
Abstract
Objectives:
To compare subjective voice outcomes and postoperative laryngoscopic examination findings of patients with subjective voice complaints between surgeon-monitored and certified technician–monitored thyroidectomies.
Methods:
Patients who underwent hemithyroidectomy, total thyroidectomy, and completion thyroidectomy using a nerve monitoring system between November 2015 and June 2018 were included in the study. Retrospective chart review was carried out to assess how often patients reported voice changes and to record postoperative flexible laryngoscopic findings of patients when that examination was performed. Data were analyzed using the χ2 test to identify significant differences in outcomes for the 2 groups.
Results:
A total of 293 procedures was performed among 3 surgeons. Surgeons monitored the nerves in 147 cases and a certified technician monitored the nerves in 146 cases. Subjective voice changes were identified in 11 (7.48%) cases in the surgeon-monitored group and in 20 (13.70%) cases in the technician-monitored group (P = .084). Among the patients who expressed subjective voice changes, 7 patients were identified with vocal cord hypomobility or immobility in the surgeon-monitored group and 13 patients had an abnormal examination in the technician-monitored group (P = .234).
Conclusions:
Subjective voice changes or proven vocal cord mobility problems were not different between surgeon-monitored patients and technician-monitored patients in thyroidectomies.
Introduction
Nerve monitoring in thyroidectomy has been in use among otolaryngologists for many years as a tool to reduce the incidence of injury to the recurrent laryngeal nerve (RLN) during thyroid surgery, 1,2 and its use has grown significantly in the United States. 3 Despite its growing popularity and long history as an adjunct to thyroidectomy, it remains uncertain whether nerve monitoring offers superior protection against nerve injury to relying on direct visualization of the nerve alone. 1 What is certain is that the use of nerve monitoring is increasing not only in the United States but in Europe, Asia, Africa, and abroad. 3 In order to further reduce the incidence of injury to the RLN, some surgeons have adopted the practice of adding a technician trained in cranial nerve monitoring in the operating room to monitor the nerve alongside the surgeon. 4 This study aims to determine whether this additional intervention has an effect on postoperative voice changes solely reported by patients undergoing thyroidectomy.
Patients and Methods
The primary variable under study was whether the intra-operative nerve monitoring (IONM) was performed by a technician or by the surgeon. A retrospective chart review was conducted for patients who underwent hemithyroidectomy, total thyroidectomy, and completion thyroidectomy using the NIM 3.0 system (Medtronic Xomed, Inc) with or without the presence of a certified nerve monitoring technician, between November 2015 and June 2018 in a tertiary academic center following institutional review board approval (228227). Patients undergoing surgeries coded according to Table 1 are included, and outcomes were determined from a careful review of operative and postoperative clinical notes. Significant outcomes were recorded as no adverse outcome, voice change including hoarseness, or RLN injury. Recurrent laryngeal nerve injury was either determined from the operative report where intraoperative RLN injury was recognized and documented or from the postoperative visit note where direct visualization of an immobilized vocal cord was documented with flexible laryngoscopy in a patient who complained of any voice changes. Information on patient demographics and indication for surgery were also collected.
CPT Codes and Procedures by Name.
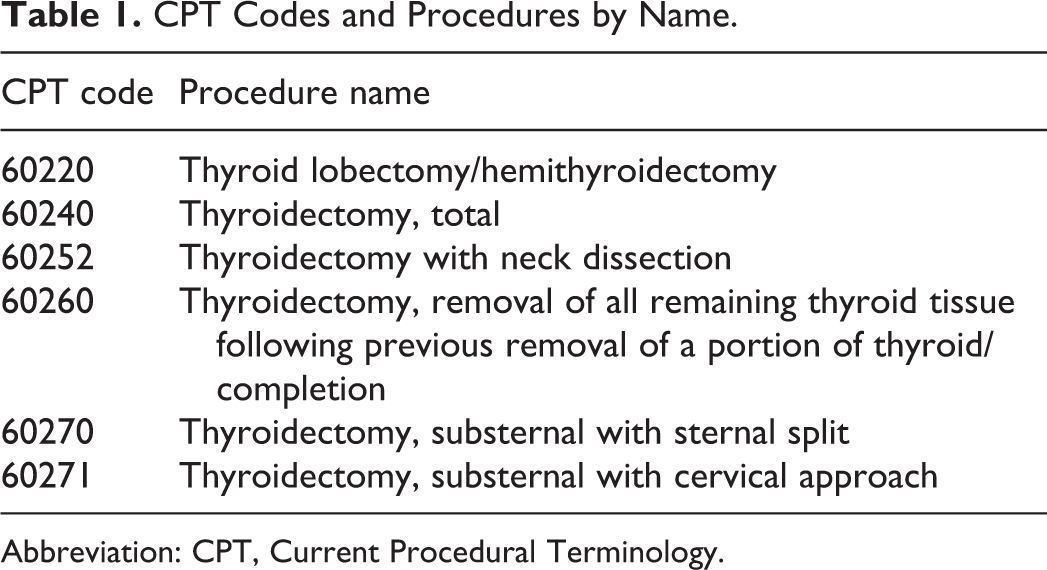
Abbreviation: CPT, Current Procedural Terminology.
Data were analyzed using the χ2 test to identify significant differences in outcomes for the 2 groups. Confounders in the data include variability of patient follow-up, use of subjective criteria, and patient refusal of confirmatory flexible laryngoscopy. Each surgeon scoped their own patients following surgery if indicated, and standard follow-up at the institution includes a postop visit at 2 weeks, another in 3 months if voice changes are noted, and a final appointment at 6 months to discuss therapeutic options. Patient records were reviewed until a change was shown to be sustained or resolved whenever possible. Patients were considered “lost to follow-up” if they did not keep a scheduled appointment during the postop monitoring period.
Results
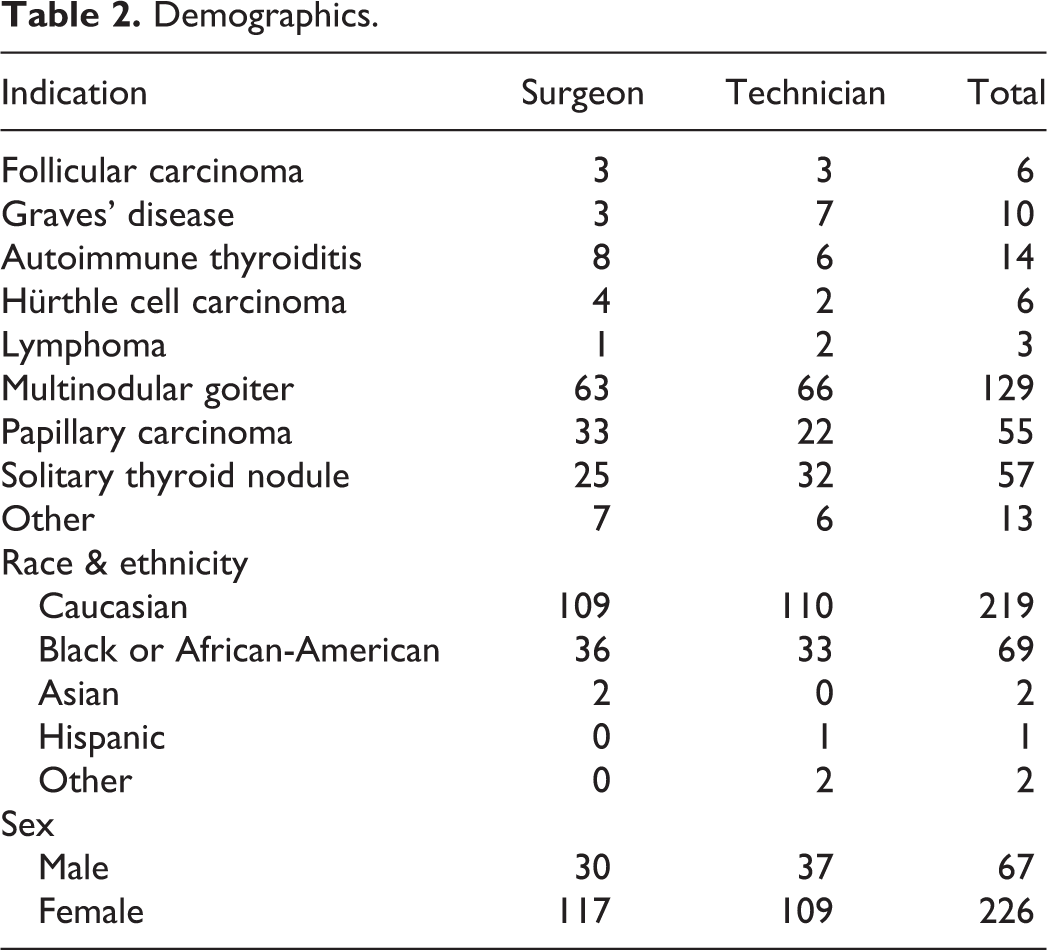
There were no significant differences between the groups in composition or outcomes according to indication for surgery (P = .887), race and ethnicity (P = .819), or gender (P = .968), summarized in Table 2.
Demographics.
In the surgeon-monitored group, 11 patients reported altered voice, 8 of whom were evaluated with laryngoscopy. Of the 8 patients who underwent laryngoscopy, 7 had abnormal vocal cord mobility and 1 had a normal examination. Three patients who reported voice changes declined a scope procedure. In the technician-monitored group, 20 patients reported altered voice, with 14 of those undergoing laryngoscopy to examine vocal cord mobility. Thirteen patients had an abnormal examination, 1 had a normal examination, and 6 patients declined the scope, 1 of whom was subsequently lost to follow-up after their initial postop visit. These results are summarized in Table 3.
Subjective Findings and Scope Results by Group.
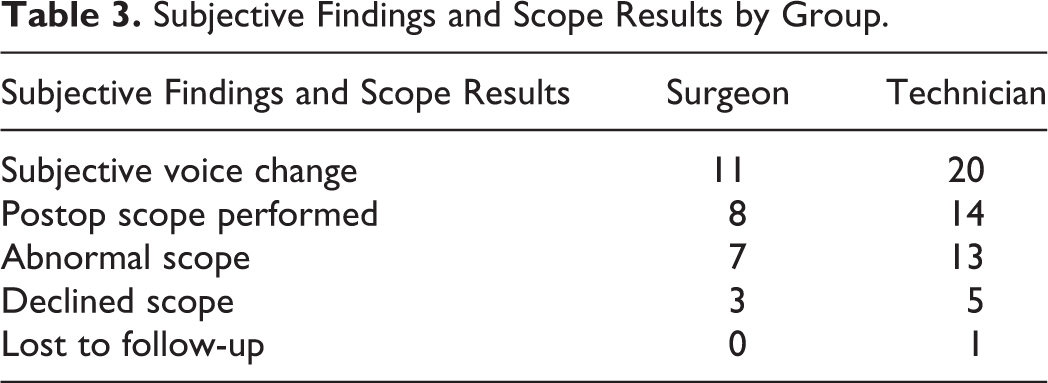
In this cohort, patient-reported postoperative voice changes or proven vocal cord mobility problems were not different between surgeon-monitored patients and technician-monitored patients in thyroidectomies (P = .084). Of note, in this study, a subjective complaint of voice change was a strong indicator of RLN injury as only 2 patients of 22 had normal scope examinations.
Discussion
One of the most feared complications of thyroidectomy is an injury to the RLN. A systematic review conducted in 2006, which included over 25 000 patients, found that the average incidence of temporary RLN injury was 9.8% and the incidence of permanent RLN injury was 2.3%. 5 Despite the low incidence of the complication, it accounted for 43% of the claims examined by Singer et al in a study published in 2011 that evaluated the characteristics of claims brought against surgeons performing thyroidectomy from 1985 to 2008. That 43% represents 55 of 127 claims, and 21 of those 55 resulted in indemnity payments. 6 Injury to the RLN may not happen often, but it represents a large proportion of the claims filed against surgeons for malpractice, and a high percentage of those claims are paid out.
IONM was introduced in the 1970s as a tool to reduce the incidence of injury to the RLN. 7 Since then many surgeons have introduced the technology into their practices. 8 Surgeons have been surveyed multiple times regarding their use of the tool, and overall trends show increasing adoption. The first survey was published in 2007, and it was sent to a random selection of half of all otolaryngologists in the United States. That survey had a response rate of 40.7%, and it revealed that 28.6% of all respondents who used IONM in thyroid surgery did so in all cases. 9 Subsequent surveys published in 2009, 2012, 2013, 2016, 2019, and 2020 10 -14 show increasing rates of adoption overall among various surgeons who perform thyroidectomy but also increasing rates of routine use. Results of a global survey published by Feng et al in 2019 investigating usage patterns of IONM revealed that 65% of respondents answered that they use the technology, while 18% reported that they use it selectively. 3 The 2020 survey published by Ritter et al of members of the American Head and Neck Society found that 72% of all respondents used IONM routinely, with 21% using it selectively. 14 Reducing morbidity associated with RLN injury is the main goal of this adjunct, but evidence supporting its superiority over direct visualization for protection of the nerve is lacking. 3
Many studies have been undertaken to ascertain whether IONM reduces the incidence of injury when compared with visual identification alone, and the results are inconclusive. A meta-analysis of the quality of systematic reviews on this subject published by Sanabria et al in 2019 revealed that the quality of 13 studies evaluating the use of IONM over visualization is low. 2 Of note, the results of those studies were mixed, with some showing significant benefit and others showing none. An earlier study published by Sanabria et al in 2013 reviewed 6 studies reporting the results of randomized controlled trials (RCTs), and the authors noted several problems with the quality of RCTs evaluating the effectiveness of IONM as well. That systematic review’s pooled patient population was 1602, and the authors calculated that, given the low incidence of even temporary paralysis, the results of about 4500 patients would need to be studied in order to have sufficient power. The authors further concluded that, even with power, the overall value of the risk distribution is not likely to change. 1
If the use of the monitor by the surgeon alone seems not to lower the risk of permanent injury, perhaps adding a certified cranial nerve monitoring technician, whose expertise is the function and use of the monitoring technology, would help drive down the incidence of permanent injury. At our institution, the monitoring technician helps the surgeon determine whether the bedside probe is registering signal correctly, or if there is some element of artifact from instruments in the field. They also help troubleshoot loss or weakening of signal, which can sometimes occur due to traction on the nerve itself. Finally, the technician is able to document the use of the NIM system, which will be explained in greater detail below. The use of the monitor alone is more expensive, but the cost rises further when the surgeon opts to have a specially trained technician monitor the system during surgery. Nevertheless, this expense may be acceptable if it leads to a significant decrease in morbidity.
An extensive search of currently available literature failed to reveal any study in any surgical subspecialty that evaluated outcomes between surgeons alone and surgeons assisted by technician. The use of technicians and MDs experienced in nerve monitoring has been discussed and advocated in various surgeries but not necessarily studied with regard to outcomes between the 2 groups. 15 -17 A few articles have been written that assess outcomes in spine surgery, parotid surgery, and parathyroid surgery that discuss results of either MDs monitoring alone 18 or in conjunction with a technician, 4,19-20 but none that assesses both in the same study. A Canadian study evaluating surgeon-monitored cases in Canada noted that it can be difficult to find trained technicians, and they studied the safety of surgeon-monitored cases to determine whether it can be done in the absence of a technician. 20
In this study, no significant difference in patient-reported voice changes was found between the groups monitored by a technician versus those monitored by the surgeon alone. Another concern addressed by having a technician present in the room is documentation of the procedure. When the surgeon alone monitors the system, no one is at the terminal to save readings or ensure that the intraoperative findings are preserved in the patient record. The technician does perform this work, which functions both as a visual aid to the patient and as evidence of nerve preservation or loss should legal action be taken. Between 1989 and 2009, the use of IONM during thyroid surgery was not mentioned in any state or federal malpractice cases that went to court. 21 Yet in Germany, IONM is beginning to be used by defendants as well as plaintiffs to argue cases. 22 Therefore, its use is likely to be an important factor with regard to medicolegal aspects of thyroid surgery in the future.
With the growing cost of health care and surgical procedures, it is important to be conscious of what is essential in the operating room. When possible, any added cost without added patient benefit should be eliminated. Better financial stewardship is critical to reducing the cost of health care and improving patient satisfaction.
There are inherent limitations of our current retrospective study. Some patients did not return to the clinic after their 2-week postoperative visit, and so some who noted voice changes at 2 weeks may have had their complaints resolve, but the record was never updated as they did not return for follow-up. Another limitation of the study is the subjective nature of voice change as an outcome. Patient-reported voice changes were ascertained from clinic notes rather than from validated surveys or questionnaires, and the only objective measure of hoarseness was whether paralysis was confirmed by flexible laryngoscopy, which was not routinely performed in all patients. In this cohort, clinicians followed the guidance provided by the American Academy of Otolaryngology for managing voice outcomes, 23 taking care to note changes in the voice reported by the patient between 2 weeks and 2 months from surgery. American Academy of Otolaryngology recommends laryngoscopy only when the patient notes a change in the voice, not as a routine postoperative measure. 23 The sample size is also small, and only 1 of the 3 treating surgeons routinely used technicians in surgery. Voice changes of any kind were included in this study, so these data may also capture injuries to the superior laryngeal nerve, which is not monitored by the NIMS IONM. These considerations aside, the results may provide some evidence that adding a technician to monitor alongside the surgeon did not improve voice outcomes for patients in this cohort.
A prospective study with a larger sample would provide more definitive evidence, and with all patients having vocal cord function confirmed by preoperative and postoperative testing for both groups under study. Comprehensive testing would include flexible laryngoscopy, baseline and postoperative voice acoustic measures, and a validated subjective questionnaire such as the Voice Handicap Index. Whether the surgeries that had nerve signals recorded by technicians resulted in fewer claims, or fewer findings in favor of the patient was not studied, but it may also influence a practitioner’s decision regarding the incorporation of a technician into the surgical team.
Conclusion
Subjective voice changes or proven vocal cord mobility problems were not different between surgeon-monitored patients and technician-monitored patients in thyroidectomies in this study. Although adding the technician to the surgical team may provide other benefits, particularly to high-volume endocrine surgeons who want to record the performance of the instrument in the patient electronic health record, this practice is not demonstrated to be of direct benefit to the patient at this time.
Footnotes
Authors’ Note
Misty Tolbert, BS, RPSGT; Ginger J. Brown, MS, RPSGT; Veronica Williford, RN, CMT.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.