
Abstract
Objectives:
To evaluate the therapeutic efficacy of the forced prolonged position (FPP) in patients with horizontal semicircular canal (HSCC) cupulolithiasis in whom the cupulolith repositioning maneuver (CuRM) failed.
Methods:
Fifty-four consecutive patients with HSCC cupulolithiasis were included, and immediate treatment efficacy of CuRM and short-term treatment efficacy of FPP were investigated.
Results:
We performed the CuRM in HSCC cupulolithiasis, and, if the CuRM did not show immediate success, instructed the patients to perform the FPP or the sham position (by random allocation) at home. The immediate therapeutic success of the CuRM was assessed by the absence of nystagmus and vertigo on positional testing after 30 minutes of the maneuver, which was 14.8% on the first visit day. And the resolution rate of HSCC cupulolithiasis was higher in the FPP group than in the sham position group at the second (78.3% vs 55.6%), third (75.0% vs 42.9%), and fourth visits (100% vs 25.0%).
Conclusion:
Although the CuRM has been considered to be a good therapeutic option for HSCC cupulolithiasis because it theoretically aims to detach otoconial particles attached both on the utricle and canal sides of the cupula, the immediate success rate was only 14.8% at the first visit. The FPP can be additionally recommended to improve the resolution rate in HSCC cupulolithiasis patients in whom the CuRM fails.
Keywords
Introduction
Benign paroxysmal positional vertigo (BPPV) involving the horizontal semicircular canal (HSCC) is characterized by positional direction-changing horizontal nystagmus in a supine head-roll test and is known as the second most common type of BPPV. Horizontal semicircular canal BPPV can be divided into 2 variants according to the location of otoconial debris in the canal. Apogeotropic nystagmus, which is generally persistent, is observed when otoconial debris is attached to the HSCC cupula (HSCC cupulolithiasis). For the treatment of HSCC cupulolithiasis, several physical maneuvers, including the barbecue rotation maneuver, 1 therapeutic headshaking in the horizontal plane, 2 the Gufoni maneuver, 3 and the Appiani maneuver, 4 have been introduced. However, these therapeutic maneuvers are sometimes difficult to perform in patients with significant mobility limitations, such as elderly or obese patients. Vannucchi et al proposed the forced prolonged position (FPP) as an effective alternative to treat these patients. 2 Another issue concerning the treatment of HSCC cupulolithiasis is that it is not easy to determine the side of the cupula on which the otoconial debris is attached. However, most liberatory maneuvers attempt to detach otoconial debris from either the utricular side 3 or the canal side 4 of the cupula. To overcome this shortcoming, Kim et al introduced the cupulolith repositioning maneuver (CuRM) with mastoid oscillation to treat otoconial debris on both the utricular and canal sides and reported good treatment efficacy in their retrospective study. 5
Because liberatory maneuvers such as the CuRM are performed at the clinic and the FPP is generally performed at home after instructing the patients to turn their heads in a supine position, it is assumed that the treatment efficacy can benefit from the combination of a liberatory maneuver and the FPP. Furthermore, there has been no study on the immediate treatment efficacy of the CuRM. In this study, we conducted a double-blind, prospective, randomized, controlled study to determine the therapeutic efficacy of the FPP in patients with HSCC cupulolithiasis in whom CuRM treatment failed.
Patients and Methods
Patients
We enrolled 54 consecutive patients diagnosed with HSCC cupulolithiasis at a single dizziness clinic of the tertiary referral center between February 2017 and October 2017. The patients who were included in this study fulfilled the following inclusion criteria: (1) the presence of positional vertigo, (2) apogeotropic positional nystagmus during a supine head-roll test, and (3) the absence of otologic symptoms suggesting other labyrinthine diseases or disorders of the central nervous system. All patients underwent a neuro-otologic examination, including spontaneous and gaze-evoked nystagmus, horizontal and vertical smooth pursuit and saccades, limb ataxia, and balance function, in addition to a routine neurologic examination, which was unremarkable. Patients who received liberatory maneuvers prior to visiting our clinic were also excluded. The purpose and design of the study were thoroughly explained to the patients, and they voluntarily consented to participate. Written informed consent was obtained from all participants, and this study was approved by the institutional review board of Konkuk University Medical Center (KUH-1110064).
Diagnosis of HSCC Cupulolithiasis and the Determination of the Affected Side
A supine head-roll test was performed to diagnose HSCC cupulolithiasis. Apogeotropic nystagmus, which is the typical positional direction-changing horizontal nystagmus beating away from the ground, was observed without fixation using a video Frenzel goggles system. The affected side was determined to show the weaker nystagmus intensity on a supine head-roll test according to Ewald’s second law. When the intensity of nystagmus was similar for both sides on a supine head-roll test, lateralization was determined by the comprehensive interpretation of the nystagmus direction during a bow and lean test in the seated position and that in a supine position. 6,7 Bilateral Dix-Hallpike tests were also performed to exclude vertical canal BPPV. The procedures for positional tests and diagnostic criteria for BPPV followed the guidelines proposed by the American Academy of Otolaryngology–Head and Neck surgery. 8
Applied Maneuvers: CuRM, FPP, and Sham Position
The CuRM was conducted in the same way that was introduced in the original study. 5 Briefly, the patient’s head was turned 135° to the affected side in a supine position, and mastoid oscillation was applied for 30 seconds. Next, the patient’s head was turned 45° to the unaffected side, and the patient’s head was further turned 90° to the unaffected side. Then, the patient’s head was turned 90° to the unaffected side one more time (lateral decubitus to the unaffected side), and mastoid oscillation was applied again. Last, the patient’s head was turned 90° in the same direction (to a prone position), and the patient was slowly brought to a sitting position without neck extension. Each position in the maneuver was maintained for 3 minutes to allow detached otoconial debris to settle.
For the FPP, the patients were advised to turn their heads to the unaffected side in a supine position and stay in this position for approximately 12 hours at home. They were instructed to stay in that position during sleep, and in the event of awakening or getting out of bed, they had to reassume the same position. The rationale for this FPP is that when the patient remains in this position for a long time, the otoconial particles detach from the utricular side of the HSCC cupula by the force of gravity and fall into the utricle. This FPP is different from that of a previous study, 2 in which the patient’s head was turned to the affected side in a supine position to detach otoconial particles from the canal side of the HSCC cupula to fall into a long arm of the HSCC. For the sham position, the patients were advised to turn their heads slightly (usually approximately 30°) to the affected side in a supine position and stay in this position for approximately 12 hours at home. They were instructed to try to stay in that position during sleep by putting another pillows on both sides, and in the event of awakening or getting out of bed, they had to reassume the same position. In the sham position, a long axis of the HSCC cupula of the affected ear is placed in the same direction as gravity. 6 In this position, the gravitational influence on the HSCC cupula, to which otoconial particles are attached, can be minimized. At each follow-up visit, the patients’ compliance was assured by asking if the patients followed the instructions well.
Study Design and Randomization
At the first visit, all patients with HSCC cupulolithiasis were treated with the CuRM. The treatment response was evaluated approximately 30 minutes after the maneuver, and if the first treatment maneuver was unsuccessful, the patient received CuRM treatment one more time. Successful resolution was defined as the absence of positional nystagmus or transformation to geotropic nystagmus. If the second CuRM treatment was also unsuccessful, the patients were, without receiving an additional therapeutic maneuver, randomly assigned to either the FPP or the sham position using a computerized random number function in Microsoft Excel. The patients were blinded to which treatment method they received and scheduled for a follow-up visit. At the second visit, the patients underwent a positional nystagmus test and received the same CuRM if apogeotropic positional nystagmus was observed. If the CuRM was unsuccessful, the patients were instructed to perform the same posttreatment postural restriction as they did before (the FPP or sham position). In this way, the patients were followed up until their fourth visit (Table 1). All diagnostic assessments and therapeutic maneuvers at the initial and follow-up visits were performed by experienced otolaryngologists other than the principal investigator. The principal investigator was blinded to which postural restriction the patient conducted up to the point of data analysis when all of the follow-up evaluations were finished.
Immediate Treatment Success Rate of Cupulolith Repositioning Maneuver (CuRM) and Resolution Rate After Forced Prolonged Position or Sham Maneuver.
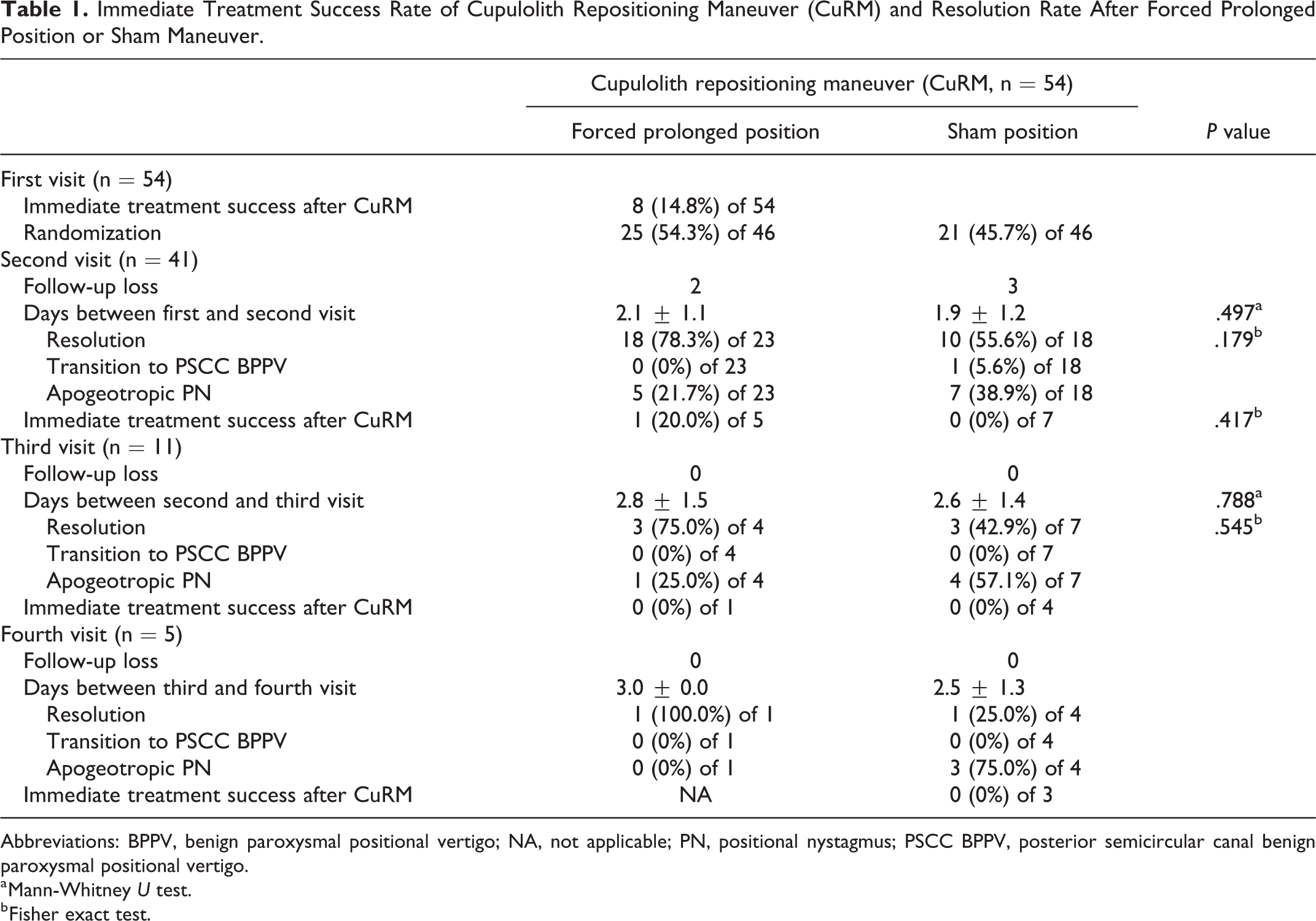
Abbreviations: BPPV, benign paroxysmal positional vertigo; NA, not applicable; PN, positional nystagmus; PSCC BPPV, posterior semicircular canal benign paroxysmal positional vertigo.
a Mann-Whitney U test.
b Fisher exact test.
Statistical Analysis
It was difficult to estimate the exact sample size required in this study because there are no data from studies that adopted the same treatment method as the present study. However, we referred to the results of the previous trials, and the calculation of the sample size was made based on the assumption of a minimum difference of 35% in the primary outcome between the groups (FPP success rate 85% vs sham position success rate 50%), with a power of 80% and significance level of 5%. We calculated that 54 patients (27 per group) were required in this study. Student t test or the Mann-Whitney U test was performed for continuous variables, and the χ2 test or Fisher exact test was performed for categorical variables. SPSS 22.2 for Windows (IBM Corp) was used for analyses. The results were considered statistically significant at P < .05.
Results
Demographic Characteristics
The selected demographic characteristics of the patients are summarized in Table 2. The mean age was 53.0 years in the FPP group, and 55.0 years in the sham position group, which was not significantly different (P = .899, Student t test). The male-female ratio was 4:21 in the FPP group, and 6:15 in the sham position group, which was not significantly different (P = .544, χ2 test). The affected side was the right side in 13 (52%) of 25 patients in the FPP group, and in 11 (52%) of 21 patients in the sham position group, which was not significantly different (P = .979, χ2 test).
Demographic Characteristics.
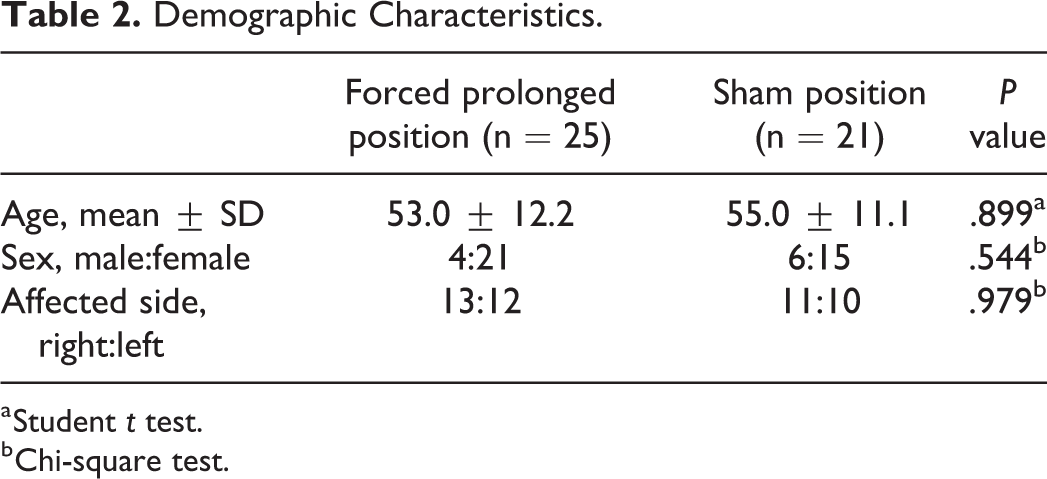
a Student t test.
b Chi-square test.
Immediate Treatment Efficacy of the CuRM and Comparison Between the FPP and the Sham Position
The overall treatment results are shown in Table 1 and Figure 1. In 54 patients with HSCC cupulolithiasis who were treated with the CuRM, the immediate treatment response was successful in 8 patients (Table 1, Figure 1). Forty-six patients in whom CuRM treatment failed were randomly assigned to either the FPP (n = 25) or the sham position group (n = 21). At the second visit, the patients were asked if they followed the instructions of postural restrictions, and the mean period from the first visit to the second visit was 2.1 ± 1.1 days in the FPP group and 1.9 ± 1.2 days in the sham position group, which was not significantly different (P = .497, Mann-Whitney U test). Lost to follow-up occurred in 2 patients in the FPP group and 3 patients in the sham position group (Figure 1). In 23 patients in the FPP group, 18 showed a resolution of HSCC cupulolithiasis, which was defined as the absence of positional nystagmus or the transformation to geotropic nystagmus, and 5 showed apogeotropic positional nystagmus. In 18 patients in the sham position group, 10 showed a resolution of HSCC cupulolithiasis, 1 showed a transition of subtype to posterior semicircular canal (PSCC) BPPV, and 7 showed apogeotropic positional nystagmus. The proportion of patients with a resolution of HSCC cupulolithiasis was higher in the FPP group (18 [78.3%] of 23) than in the sham position group (10 [55.6%] of 18); however, this difference was not significant (P = .179, Fisher exact test). The CuRM was performed in the patients who still showed apogeotropic positional nystagmus, which was successful in 1 (20.0%) of 5 patients in the FPP group and no patient (of 7) in the sham position group (Table 1, Figure 1). At the third visit, the patients were asked if they followed the instructions of postural restrictions, and the mean period from the second visit to the third visit was 2.8 ± 1.5 days in the FPP group and 2.6 ± 1.4 days in the sham position group, which was not significantly different (P = .788, Mann-Whitney U test). No loss to follow-up occurred. In 4 patients in the FPP, 3 showed a resolution of HSCC cupulolithiasis, and 1 showed apogeotropic positional nystagmus. In 7 patients in the sham position group, 3 showed a resolution of HSCC cupulolithiasis and 4 showed apogeotropic positional nystagmus. The proportion of patients with a resolution of HSCC cupulolithiasis was higher in FPP group (3 [75.0%] of 4) than in the sham position group (3 [42.9%] of 7); however, the difference was not significant (P = .545, Fisher exact test). The CuRM was performed in patients who still showed apogeotropic positional nystagmus, which was not successful in any of the patients in the FPP or sham position groups (Table 1, Figure 1). At the fourth visit, the patients were asked if they followed the instructions of postural restrictions, and the mean period from the third visit to the fourth visit was 3.0 days in the FPP group and 2.5 ± 1.3 days in the sham position group. No loss to follow-up occurred. One patient in the FPP group who was followed up showed a resolution of HSCC cupulolithiasis. In 4 patients in the sham position group, 1 showed a resolution of HSCC cupulolithiasis and 3 still showed apogeotropic positional nystagmus. The CuRM was applied in 3 patients with apogeotropic positional nystagmus, which was not successful in any of the patients (Table 1, Figure 1).
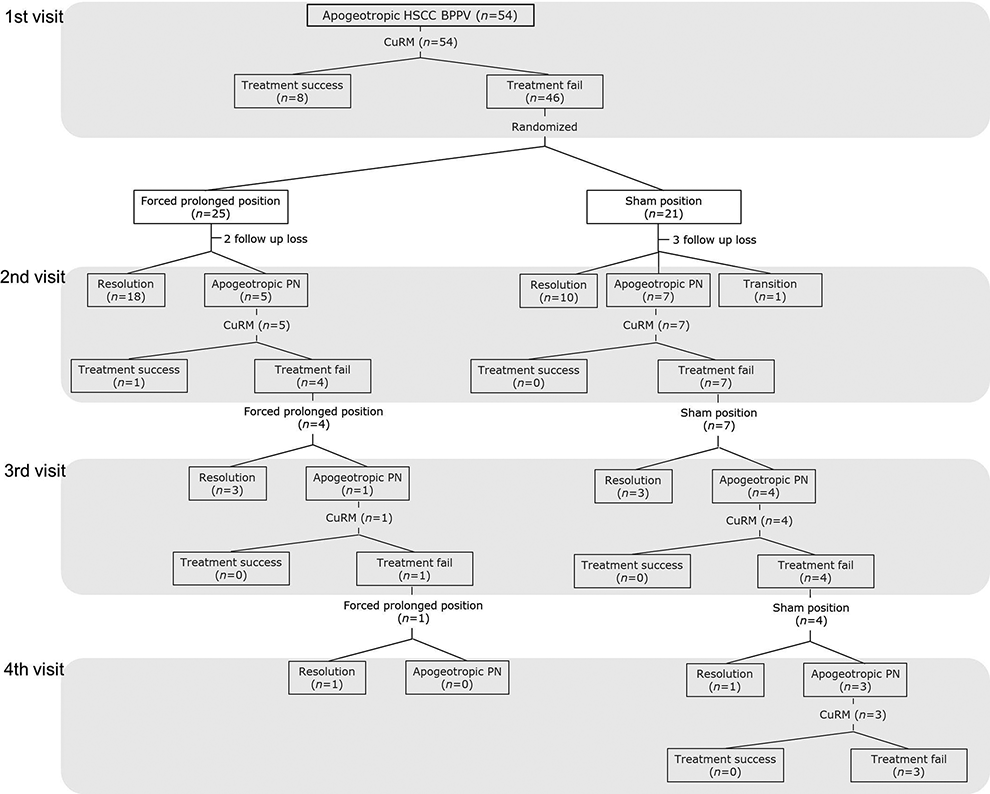
Treatment modality and flowchart for apogeotropic HSCC BPPV. This flowchart illustrates the progression of participants through the trial. CuRM indicates cupulolith repositioning maneuver; HSCC BPPV, horizontal semicircular canal benign paroxysmal positional vertigo; PN, positional nystagmus.
Nystagmus in Patients With a Resolution of Apogeotropic Positional Nystagmus After the FPP or Sham Position
Because the resolution of HSCC cupulolithiasis was defined as the absence of positional nystagmus or transformation to geotropic nystagmus, we examined whether the nystagmus in those patients was absent or geotropic (Table 3). At the second visit, 18 patients showed a resolution of HSCC cupulolithiasis after the FPP, of whom 13 (72.2%) showed no nystagmus and 5 (27.8%) showed geotropic nystagmus, and 10 patients showed a resolution of HSCC cupulolithiasis after the sham position, of whom 6 (60%) showed no nystagmus and 4 (40%) showed geotropic nystagmus. The proportion of patients with no nystagmus was not significantly different between the FPP group and the sham position group (P = .677, Fisher exact test). At the third visit, 3 patients showed a resolution of HSCC cupulolithiasis after the FPP, of whom 2 (66.7%) showed no nystagmus and 1 (33.3%) showed geotropic nystagmus, and 3 patients showed a resolution of HSCC cupulolithiasis after the sham position, of whom 3 (100%) showed no nystagmus and 0 showed geotropic nystagmus. At the fourth visit, 1 patient showed no nystagmus after the FPP, and 1 patient still showed geotropic nystagmus after the sham position. In total, 16 (72.7%) of 22 patients showed no nystagmus after the FPP, and 9 (64.3%) of 14 patients showed no nystagmus after the sham position; the difference between groups was not significant (P = .716, Fisher exact test; Table 3).
Classification of Nystagmus in Patients Showing Resolution of Apogeotropic Positional Nystagmus After Forced Prolonged Position or Sham Position.
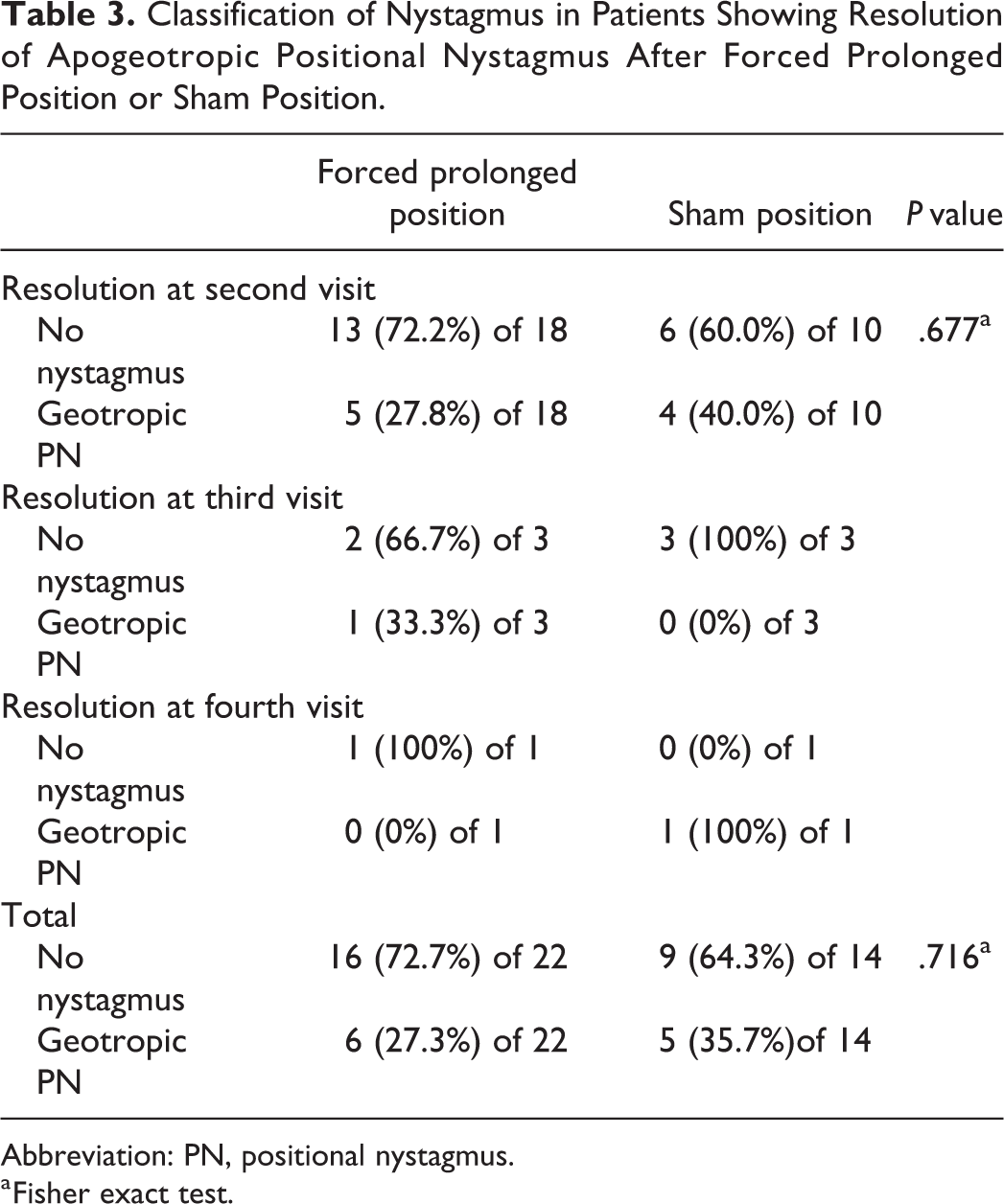
Abbreviation: PN, positional nystagmus.
a Fisher exact test.
Discussion
In general, the success rate of therapeutic maneuvers has been reported to be lower in BPPV involving the HSCC than in the PSCC, probably because the determination of the affected side is more complicated in HSCC BPPV. 9,10 Furthermore, in the case of HSCC cupulolithiasis, it is currently impossible to predict the side (canal or utricular side) on which otoconial particles are attached. The aim of therapeutic maneuvers for HSCC cupulolithiasis is to remove otoconial particles from the anterior arm of the HSCC and detach otoconial particles from the cupula. Otoconial particles attached to the cupula on the canal side can be detached and move toward the utricle through the canal, and those attached to the cupula on the utricle side can move directly to the utricle during the therapeutic maneuver. Several therapeutic maneuvers, such as the barbecue rotation maneuver, therapeutic headshaking in the horizontal plane, the Gufoni maneuver, and the Appiani maneuver, have been introduced to treat HSCC cupulolithiasis. 1 -4,11 -16 While the Gufoni maneuver was found to be the most effective therapeutic maneuver in a meta-analysis of 14 studies, 17 no maneuver was superior to other maneuvers regarding success rate in another study. 18 Recently, therapeutic maneuvers to treat both canalolithiasis in the anterior arm of the HSCC and cupulolithiasis caused by otoconial particles attached to either side of the HSCC cupula have been introduced. 5,19
The CuRM consists of mastoid oscillation and positioning maneuvers and aims to treat both utricular- and canal-sided HSCC cupulolithiasis. 5 Kim et al first introduced the CuRM and reported treatment outcomes of 78 consecutive HSCC cupulolithiasis patients. 5 Although immediate treatment efficacy was not evaluated, 61.5% of patients with HSCC cupulolithiasis resolved after a single maneuver. 6 A recent study reported that the immediate success rate of the CuRM in HSCC cupulolithiasis was 38.9% on the first day, and the resolution rate increased to 88.9% until 1 week even without further CuRM treatment. 20 The FPP was first introduced to treat HSCC canalolithiasis. 2 This maneuver aims to move otoconial particles to the utricle through the canal’s opening only at its nonampullary end using the force of gravity. For this purpose, the patients were instructed to go home, lie on their beds, and turn their heads or whole body from the supine position toward their healthy side, and to stay in this position for approximately 12 hours. After 72 hours, 74.3% of patients with HSCC canalolithiasis were totally symptom-free and did not show any positional nystagmus. 2 A recent study applied the FPP to treat HSCC cupulolithiasis and showed that the cumulative chance of being cured or obtaining a transformation of positional nystagmus to the geotropic form at the 24-hour follow-up was significantly higher in the FPP group than in the sham position group, although the proportion of patients without nystagmus was not different between the groups. 21 The FPP is easily performed at home, especially in severely symptomatic and obese patients or those with restricted neck movement in whom therapeutic maneuvers cannot be safely conducted. 2 However, the FPP can be additionally performed at home after performing therapeutic maneuvers at the clinic in patients with HSCC cupulolithiasis to maximize the treatment efficacy.
In the present study, we performed the CuRM in all patients with HSCC cupulolithiasis at the clinic and instructed the patients in whom CuRM treatment failed to perform the FPP or sham position at home. To our knowledge, this is the first randomized controlled study to compare the therapeutic efficacy of the FPP in HSCC cupulolithiasis patients who were not successfully treated by the CuRM. Several findings should be noted in the present study. First, this study showed that the immediate success rate of the CuRM was 14.8% on the first visit day (Table 1), which was lower than the 38.9% success rate in a previous study. 20 Second, for the FPP, we instructed the patients to turn their heads to the unaffected side in a supine position to move otoconial particles attached on the utricular side of the cupula directly into the utricle, which was different from previous studies 2,21 that instructed the patients to turn their heads to the affected side in a supine position to move otoconial particles attached on the canal side of the cupula into the posterior arm of the canal. The rate of HSCC cupulolithiasis resolution was higher in the FPP group than in the sham position group at the second (78.3% vs 55.6%), third (75.0% vs 42.9%), and fourth visits (100% vs 25.0%, Table 1). Thus, it seems that the FPP contributed to the resolution of HSCC cupulolithiasis, which may imply that otoconial particles are attached on the utricle-sided cupula in at least some of the patients with HSCC cupulolithiasis, as assumed in previous studies. 22,23 In addition, the proportion of patients who showed a transformation of apogeotropic nystagmus to geotropic nystagmus in patients with a resolution of HSCC cupulolithiasis was not different between the FPP group (27.3%) and the sham position group (35.7%, Table 3). On the other hand, in the previous study by Mandalà et al in which the patients’ heads were turned to the affected side in order to move otoconial particles attached on the canal side of the cupula into the posterior arm of the canal, the proportion of patients showing conversion to geotropic variant was significantly higher in the FPP group compared to the sham group. 21 Thus, as shown in the present study, although turning the head to the unaffected side can be more efficient in repositioning the otolith on the utricular side, it may have limitations for repositioning the otolith on the canal side. Further study is needed before a recommendation can be given about which side the FPP should be performed in HSCC cupulolithiasis. Another interesting finding was that the number of patients who showed a resolution of HSCC cupulolithiasis after performing the FPP was higher than that of patients who showed immediate resolution by the CuRM. Moreover, the patients who showed spontaneous resolution after performing the sham position outnumbered the patients who showed resolution immediately after the CuRM, which was similarly observed in a previous study. 20 Although it is difficult to definitely determine whether the CuRM contributed to spontaneous resolution, the previously reported characteristic shortness of the natural course of HSCC cupulolithiasis, which may be associated with postural change during sleep, could have contributed to the resolution. 24,25 Imai et al reported that the average period from the onset to natural remission of positional vertigo in HSCC cupulolithiasis was 13 days and hypothesized that the head movement of daily life makes the otolithic debris fall off the cupula. 25 Shim et al reported that the mean period between the symptom onset and the remission of vertigo was 3.7 days, and the mean period from the initial diagnosis to the disappearance of positional nystagmus in HSCC cupulolithiasis was 4.4 days. 24 They speculated that utricle-side cupulolithiasis, rather than the canal-side cupulolithiasis, is the predominant pathology underlying HSCC cupulolithiasis because the pathway from the utricle side of the cupula to the utricle is much shorter than that from the canal side of the cupula to the utricle. The limitation of the present study is that the difference in treatment efficacy between the FPP and sham group failed to reach statistical significance, though the resolution rate at each follow-up visit was higher in the FPP than sham group (78.3% vs 55.6% at the second visit, 75.0% vs 42.9% at the third visit, and 100% vs 25.0% at the fourth visit). In conclusion, although the CuRM has been considered to be a good therapeutic option for HSCC cupulolithiasis because it theoretically aims to resolve otoconial particles attached both on the utricle and canal sides of the cupula, the immediate success rate was only 14.8% (8 of 54 patients) at the first visit. The FPP can be additionally recommended to improve the resolution rate in HSCC cupulolithiasis patients in whom the CuRM fails.
Conclusion
Although the CuRM has been considered to be a good therapeutic option for HSCC cupulolithiasis because it theoretically aims to resolve otoconial particles attached both on the utricle and canal sides of the cupula, the immediate success rate was only 14.8% (8 of 54 patients) at the first visit. The FPP can be additionally recommended to improve the resolution rate in HSCC cupulolithiasis patients in whom the CuRM fails.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article:This work was supported by Konkuk University Medical Center Research Grant 2020.