
Abstract
We report a case of a recurrent hypopharyngeal fistula following spinal hardware placement that required multiple procedures. The course was complicated by a medication error and ultimately the fistula resolved after contralateral pectoralis muscle flap.
A 51-year-old female underwent a 2-level anterior cervical discectomy and fusion and 6 months later developed a neck abscess, salivary fistula draining into the neck, and was found to have a screw placed through the hypopharynx into the hardware" to say: "found to have a mucosal opening with hardware visible in the hypopharynx. She had chronic pain from her spine disease and was on chronic opiates but was otherwise healthy and did not have diabetes.
A washout was performed with primary repair of a small fistula in the hypopharynx and reconstruction with a right sternocleidomastoid (SCM) flap, with placement of Jackson-Pratt (JP) drain and initiation of gastrojejunal (GJ) tube feeds. Six weeks postoperatively, the patient had a recurrence of the salivary fistula and second surgery was performed 4 months after the first. Direct laryngoscopy revealed midline hypopharyngeal perforation measuring about 1 cm in size with the cervical hardware visible. A left transcervical approach was utilized for primary repair of the fistula and placement of the left SCM pedicled muscle flap for coverage of the spinal hardware. However, the patient again developed a recurrence of fistula and abscess about 2 to 3 weeks postoperatively. One month after the third, in which a pectoralis flap was used to replace the prior necrotic SCM flap after debridement. At this time, the patient had a revision of the anterior hardware as it was loose. She had a multilevel corpectomy and a large cage was placed as well as a posterior fusion due to instability. A mucosal defect at the site of the prior repair was visualized and sutured closed through the neck. The left pectoralis flap was rotated inward to completely cover the hardware. Caution was taken to not expose both recurrent laryngeal nerves, so only the left central neck was exposed at this surgery.
Challenging factors for this case also included the patient’s severe malnourishment (body mass index down to 18), severe gastroesophageal reflux despite having a GJ tube, and chronic pain. Accordingly, multiple services were following (head and neck surgery, orthopedics, general surgery, pain medicine, nutrition, and internal medicine). The patient’s neck wound and salivary fistula persisted and her abdominal site where the GJ tube was placed broke down and formed an ulcerated wound larger than 10 cm. After about 30 days of treatment, it was realized that high-dose steroids had been administered from the time of surgery and had not been discontinued. Upon discovery of the error, the steroids were discontinued, risk management was notified, and the patient was immediately approached, and full disclosure of the medication error was made. We discussed the error, how it impacted her care, what options were available, what was being done to manage negative effects, and how this will be prevented in the future.
Two months following the first pectoralis flap, the patient developed another neck abscess and fistula. A fifth surgery was performed which included a neck washout and placement of Penrose drains. Six months after the patient’s initial presentation, she was given hyperbaric oxygen therapy and slow but gradual improvement of the neck was noted.
A swallow study was obtained and although the neck was healed, the spine hardware was in continuity with saliva and corpectomy site (Figure 1). Despite some wound improvement, the neck wound again broke down. A sixth surgery was performed where left neck exploration was done. The left pectoralis muscle was rotated more to create a barrier between the hardware. Importantly, the pectoralis pedicle was not divided. Pectoralis muscle fibers were taken to rotate inward, and no large vessels were seen. Two weeks postoperatively, the pectoralis flap became necrotic and a neck abscess returned.
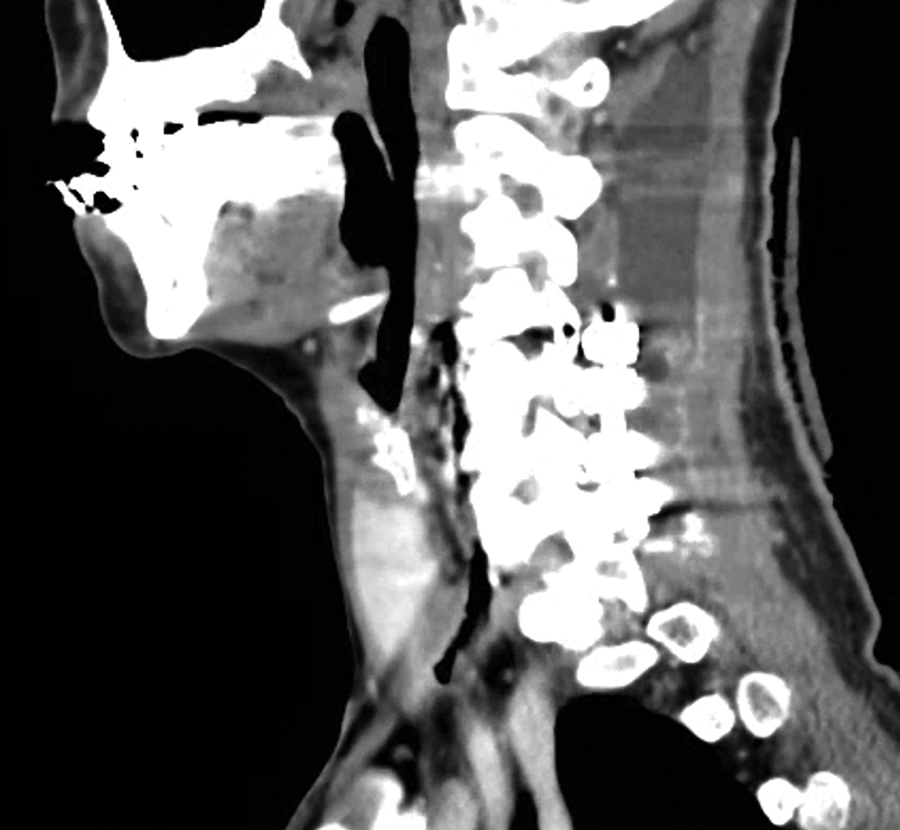
Barium video swallow study demonstrating a persistent communication from the hypopharynx/esophagus to the anterior cervical hardware.
The patient’s seventh surgery occurred 9 months after the initial surgery and included a contralateral pectoralis flap and bilateral neck wound vacuum device. Both sides of the neck were explored, and the contralateral pectoralis flap was flossed completely between the hardware (Figure 2). Wound vacs were placed on both sides.
Fourteen months after the initial surgery, the patient no longer has exposed hardware. The G tube was removed and the patient has full orally intake.
Discussion
Esophageal and hypopharyngeal perforation with anterior cervical spine surgery is uncommon but poses considerable challenges when it occurs. 1 -3 This case is an example of a challenging surgical case that was compounded by a medication error. Medical errors have been reported to be the third leading cause of death in the United States, with a large component related to patient medication. 4 Although the patient in the current report suffered from a complex case involving spinal hardware and saliva, a recurrent abscess, and a persistent fistula, the unnoticed 30-day use of high-dose corticosteroids likely prolonged her course.
Corticosteroid use has been associated with impaired wound healing, 5 which may have played a role in the development of the patient’s persistent fistula—one of a number of potential instances in which the chronic steroid use may have complicated her treatment. A thorough patient history, a detailed look through the patient’s chart, and a more streamlined and effective strategy of communication between the patient’s various teams of care would help avoid this medical error. Additionally, conversations between provider and patient should be documented.
Despite the contemporary prominence of microvascular reconstruction in head and neck surgery, the pectoralis major musculocutaneous flap remains as a commonly used trusted method. The pectoralis muscle flap has a reliable blood supply from the thoracoacromial vessels and can provide a large amount of tissue. 6 Its utilization has been described numerous times in the literature for the purposes of reconstructive surgery of the head and neck. 6 -9 Nevertheless, bilateral pectoralis flaps is an uncommon situation that in this case was encountered due to a unique constellation of circumstances. We think that the first pectoralis muscle flap failed because it did not fully cover the hardware, and was exposed to saliva and infection and revision inset that compromised the blood supply. If the bilateral central neck had been exposed at that time of initial pectoralis flap, the muscle could have been “flossed” behind and draped widely across the hardware. This is the technique that was employed for the contralateral pec flap case (Figure 2) that was ultimately successful.

Contralateral pectoralis muscle flap. The muscle is tunneled posterior to the pharyngoesophageal complex, completely covering the anterior cervical hardware. This coverage was ensured by dissecting both the right and left central neck regions.
An initial surgery was done on the patient’s hostile neck–neck washout with primary repair of a small fistula in the hypopharynx and reconstruction with a left sternocleidomastoid (SCM) flap, with placement of Jackson-Pratt (JP) drain and initiation of gastrojejunal (GJ) tube feeds. Several weeks postoperatively, the patient was seen in office and drain output was minimal. Two weeks later, the patient developed a recurrent salivary fistula draining to the neck. We considered whether the hardware is removed, but this was not feasible due to substantial cervical spine instability. A second surgery was performed. Direct laryngoscopy demonstrated a midline perforation of the hypopharynx with about 1.5cm of hardware visible. From a transcervical exposure, four interrupted 3-0 Vicryl sutures were placed and good closure was observed. The SCM was divided inferiorly and rotated to cover the spine hardware, and a JP drain was placed. Within a few days, the drain output was clearly salivary indicating further fistula. The patient was taken for a third surgery.
The Vicryl sutures were intact from prior repair, but a new 15-mm mucosal hole had formed that was separate from the initial defect, but still in continuity with hardware. The prior SCM flap was not viable and was debrided. Through the neck, the mucosal holes were sutured closed, and a pectoralis flap was used to replace the prior necrotic SCM flap. The left pectoralis flap was rotated inward to completely cover the hardware. Caution was taken to not expose both recurrent laryngeal nerves, so only the left central neck was exposed at this surgery. At this time, the patient had a revision of the anterior hardware as it was loose. She had a multilevel corpectomy and a large cage was placed as well as a posterior fusion due to instability.
Ten days later, the neck had signs of fistula and the incision was explored at the bedside and there appeared to be a fluid collection that was not fully drained so she was taken to the operating room for a washout (fourth surgery). There was no visible mucosal defect and the muscle appeared to be covering the hardware. Challenging factors for this case also included the patient’s severe malnourishment (body mass index down to 18), severe gastroesophageal reflux despite having a GJ tube, and chronic pain. Accordingly, multiple services were following (head and neck surgery, orthopedics, general surgery, pain medicine, nutrition, and internal medicine). The patient’s neck wound and salivary fistula persisted and her abdominal site where the GJ tube was placed broke down and formed an ulcerated wound larger than 10 cm.
After about 30 days of treatment, it was realized that high-dose steroids had been administered from the time of surgery and had not been discontinued. Upon discovery of the error, the steroids were discontinued, risk management was notified, and the patient was immediately approached, and full disclosure of the medication error was made. We discussed the error, how it impacted her care, what options were available, what was being done to manage negative effects, and how this will be prevented in the future. She was treated with a full course of hyperbaric oxygen therapy, her neck healed.
A few months later, a barium swallow study demonstrated that there was still an area of communication between the hypopharynx and the anterior cervical hardware (Figure 1). Shortly thereafter, her left neck incision opened up and started draining purulence, which prompted another admission and return to the operating room for a fifth surgery–left neck exploration, revision inset of the left pectoralis muscle flap, and placement of a negative pressure wound device. The wound vacuum device was used for about one week. Then when seen for a post-operative visit, the left neck wound was open with draining purulence and saliva and there was necrotic pectoralis muscle. The patient was taken for a sixth surgery where the spine and pharynx were dissected from bilateral approaches, and a contralateral pectoralis muscle was placed.
The contralateral pectoralis flap was flossed completely between the hardware (Figure 2). Negative pressure wound devices were placed on both central neck sites. The wound sponges were changed on post-operative day 3, and there was a moderate amount of saliva noted in the wound. The patient was taken for what ended up being her final surgery and there was no clear opening in the mucosa when viewed through the neck, but an endoscopic suture repair was performed in an effort to minimize salivary leakage. A mucosal defect was seen transorally, with healthy visible muscle and no exposed hardware. Endoscopic needle drivers were used through a Dedo laryngoscope, and a barbed running suture was used to close the visible mucosal edges from a transoral approach. Bilateral wound vacuum devices were again used for about 10 days and then the wounds left to heal by secondary intention More than three years after the initial surgery for the hypopharynx fistula, the patient no longer has exposed hardware and is taking full oral diet.
This case highlights the rare risk of esophageal/hypopharyngeal perforation from anterior spine fixation surgery and raises several important surgical considerations. Additional insight can be gained into the occurrence of a medication error and the process implemented in managing it appropriately.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.