
Abstract
The rarity of Melkersson-Rosenthal syndrome, or orofacial granulomatosis, can present with persistent midface bogginess. The management for previous reported cases has included corticosteroid injections, antihistamines, and antibiotics. In the current reported case, the patient was treated with 5-fluorouracil and has been responding positively. Additionally, the patient has not shown signs of steroid atrophy.
Introduction
Chronic orofacial edema can result from a multitude of etiologies, such as those of an infectious, inflammatory, or allergic origin, among others. A proper history intake, as well as thorough physical examination, can inform the clinician both as to the cause and the most appropriate and efficacious management approach.
Case
A 45-year-old male presented with welts under his eyes with associated thickening of the buccal space of 8 months duration (Figure 1). He had no significant past medical history aside from occasional hay fever, had no history of trauma or surgery, and denies any pertinent social or family history. The patient received a Botox injection about 5 years prior and states that there was no concurrent use of dermal fillers. He was previously treated with steroid creams, antibiotics, and oral steroids without any improvement. Magnetic resonance imaging, computed tomography of the sinuses, and chest X-ray were negative, and the patient was referred to facial plastics for surgery.

Welts appearing under the patient’s left eye.
Laboratory tests were collected including C1-esterase inhibitor and serum immunoglobulin E, both of which came back negative. The patient was given a trial with antihistamines, montelukast, and tranexamic acid in case it might be a case of angioedema; however, there was no improvement. The patient was then given a hyaluronidase injection in the event that he may not have been made aware of other treatments during the time of his previous Botox injection. He also demonstrated a negative PPD test. The patient responded to Kenalog steroid injections but had to return every 3 months for repeat injections, and he began to develop steroid atrophy. These treatments totaled to 6 months in duration.
Given the involvement of the buccal space, an anterior buccal biopsy was performed that demonstrated noncaseating granulomas and scattered perivascular inflammatory cells, confirming the diagnosis of orofacial granulomatosis (Figure 2), otherwise known as Melkersson-Rosenthal syndrome. The patient was injected with 5-fluorouracil (5-FU) in the region (0.1-0.5 cc at a concentration of 50 mg/mL), returns to the office every 3 to 4 months for follow-up injections for several years now, and is doing very well. He does not demonstrate steroid atrophy as a result of the 5-FU injections.
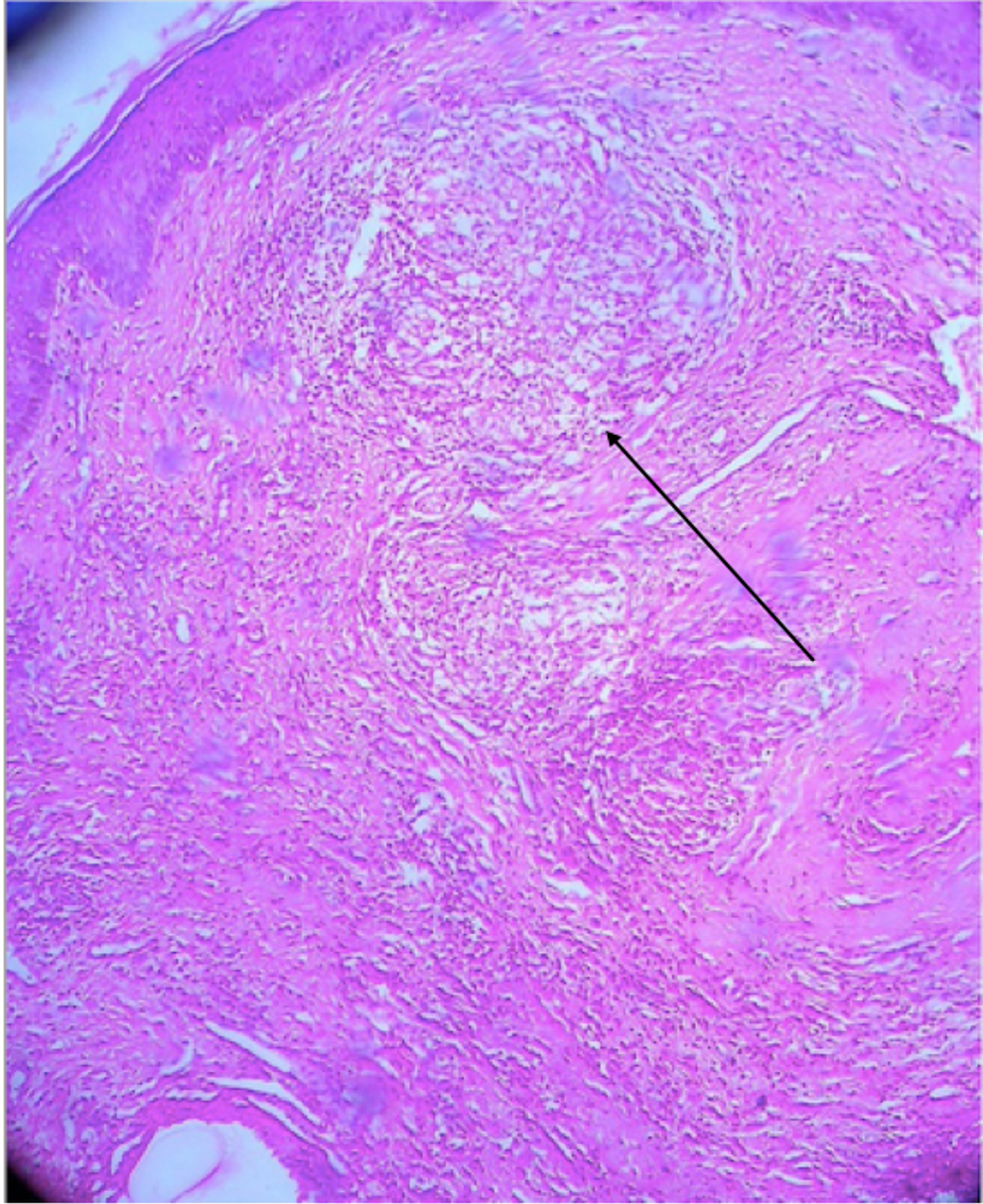
Histopathology of orofacial granulomatosis. Black arrow demonstrates a granuloma.
Discussion
Orofacial granulomatosis is a rare neuromucocutaneous disease that presents as orofacial swelling especially around the lips, facial palsy, and fissured tongue and can be oligosymptomatic or monosymptomatic. The diagnosis is made by exclusion in addition to a positive biopsy for noncaseating granulomas where any additional medical workup for granulomas is negative. 1,2 Treatment is symptomatic and typically local. 3 In the current report, nonstandard options had to be explored as local steroid injections were no longer an option.
The differential diagnosis for Melkersson-Rosenthal syndrome includes persistent hyaluronic acid filler reaction, foreign body reaction, angioneurotic edema especially with monosymptomatic form, amyloidosis, autoimmune vasculitis or Crohn, infections such as Bell’s or orofacial herpes, allergic reactions, or other granulomatous disease. These were all explored.
There is currently no literature on the use of 5-FU for Melkersson-Rosenthal syndrome. This injection is typically performed by facial plastic surgeons and is used for scars and nasal surgery, in addition to many other uses.
Persistent or recurrent facial swelling can be complex to manage. The use of 5-FU is adequate and does not demonstrate steroid side effects such as steroid atrophy or sequelae of systemic steroid absorption. The current report demonstrates that Melkersson-Rosenthal syndrome can be limited.
5-fluorouracil is a chemotherapeutic agent used in the treatment of a multitude of malignancies. Systemic use is indicated in breast carcinomas and gastric, pancreatic, and colorectal adenocarcinomas. Topical use is indicated in several dermatologic conditions such as actinic keratoses and basal cell carcinomas. Other uses include the reduction of keloids and hypertrophic scars. Upon entering cells, 5-FU is converted to fluorodeoxyuridine monophosphate, which complexes with thymidylate synthase to inhibit the production of deoxythymidine monophosphate, a compound essential for DNA replication and repair. 5-fluorouracil also serves as a pyrimidine analog. The result of these mechanisms of action is the death of rapidly proliferating cells. Additionally, the topical use of 5-FU has demonstrated a cytotoxic effect on actinic skin. Common adverse effects of systemic 5-FU treatment include diarrhea, vomiting, nausea, and dehydration, while those of topically applied 5-FU are minimal due to limited absorption. Adverse effects of topical application include localized skin irritation, pruritus, erythema, and eczematous skin reactions. Contraindications include breastfeeding as well as patients deficient in dihydropyrimidine dehydrogenase, an enzyme responsible for 5-FU’s degradation. Patients experiencing severe adverse effects may be administered uridine triacetate orally within 4 days of 5-FU treatment. This mechanism of toxicity reversal supplies a high concentration of uridine, which competes with 5-FU metabolites for binding sites. 4
Footnotes
Authors’ Note
This manuscript is original and has not been submitted elsewhere in part or in whole.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.