
Abstract
Chordomas are rare, malignant bone tumors that arise from embryological remnants of the notochord, typically affecting the skull base, mobile spine, and sacrum with uncommon metastasis to the larynx. Patients with metastasis to the larynx may present with slowly progressive dysphonia and dyspnea. Here, we report an organ-preservation treatment strategy for a patient with widely metastatic extra-axial chordoma presenting with airway compromise who was found to have a new metastasis to the cricoid cartilage.
Clinical Report
An 80-year-old male with a history of metastatic extra-axial chordoma of the proximal tibia, right scapula, and multiple vertebrae with known residual disease despite multimodal therapy presented with 3 months of worsening dysphonia and dyspnea. Flexible fiberoptic laryngoscopy performed in the clinic was notable for narrowing of the glottic inlet and subglottic airway along with left vocal fold paralysis (Figure 1A).
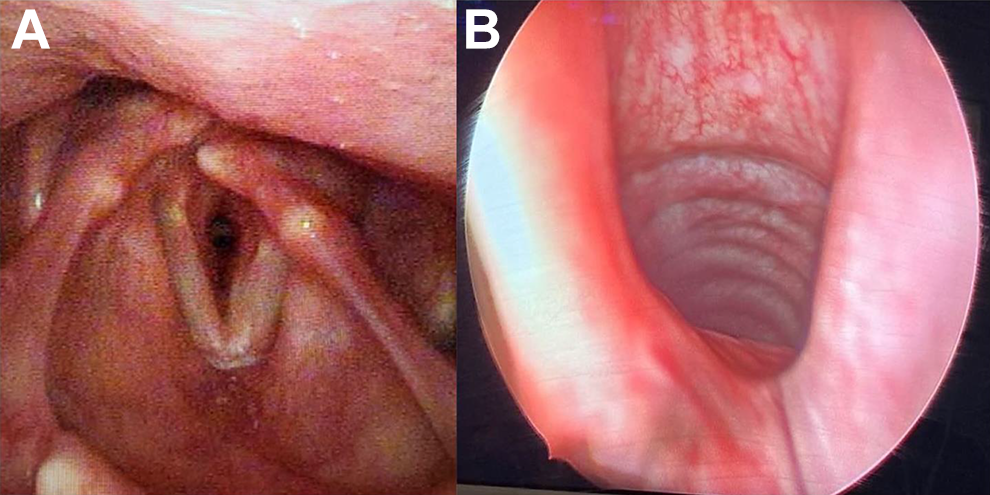
(A) Preoperative flexible fiberoptic laryngoscopy demonstrating subglottic fullness and left vocal cord in paramedian position. (B) Direct laryngoscopy performed during initial resection demonstrating posterior subglottic fullness and asymmetry.
Computed tomography (CT) scan was performed, which revealed an expansive mass of the posterior cricoid cartilage with mass effect on the larynx. Given his known diagnosis of chordoma, this was suspicious for metastatic chordoma, although another cartilaginous tumor such as chondroma or chondrosarcoma could not be ruled out (Figure 2A).
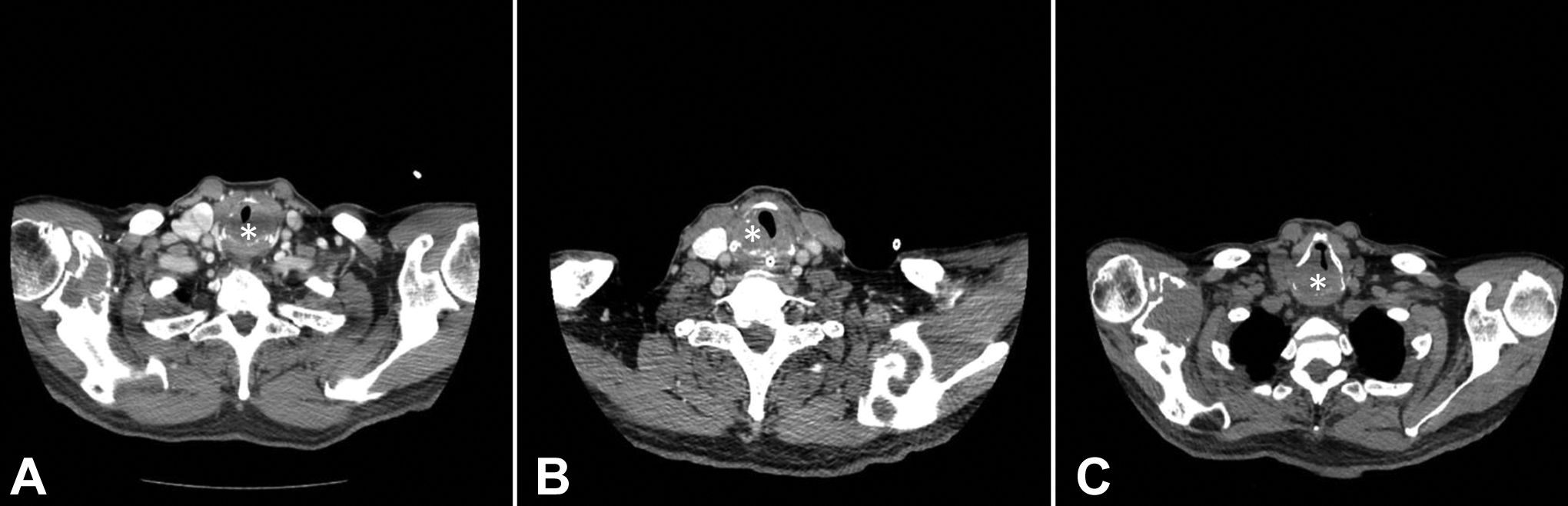
(A) Initial computed tomography (CT) scan performed prior to first debulking procedure shows an expansive mass (identified with the star) of the cricoid cartilage with associated narrowing of the airway. (B) CT scan performed 1 month after initial debulking procedure demonstrates known residual tumor (star) and an improved airway opening compared to preoperative CT. (C) CT scan performed at 9-month follow-up prior to second debulking procedure demonstrates significant tumor regrowth (star) and airway narrowing.
The mass had destroyed and expanded a significant portion of the posterior cricoid lamina and would traditionally require a total laryngectomy for complete resection. After discussion with the patient, given his age and treatment goals, the decision was made to pursue organ-preserving surgery with the understanding that some residual tumor would remain, and regrowth was possible.
Intraoperatively, direct laryngoscopy revealed significant subglottic airway narrowing (Figure 1B). An extensive subtotal enucleation was performed via left lateral laryngotomy. The gelatinous mass was dissected away from the posterior lamina, leaving some residual cartilage on the right, and preserving the cricoarytenoid muscles bilaterally. Due to anticipated postoperative laryngeal edema, a concurrent tracheotomy was performed. Surgical pathology noted polygonal cells with eosinophilic cytoplasm and vacuoles set in a myxoid stroma, diagnostic of metastatic chordoma (Figure 3).
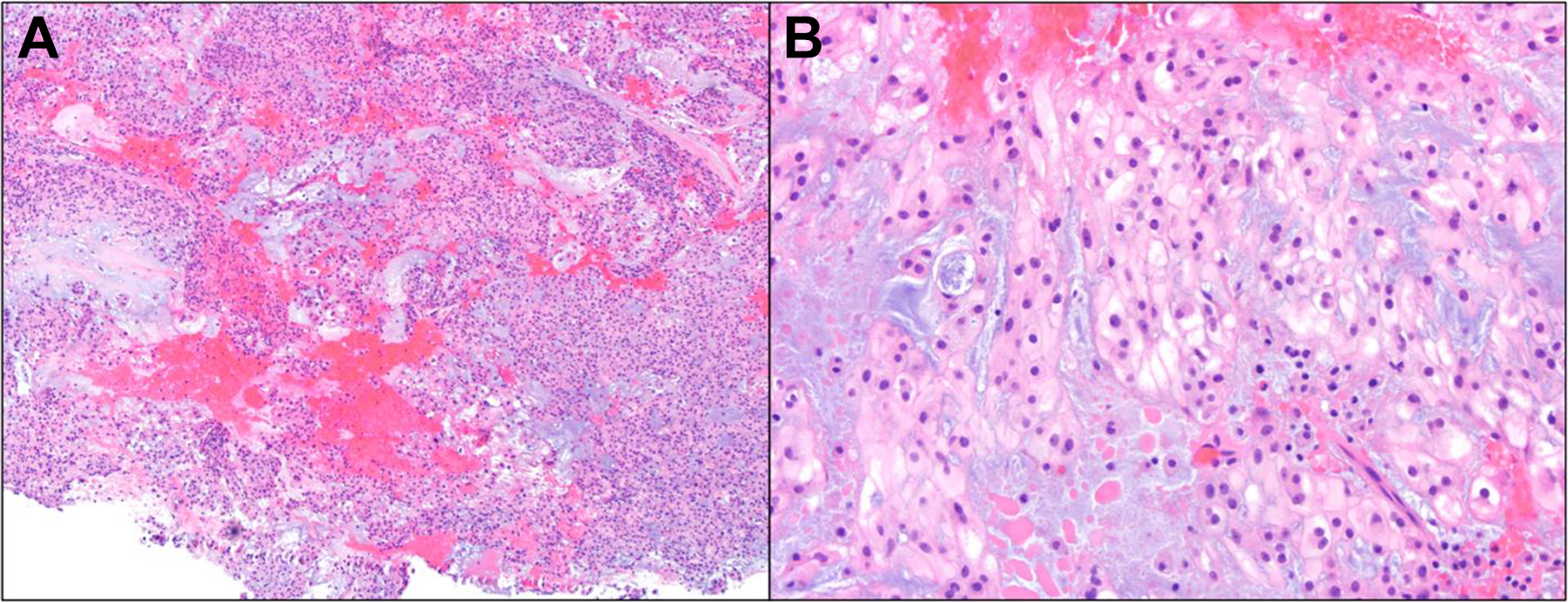
Hematoxylin and eosin (H&E) stained histological sections of tumor (A) low-power magnification shows fragments of tumor consisting of sheets and cords of polygonal tumor cells in a myxoid matrix (4× magnification). (B) High-power magnification shows polygonal tumor cells with round nuclei, prominent nucleoli, and abundant cytoplasm that ranges from eosinophilic to clear and vacuolated (20× magnification).
The patient was successfully decannulated one-month postoperatively, and a CT scan performed at that time showed an improved patent airway and expected residual tumor (Figure 2B). At his 3- and 6-month follow-up appointments, he reported adequate swallowing, voice, and respiratory function. At his 9-month follow-up visit, he reported shortness of breath on exertion and was noted to again have airway narrowing on flexible fiberoptic laryngoscopy; CT scan demonstrated tumor regrowth (Figure 2C). He underwent a second tumor debulking procedure approximately one year after the initial procedure, again via left lateral laryngotomy with resection of approximately 90% of the tumor. Both posterior cricoarytenoid muscles were preserved, and the patient was felt to have adequate arytenoid function bilaterally. He again underwent tracheostomy for postoperative edema. At his most recent follow-up visit, he reported good swallowing, voice, and respiratory functions with formalized tracheotomy in place.
Here, we report a unique case of a patient with an obstructive posterior laryngeal chordoma who underwent serial debulking and tracheotomy. Extra-axial chordoma metastatic to the larynx is a rare disease; to our knowledge, there is only one prior case report in the literature. 1 Conversely, more common primary malignancies of the larynx include squamous cell carcinoma, adenocarcinoma, or low-grade cartilaginous tumors such as chondroma or chondrosarcoma. 2,3 Metastatic lesions to the larynx are even more uncommon and primarily affect the supraglottis, while the glottis is the least common site. 3,4 Obtaining a detailed clinical history and radiographic imaging is crucial to narrowing the differential, as in this patient. Directed tissue diagnosis obtained via surgical resection or debulking and review by an experienced pathologist is often required for diagnosis and appropriate treatment choice and patient counseling.
As with any airway-related disease, treatment begins with prompt identification and management of any impending airway compromise. In this patient, with symptoms of chronic dyspnea and subglottic narrowing, initial decision-making centered around the preservation of a patent airway. Although total laryngectomy would be the definitive surgical treatment for this type of laryngeal tumor, 1,5 we elected for a more conservative approach given the patient’s age, preferences, and the slow-growing nature of the tumor. The possibility of preserving voice and swallow should be carefully considered depending on an individual patient’s goals. Tumor debulking can be very helpful in alleviating the symptoms of mass effect, but ultimately tracheotomy may be necessary to maintain a safe airway. Close clinical follow-up is necessary due to the high risk of long-term local regrowth or recurrence, and many of these patients will require repeat debulking procedures.
Footnotes
Authors’ Note
American Laryngological Association (ALA)/Combined Otolaryngology Spring Meetings; April 7-8, 2021.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.