
Abstract
Significance Statement
Granulomatosis with polyangitis (GPA) is a systemic necrotizing vasculitis comprising of inflammation of small and medium-sized vessels. 1 It typically presents with involvement of the upper and lower airways as well as the kidneys. If left untreated, end-organ damage may occur. Hematological investigations typically demonstrate the presence of antinuclear cytoplasmic antibodies (ANCA). 2 Here, we discuss an unusual presentation of ANCA negative GPA, presenting initially with nasal symptoms.
Case Report
A previously fit and well 48-year-old construction worker presented to the ear nose and throat clinic with a 5-month history of unilateral nasal discharge and a sensation of pressure around the maxillary sinus. Nasendoscopic examination demonstrated extensive crusting of the left nasal cavity. On obtaining further imaging, computed tomography (CT) and magnetic resonance imaging (MRI) scans revealed irregular mucosa and crusting within the left nasal cavity, as well as pansinusitis. There was no bony erosion noted. Subsequent examination under anesthetic (EUA) was performed, which demonstrated significant crusting, granulomatous-looking mucosa throughout the left nasal cavity and an ulcerated area around the middle meatus (see Figure 1). Multiple biopsies were taken which reported chronic inflammation but no evidence of granulomatous inflammation, vasculitis, or neoplasia.
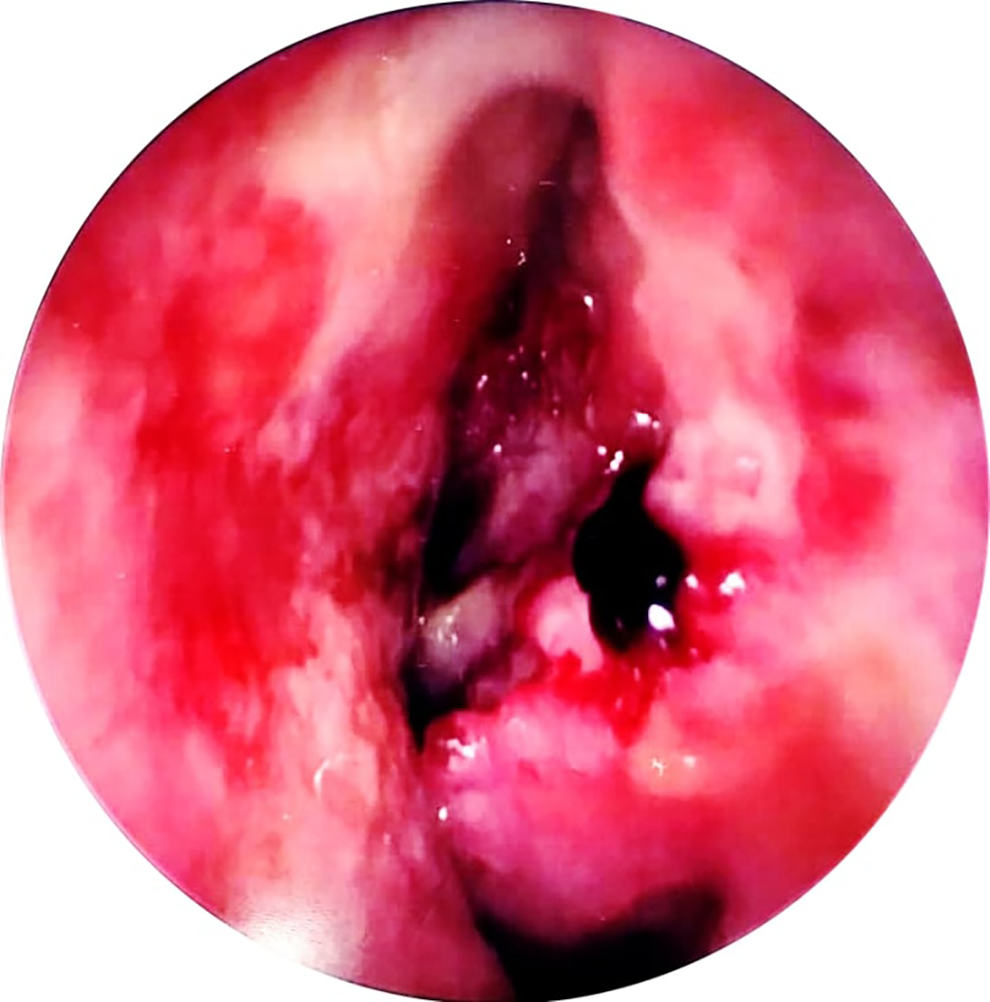
Appearance of the left middle meatus at the initial EUA.
Following these results, medical therapy comprising of a nasal steroid sprays, saline douches, and a 2-month course of oral antibiotics were commenced.
After 2 months of medical therapy, there had been no improvement in symptoms and the nasendoscopic appearance remained unaltered. A repeat CT scan revealed similar irregular mucosal with a new erosion of the left lamina papyracea. Blood tests for c-ANCA and p-ANCA were negative. Repeated EUA and multiple biopsies on this further occasion demonstrated no evidence of granulomatous inflammation, vasculitis, or dysplasia.
Subsequent development of left infraorbital numbness, weakness of the left lateral rectus muscle, a red-eye, and epididymitis associated with significant malaise prompted a further urgent MRI scan and EUA with biopsy as well as referral to the rheumatology team. At this point, the MRI and the EUA demonstrated destruction of the septal cartilage as well as the medial wall of both maxillary sinuses and parts of the inferior and middle turbinates (see Figure 2). There was also soft tissue extending from the ethmoid sinuses into the extraconal compartments of both orbits (see Figure 3).
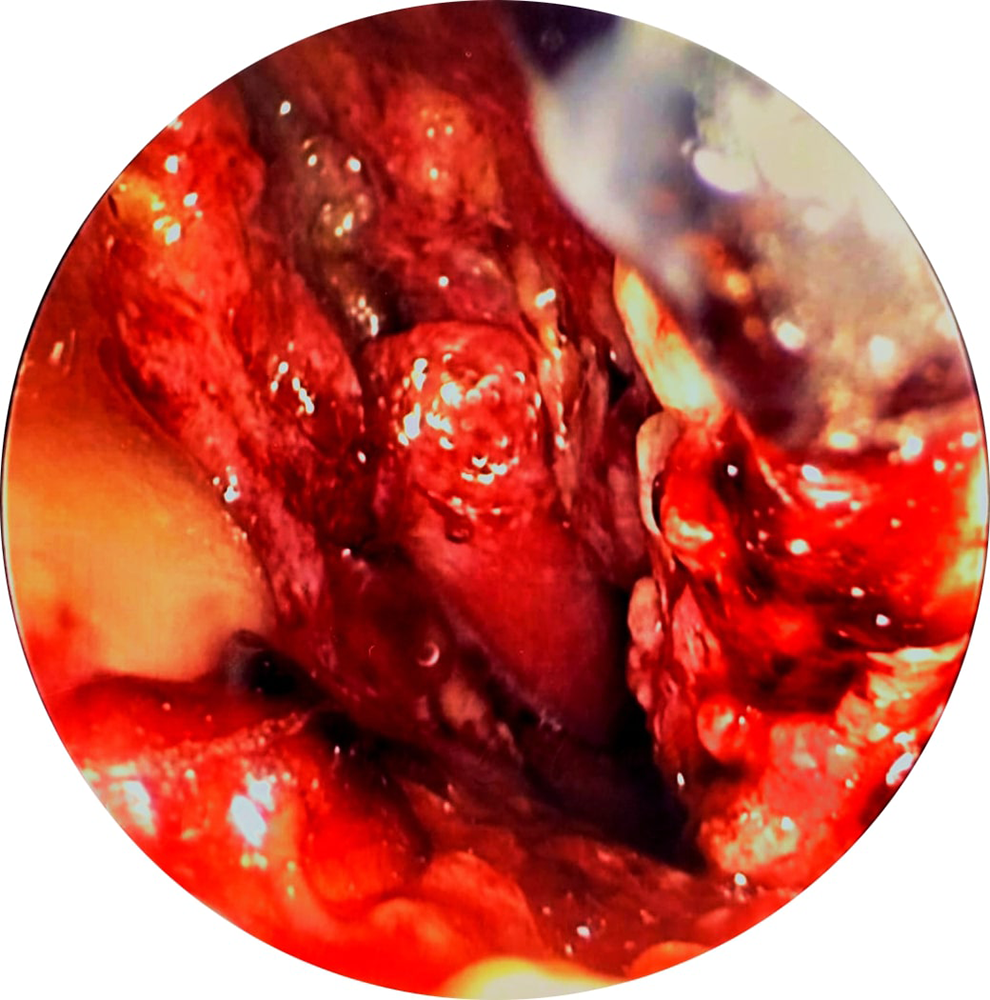
Appearance of the nasal cavity at third EUA.
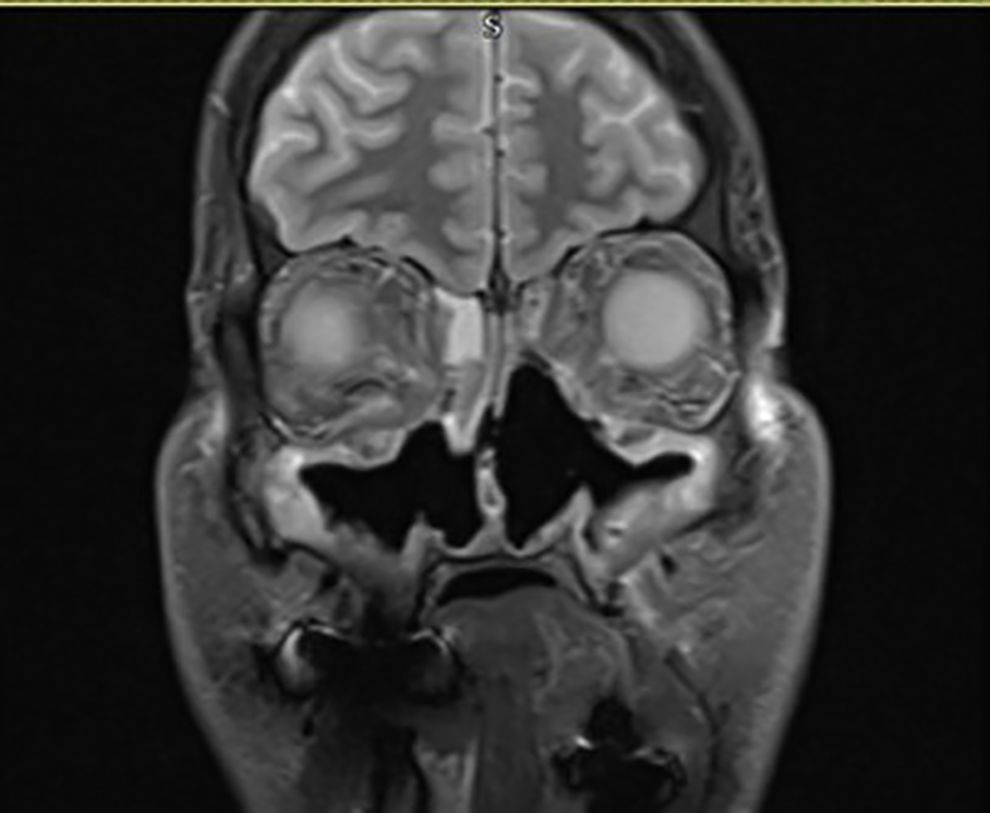
Magnetic resonance imaging (MRI) scan demonstrating septal and maxillary sinus wall destruction.
Blood tests for c- and p-ANCA were again negative and the biopsies again did not demonstrate granulomatous inflammation or vasculitis. Despite this referral was made to rheumatology for an opinion.
Based on the correlation of symptoms, a clinical diagnosis of ANCA negative granulomatosis with polyangiitis was made, and the patient was commenced on cyclophosphamide and prednisolone before switching to azathioprine.
Following this, his general systemic symptoms, ocular and nasal symptoms improved drastically. Review in the ENT clinic subsequently demonstrated healthy mucosa with minimal crusting. He remains on azathioprine with good disease control.
Discussion
Granulomatosis with polyangiitis is a necrotic small and medium vessel vasculitis. It is reported to be c-ANCA positive in between 79% and 95% of cases. 3 -5 It is usually characterized by small and medium vessel vasculitis and granulomatous inflammation affecting the upper airway, lungs, and renal system. It most commonly presents with rhinosinusitis and significant crusting, before progressing toward hemoptysis, cavitating lung lesions, and end-stage renal failure due to glomerulonephritis, if left untreated.
Although suspicious lesions within the nasal cavities should be biopsied and a positive histology has a specificity of 100%, negative histology cannot exclude GPA. Studies have shown that patients with a negative c-ANCA at presentation, may develop a positive result up to 4 years later. 6 This should therefore be repeated on multiple occasions in patient whom there is a high clinical suspicion of GPA.
Our case highlights the importance of early involvement of the rheumatology team when GPA is suspected, even in cases where c-ANCA and histology are both negative for vasculitis. Early diagnosis can prevent progression of the disease which could otherwise lead to local and systemic sequelae.
Footnotes
Authors’ Note
Written consent for publication was gained form the patient prior to manuscript submission.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.