and cause thrombosis around the foreign body, which can lead to acute cerebral ischemia, acute cerebral infarction, and other serious complications. Therefore, once foreign bodies are found in the arteries of the head and neck, they should be removed as soon as possible to prevent the occurrence of cerebral ischemic events. Fortunately, in our case, no cerebrovascular events had occurred before the operation. We chose open surgery rather than interventional surgery to remove the guidewire. Based on preoperative imaging results, we made a longitudinal incision in the ECA. Considering that the difficulty of removing the guidewire from the ECA and leaving the guidewire in the ECA would not cause serious cerebral ischemic complications, we removed the part of the guidewire extending from the IA to the CCA, while the part of the guidewire above the incision remained in the artery.
Conclusion
We report a rare case after EE for IE. However, the intravascular guidewire was left in the vessels after embolization. To avoid serious and fatal complications, open surgery instead of interventional surgery was used to remove the guidewire. The part of the guidewire extending from the IA to the CCA was completely removed, while the part of the guidewire above the incision was left in the artery. No symptoms have occurred after surgery thus far.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.