
Abstract
Recurrent respiratory papillomatosis is a condition caused by human papilloma virus, usually sub types 6 and 11. Papillomas are benign neoplasms that are most commonly found on the larynx and can be often associated with significant airway involvement. Frequency of episodes varies among patients as do the clinical symptoms. Patients often present with symptoms such as hoarseness but there is potential for respiratory compromise and even complete airway obstruction.
Treatment options for recurrent respiratory papillomatosis (RRP) usually involve careful debridement, with different approaches involving endoscopic removal via coblator, laser, or microdebrider. Medications have been pursued as adjuvant options to attempt remission of lesion regrowth, though no approach has been proven to provide a consistent response. The following case was deemed exempt from institutional review board review and oversight. This report describes the use of bevacizumab therapy as the initial choice for adjuvant treatment in a patient with an aggressive form of RRP.
We report on a 5-year-old female who presented to the emergency department with respiratory compromise. Her parents reported progressive hoarseness over the previous several months with worsening stridor. Flexible laryngoscopy showed extensive glottic and subglottic lesions indicative of severe laryngeal papilloma disease. She underwent debridement with microdebrider (Figure 1). Recurrent lesions quickly redeveloped and subsequent debridement with postoperative steroid course took place during the same admission. After discussion with parents, repeat debridement with intralesional bevacizumab injection was performed given the severity of her disease course and frequency of her recurrence. Following a second intralaryngeal injection delivered a week later, she was started on a course of systemic bevacizumab therapy 10 mg/kg every 3 weeks without later return of symptoms and complete response after 4 weeks of therapy (Figure 2). After 5 treatments, the interval of therapy was extended to every 4 weeks. The patient has received a total of 8 treatments with continued complete response.
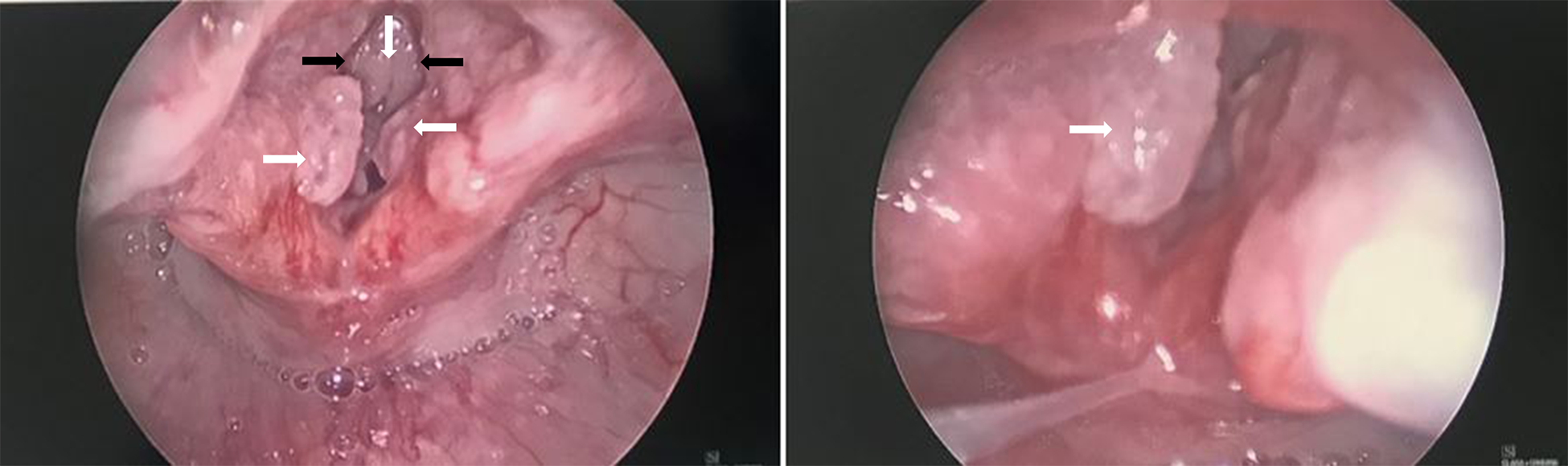
Direct laryngoscopy images show early disease course identifying numerous papillomatous lesions (white arrows) prior to systemic adjuvant therapy with anterior commissure as well as bilateral true and false cord involvement. True vocal cords are identified (black arrows).
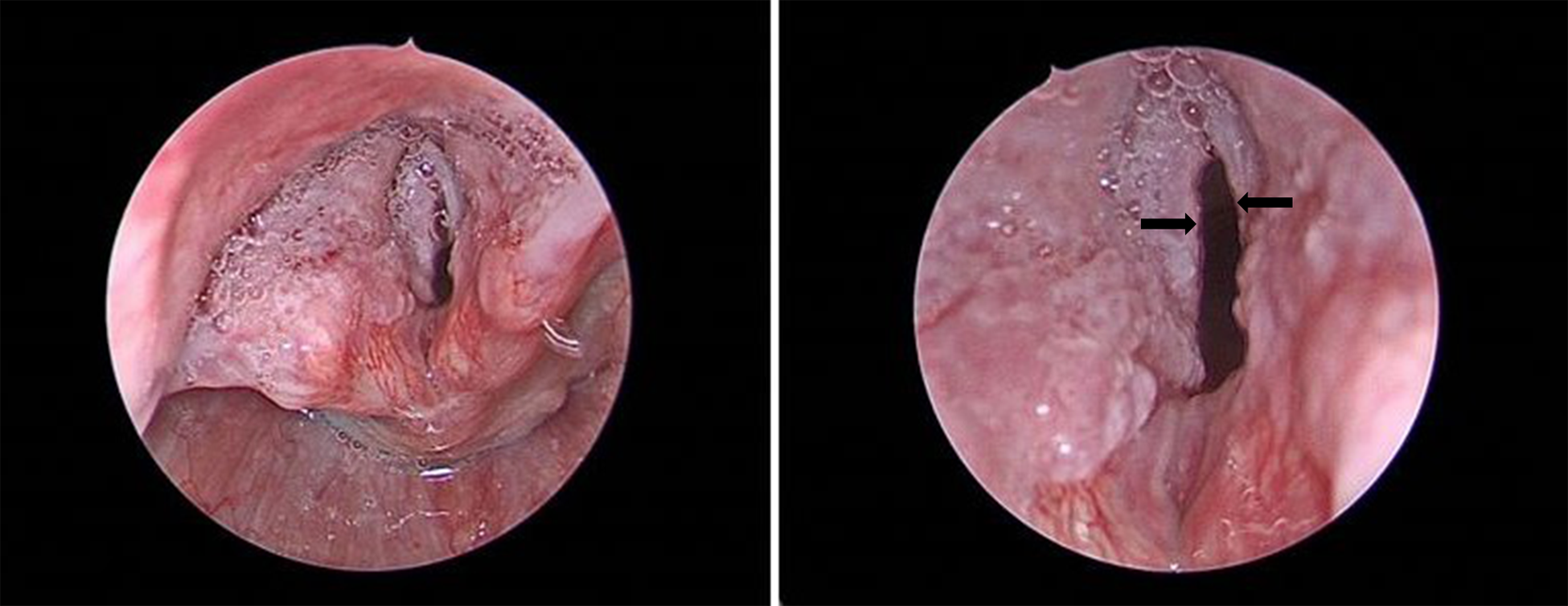
Views of the larynx on direct laryngoscopy following systemic bevacizumab therapy show absence of papillomas 4 weeks following initiation. True vocal cords (black arrows) and patent airway is visualized without obstruction from previous papillomas.
In our case of severe RRP, the patient underwent an extensive surgical course over a 6-week period with minimal improvement in overall disease burden. Of note, no adjuvant therapy was tried prior to bevacizumab initiation though other treatment options have previously been reported for RRP such as cidofovir, interferon α, and therapeutic use of the Gardasil human papilloma virus vaccine. 2,3 Our patient ultimately underwent a systemic regimen consistent with the current dosing standard of 10 mg/kg. She promptly responded to treatment without subsequent sequelae or recurrence of disease.
Recurrent respiratory papillomatosis has an unpredictable and often complicated clinical course. Surgical treatment with debridement alone has not been proven to reduce the rate of recurrence and outcomes are variable. 1 -3 In the pediatric population, patients undergo an average of 4.1 to 5.1 procedures annually, especially in the first year of diagnosis. 1,4,5 To our knowledge, the use of systemic bevacizumab therapy for treatment of RRP has not been studied in clinical trials though previous case studies have been reported. Bevacizumab is a recombinant humanized monoclonal antibody that inhibits angiogenesis by preventing vascular endothelial growth factor from binding with its receptors. 5 Case series and surveys have shown that systemic bevacizumab therapy may offer potential resolution or at the very least a decreased requirement for surgical intervention. 2 -5
Its use here as an initial adjuvant agent demonstrated a rapid complete response and identifies the potential for bevacizumab to become a preferred option for RRP management. This case report adds to the body of evidence that systemic bevacizumab therapy can offer favorable outcomes in RRP. Further study of this treatment is warranted to better identify its role in the treatment of advanced RRP.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.