
Abstract
Objective:
To review the literature on Hyrtl fissure (HF) and contribute our experience with a 2-year old who developed cerebrospinal fluid (CSF) otorrhea during routine tympanostomy tube placement.
Methods:
Data Sources: Pubmed and Google Scholar searches were conducted of articles in the English language literature from all time periods using the words Hyrtl, Hyrtl’s fissure, HF, and tympanomeningeal fissure. Study Selection: All relevant articles were reviewed to identify cases of HF.
Results:
Data Extraction: Nineteen cases, including ours, are described. Patient characteristics, method(s) of diagnosis and repair, and outcomes are reported. Computed tomography and intraoperative endoscopic images from our case are included. Presentation is more common in children (66.7% of cases where age was stated, n = 10) than in adults (33.3%, n = 5), and is most commonly unilateral (89.5%, n = 17). Cerebrospinal fluid otorrhea was the most common presentation. Six were discovered after tympanostomy tube placements while 3 were identified during cochlear implant work-up or after device failure. Surgical approaches described include endaural, transcanal, retrosigmoid, postauricular, and posterior fossa endoscopic. Multiple materials including bone wax, bone pate, fascia, muscle, and tissue sealant have been used. Our case describes an endoscopic repair in a child, which was successful at a 2-year follow-up. Data Synthesis: The small number of cases limits the utility of statistical analysis (n = 19).
Conclusions:
Hyrtl fissure is a rare but important entity that may be discovered when routine procedures have unexpected results. Hyrtl fissure should be included in the differential diagnosis when there is persistent clear otorrhea after a tympanostomy tube, cochlear implant misinsertion, meningitis, or unexplained middle ear effusion in an adult.
Keywords
Introduction
Hyrtl fissure (HF) is one of several known congenital communications between the posterior cranial fossa and middle ear via the temporal bone. Others include an enlarged cochlear aqueduct, facial canal, fallopian canal (internal auditory canal), or petromastoid canal. In their review of lateral skull base defects, Remenschneider et al describe 3 categories of fistulous pathways based on 35 temporal bone specimens: transdural, labyrinthine, and perilabyrinthine. 1 Transdural communication into the middle ear space can be caused by arachnoid granulations, bony defects, and/or meningoceles. Labyrinthine defects appear to cause leakage of cerebrospinal fluid (CSF) through the oval window and are frequently associated with congenital modiolar defects and stapes footplate defects, as well as nonotologic congenital defects which are frequently fatal. In their series of 10 temporal bones with labyrinthine defects, the median age at the time of death was <12 months, and only 2 patients had survived into adulthood. Hyrtl fissure is described as the most common perilabyrinthine defect, occurring unilaterally in 3 temporal bone specimens of 52 examined. They also suggested that perilabyrinthine defects may be difficult to detect and may pose a higher risk of intracranial complications compared with transdural or labyrinthine sources. 1 As any of these temporal bone defects may lead to CSF otorrhea, there is a potentially life-threatening risk of developing meningitis. Indeed many articles which mention HF do so in passing, in the context of potential causes of CSF leaks or meningitis. 2 -5
Owing to its rarity, the incidence, epidemiology, natural history, and potential sequelae of HF remain largely unknown. The goal of this article is to gather what is known, add our experience, and analyze the cumulative information to identify heretofore undescribed patterns in order to help Otolaryngologists better understand and treat this important entity.
Materials and Methods
Using PubMed and Google Scholar, results for searches of “Hyrtl fissure,” “Hyrtl’s fissure,” and “tympanomeningeal fissure” were reviewed for all time periods in the English language. Although numerous articles mention HF, a total of just 18 unique cases were identified. Many of these accounts lacked critical information such as patient age, laterality, clinical presentation, audiometric findings, and outcome. Our own case brings the total to 19, summarized in Table 1. Informed consent for all included images was obtained from the patient’s family.
Summary of Cases of Hyrtl Fissure in the Literature.
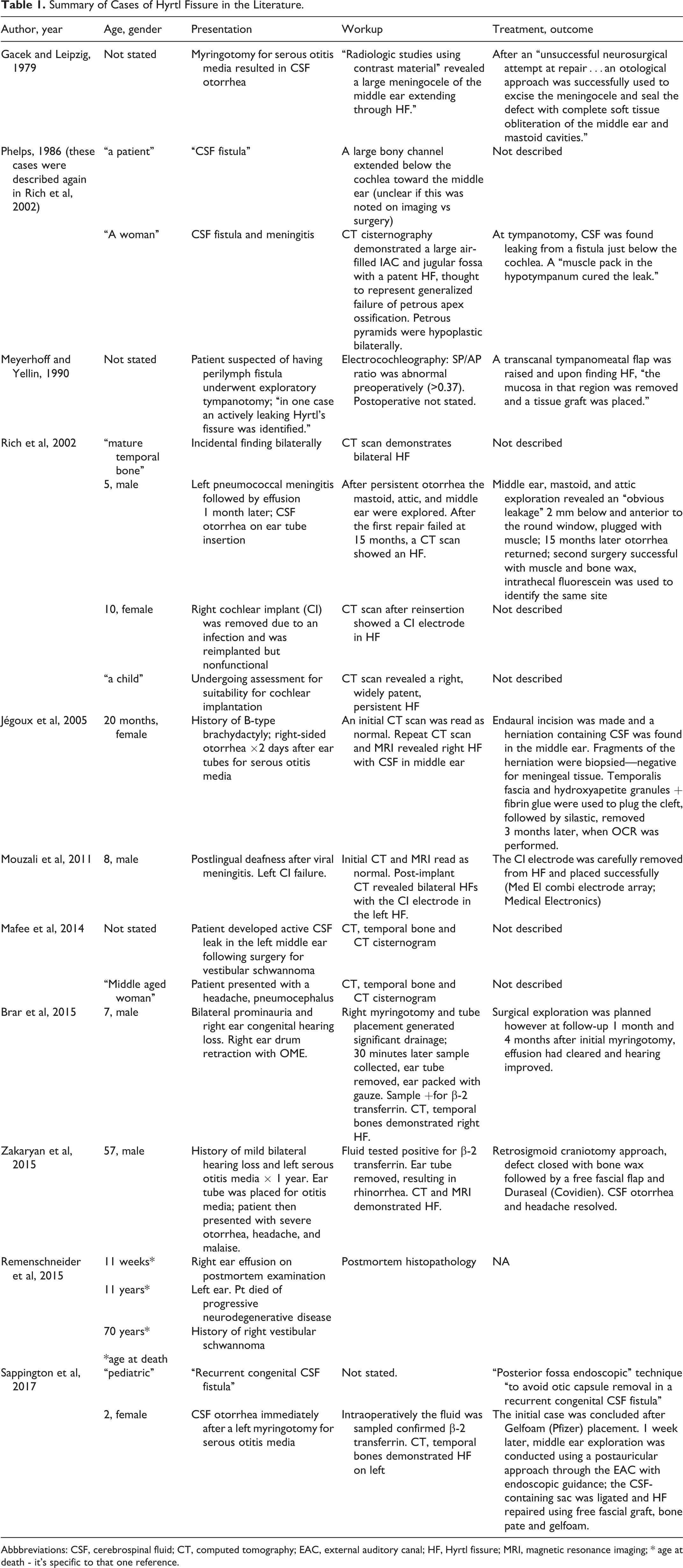
Abbbreviations: CSF, cerebrospinal fluid; CT, computed tomography; EAC, external auditory canal; HF, Hyrtl fissure; MRI, magnetic resonance imaging; * age at death - it's specific to that one reference.
Results
Case Presentation
Our patient is an otherwise healthy 2-year-old girl who underwent routine tympanostomy tube placement for presumed chronic otitis media with effusions with associated conductive hearing loss. The right-sided tympanostomy tube was placed without difficulty; however, upon making a left-sided myringotomy, a rush of clear fluid filled the external auditory canal (EAC) and the fluid continued to fill in a pulsatile nature, despite evacuation. A sample of the fluid was sent for β2-transferrin testing which confirmed the fluid as CSF. The EAC was packed with Gelfoam (Pfizer) and the case concluded. She was discharged with a course of oral antibiotics, and a noncontrasted computed tomography (CT), temporal bone, was obtained. This revealed an aberrant communication between the posterior fossa and the hypotympanum which was consistent with an HF (Figure 1), with normal right-sided anatomy.
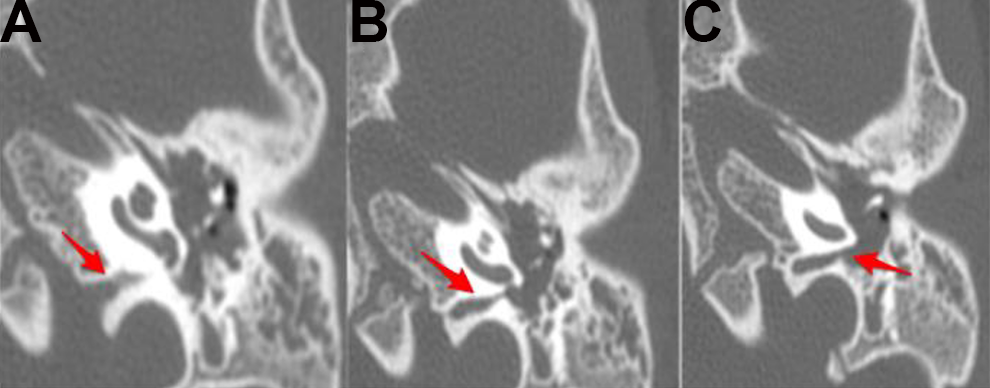
A-C, Axial computed tomography images of the left temporal bone demonstrating Hyrtl fissure connecting posterior fossa to the hypotympanum. Laterally, it terminates just inferior to the round window niche.
The patient was brought back to the operating room one week later. A left middle ear exploration was conducted with endoscopic assistance. Immediately upon entering the middle ear space after the tympanomeatal flap was raised, a membranous sac filled with CSF in the middle ear cleft was encountered. Once the ossicles were identified and found to be intact, the sac was explored and its stalk was discovered to be emanating from an HF directly adjacent and inferior to the round window niche (Figure 2). The fissure was packed with fascia, followed by bone pate and Gelfoam which seized the CSF egress. The ear was then closed in a standard fashion. At the 2-year follow-up, the CSF otorrhea had not recurred and the conductive hearing loss remained resolved.
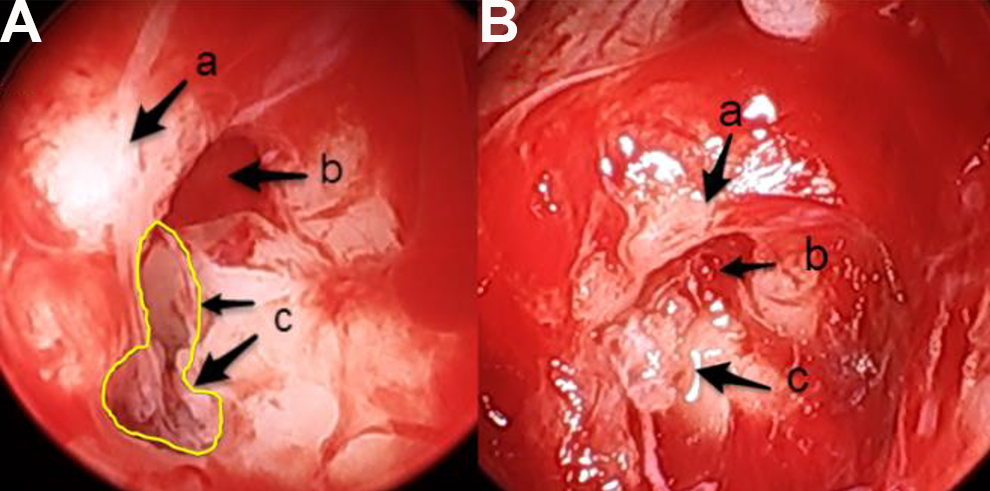
Endoscopic images of the surgical repair of a Hyrtl fissure (HF), left ear. A, (a) round window niche, (b) round window membrane, (c) patent HF (outlined in yellow) emanating cerebrospinal fluid (CSF). Inside the fissure is a remnant stalk of soft tissue which was the fluid-filled sac encountered on myringotomy, thought to be a meningocele. B, View of the fissure after packing with fascia, with resolution of the CSF leak.
General Information
There is a dearth of literature on HF and detailed case series are lacking; only a few authors describe more than one case of HF. 1,6,7 Presentations of HF vary widely. Age at diagnosis was not uniformly provided, but in cases where given, the mean age was 17.2, median age 7.5, and range 0.2 to 70 years (including the ages at death in 3 postmortem studies). Five cases were in adults, while 10 were in children. Age was not stated in another 4 cases. Four cases were in males, 5 were in females, and gender was not stated in 10. Five cases involved left ears, 7 involved right ears, and another 5 cases did not state laterality but were presumably unilateral, while 2 cases were bilateral: overall, 89.5% unilateral versus 10.5% bilateral. Follow-up was only described by Jégoux et al 8 and our case, with no recurrence at the 10-year and 2-year follow-up visits, respectively. Table 1 shows a summary of HF in the literature.
Hearing Loss
Effusion and hearing loss were frequently described, however only Brar et al 9 included full audiometric data. Hearing loss, when present, was noted to range from “mild bilateral hearing loss,” 10 to post-meningitic “bilateral profound sensorineural hearing loss,” 11 Jégoux described a 30 dB conductive hearing loss in the affected ear. 8
Ear Tubes, Otorrhea, and Rhinorrhea
Perhaps most important clinically is that 7 cases involved otorrhea in the setting of ear tube insertion. 6,8 -10,12,13 In 3 of those cases, including our own, there was immediate CSF otorrhea at the time of myringotomy (otorrhea was delayed or timing was not described in the other 3). In one such case of immediate CSF otorrhea, the drainage was addressed with immediate ear tube removal and packing of the EAC with gauze, and at follow-up, there was no further drainage or effusion. 9 These authors postulated that there had been closure of the HF. In the case described by Zakaryan et al, rhinorrhea developed in an adult after removal of an ear tube in an ear that had been draining CSF otorrhea. 10
Cochlear Implantation
Three cases were detected in the setting of cochlear implant planning or placement—2 involved misinsertion. 6,11 Mouzali et al describe the inadvertent insertion of a Med-El Combi electrode array cochlear implant electrode into HF in an 8-year-old boy who had had hearing loss subsequent to viral meningitis. A preoperative CT and magnetic resonance imaging (MRI) had failed to detect the anomaly, but a postoperative CT scan revealed the extracochlear electrode position. It was successfully removed and reinserted, resulting in good function. In one of the cases described by Rich et al, a cochlear implant was placed in a 10-year-old girl; it had to be removed following infection and scalp breakdown. At reimplantation, the original insertion site could not be identified, and the electrode “was placed in what was thought to be an obstructed scala tympani.” The child received no sensation of hearing upon device activation, and a postoperative CT scan demonstrated the electrode in HF. Another case reported by Rich et al involved the identification of an HF on a preoperative CT scan in a child (details in Table 1).
Infectious Complications
Although frequently cited as a potential cause of meningitis, HF was only noted in 3 cases. Rich et al report a case of a 5-year-old boy with purulent otorrhea and pneumococcal meningitis which was treated initially with antibiotics and an ear tube, resulting in persistent clear otorrhea. Two months after meningitis, he underwent exploration, revealing a patent HF which was successfully plugged with muscle. The second case, originally described by Phelps in 1986 and revisited by Rich et al in 2002, was a woman who presented with meningitis and was subsequently found on CT cisternogram to have bilateral petrous pyramid hypoplasia with right HF. The third case of meningitis was in an 8-year old with postlingual deafness described by Mouzali et al.
Imaging/Photographs
Almost all cases described the use of CT of the temporal bone, and in 3 cases, a CT cisternogram was also obtained. 7 Zakaryan et al provide a 3-dimensional reconstruction of the left petrous bone computed tomography. In another 2 cases, an MRI was obtained in addition to the CT scan, although this additional study did not necessarily reveal additional findings. 10,11 In 2 cases, an HF was missed on initial imaging and only identified on later review, including 2 CT scans and an MRI. 8,11 Remenschneider’s series included a representative histopathological image in color, as did Gacek and Leipzig (in black and white). Zakaryan et al offer a schematic representation of the etiopathogenic classification of the cranial CSF leaks. Only the case presented here includes intraoperative photographs.
Associated Clinical History
A few cases were associated with other developmental anomalies and other otologic conditions. The 20-month old in Jégoux’s case report had B-type brachydactyly, and the 7-year-old in Brar et al’s case had bilateral prominauris and right congenital hearing loss. The 3 children in Rich et al’s cases were all candidates for a cochlear implant, indicating significant hearing loss. Another case, by Phelps 14 and later Rich et al 6 (previously mentioned for its presentation with meningitis), included generalized bilateral petrous pyramid hypoplasia with HF on the more affected side. The authors believed that this case represented the persistence of the primitive cochlear aqueduct, which incorporated a patent HF as part of a more generalized failure of petrous apex ossification. 14 In the postmortem histopathologic analyses by Remenschneider et al, an 11-year-old boy died from progressive neurodegenerative disease, although it is unclear the relation this may have had to his HF. The 70-year-old person in Remenschneider’s series had a remote history of a vestibular schwannoma. As mentioned in the introduction, perilabyrinthine defects seem to be associated with other congenital anomalies, frequently fatal within the first year of life. 1
Surgery for HF
Surgical repair of HF is described in 9 cases, including our own. In many cases, there is a paucity of detail; Gacek and Leipzig used “an otological approach” to “excise the meningocele and seal the defect with complete soft tissue obliteration of the middle ear and mastoid cavity.” Meyerhoff and Yellin used a transcanal, tympanomeatal flap with canaloplasty to identify the leak which was then sealed with a tissue graft. 15 Rich et al, 6 in the case of the 5-year-old boy, conducted a “middle ear, mastoid, and attic exploration” and plugged an “obvious leakage” with muscle. Unfortunately, 15 months later, the CSF otorrhea returned. The patient underwent revision surgery aided by intrathecal fluorescein to identify the fissure followed by muscle and bone wax to successfully plug the fissure. This was the only case of revision surgery described. A staged approach was described by Jégoux et al, 8 in which an endaural incision was used. There was a herniation containing CSF, and the incudostapedial joint was separated. Fragments of the herniation sac were removed for histologic analysis, which later demonstrated only respiratory mucosa. Temporalis fascia and a composite mixture of fibrin glue and biphasic calcium phosphate ceramic were used to fill the fistula, and silastic was placed. The silastic was removed 3 months later when an ossicular chain reconstruction was performed. Zakaryan et al 10 described a retrosigmoid approach, after which the defect was closed with bone wax, followed by a free fascial flap and Duraseal (Covidien). In our case, we utilized a postauricular approach through the EAC with endoscopic guidance; a CSF-containing sac was avulsed after it was dissected free from the ossicles, and the fissure was packed with a free fascial graft and bone pate. Finally, Sappington et al 13 was the only author to address the fistula from the medial aspect and utilized a posterior fossa endoscopic technique to “avoid otic capsule removal.”
Interestingly, a CSF-containing sac was described in 3 cases, including our own. Gacek and Leipzig 12 described a meningocele, Jégoux et al 8 described a “herniation containing CSF,” fragments of which were biopsied and found to be negative for meningeal tissue but rather reflected “respiratory mucosa,” In our case, there was a CSF-containing sac seen as well, not sent for pathologic analysis.
Discussion
Hyrtl fissure is the eponym for a tympanomeningeal fissure, which is an embryologic communication between the posterior cranial fossa and the hypotympanum that involutes in normal development. Spector et al published a detailed study of normal development and closure of HF in 1980 after postmortem and histologic analyses of 55 fetuses and neonates ranging in age from 16th week of gestation to 21 days postpartum. 16 During fetal development, the tympanomeningeal fissure runs with the cochlear aqueduct and cochlear vein in the periotic duct, located just medial to the round window niche. 16 Between the 20th and 24th weeks of gestation, there is progressive closure and ossification of this duct until HF is completely obliterated. 6,16 More simply put, in normal development, the bone of the jugular bulb and the cochlea fuse close this embryologic fissure. 2 When they fail to fuse, there is a connection between the hypotympanum and the posterior fossa through an opening in the fossula of the round window niche.
Our ability to draw definitive conclusions about HF is limited due to the small number of cases (n = 19) and heterogeneity of data reported. Presentation occurs more frequently in the pediatric population (66.6% of cases where age was stated, n = 10), mainly unilateral (89.5%, n = 17), and affecting left (5/17) and right ears (7/17) with similar frequency. There was no gender predilection noted (females n = 5, males n = 4, not stated n-10). The most common clinical presentations were CSF otorrhea after tympanostomy tube insertion, followed by cochlear implant failure and incidental imaging findings. Some cases had notably associated otologic and nonotologic conditions, previously discussed and found in Table 1. Three cases involved a history of meningitis. 6,11 In one case, CSF otorrhea seemingly spontaneously resolved after ear tube placement and removal, 9 and in 7 cases, surgery was undertaken to repair the defect.
Surgical approaches and repair methods for HF reported in the literature vary widely. Approaches described included endaural, transcanal, retrosigmoid, postauricular, and posterior fossa endoscopic. It is our opinion that a transcanal middle ear exploration is the most direct way to definitively treat the HF because it enables the surgeon to remove the outpouching and obliterate the fistula with minimal morbidity. Multilayered closure with autologous and synthetic material is generally recommended for CSF leaks which can include bone wax, bone pate, fascia, muscle, and Duraseal (Covidien), and Gelfoam (Pfizer). It is unclear if the sac seen in 3 of the cases within the middle ear space represents an outpouching of middle ear mucosa or a meningocele. It is unclear why a sac appears in some patients with HF and not others, but when present, it should be ligated.
Detection of this rare anomaly requires a high index of suspicion. Both otolaryngologists and radiologists should be familiar with its location and common presentations. Mafee et al recommend that all adults with a persistent middle ear effusion with negative otologic history and normal nasopharyngoscopy undergo a middle ear aspiration for β-2 transferrin (or beta-trace protein) testing. 7 Similarly, children with CSF otorrhea after a myringotomy should also have laboratory testing to assess for CSF, followed by a high-resolution computed tomography (HRCT) scan of the temporal bone. Indeed HRCT is the preferred initial imaging study for all suspected temporal bone CSF leaks. 17 MRI does not appear to play a central role in the diagnosis of HF. Finally, CT cisternography may demonstrate the leak but may be falsely negative if it is intermittent or low flow. 17
Interestingly, recent historical explorations have revealed that the anatomist Joseph Hyrtl (1810-1894) was unlikely to have described the fissure that now bears his name; despite this, the eponym persists. 6,18,19 Both Rich et al 6 and Mudry 19 do an excellent job investigating this point of historical intrigue.
Conclusion
Hyrtl fissure, or tympanomeningeal fissure, is a rare congenital anomaly resulting from incomplete obliteration of a fetal connection between the hypotympanum and posterior fossa. There are 19 cases described in the English language literature. Cerebrospinal fluid otorrhea after a tympanostomy tube and failed cochlear implant are the most common presentations. Further research is clearly required to better characterize the incidence, presentation, and treatment options of this rare, but important, anomaly.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The views stated herein are those of the individual authors and do not represent the views of the Department of Defense or the United States Army.