
Abstract
Papillary urothelial carcinoma is aggressive and characterized by frequent metastasis to distant sites at an early stage. Papillary urothelial carcinoma of the urinary bladder usually metastasizes to the local lymph nodes, liver, lungs, bone, and mediastinum. Urogenital tract carcinoma of the head and neck metastasis is uncommon and rarely reported to the cervical lymph nodes. We present a case of cervical lymph node metastasis of papillary urothelial carcinoma of the urinary bladder.
Introduction
Papillary urothelial carcinoma is an aggressive and rapidly metastatic cancer. 1 Metastases of papillary urothelial carcinoma are mainly bone, regional lymph nodes, and lungs. 2 Urogenital tract carcinoma of the head and neck metastasis is uncommon but requires differential diagnosis. 3 In particular, very rarely reported metastases of papillary urinary carcinoma to the cervical lymph nodes. Herein, we present a case of cervical lymph node metastasis of papillary urothelial carcinoma.
A 73-year-old male was referred to our hospital with a 2-week history of a right neck mass. A gun biopsy was performed, and a microscopic examination revealed metastatic carcinoma. Neck computed tomography (CT) and combined positron emission tomography/computed tomography (PET/CT) were performed. The PET/CT and neck CT revealed multiple metastatic lymph nodes in the right neck level II to V and right supraclavicular space (Figure 1). He had undergone transurethral resection of bladder cancer 10 years prior. The microscopic diagnosis of urinary bladder tissue was papillary urothelial carcinoma of low grade. Three years later, the patient was diagnosed with recurrent bladder cancer. Transurethral resection of the bladder lesion was performed. Microscopic diagnosis of the urinary bladder tissue revealed low-grade papillary urothelial carcinoma (Figure 2). Follow-up was performed postoperatively every 6 months, and no recurrence was observed. We reevaluated the pathological review of the previous cervical lymph node biopsy, and the biopsy result was diagnosed as favorable for metastatic urothelial carcinoma (Figure 2). Palliative chemotherapy was administered for 6 months at the metastatic lesion of the right neck. The metastatic lesion did not respond to chemotherapy, and the patient consistently complained of neck discomfort. Therefore, we started palliative radiation therapy for 2 months at the right neck lesion. Despite radiation therapy, his condition continued to worsen, and he died 9 months after the diagnosis of neck metastasis.
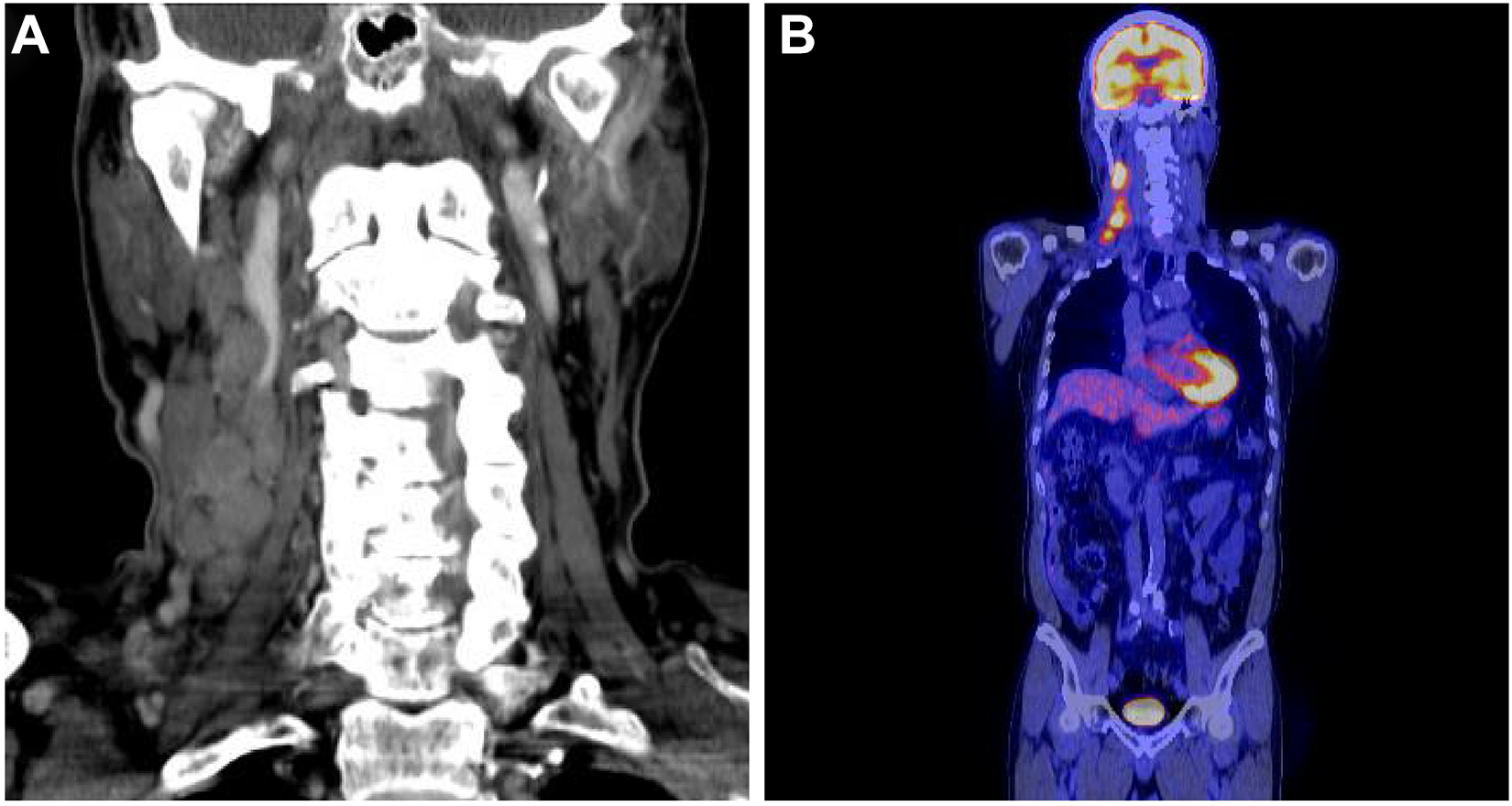
(A) CT showed multiple metastatic lymph nodes in the right neck levels II to V. (B) PET/CT showed multiple metastatic lymph nodes in the right neck levels II to V showed high FDG uptake. CT indicates computed tomography; FDG, fluorodeoxyglucose; PET/CT, positron emission tomography/computed tomography.
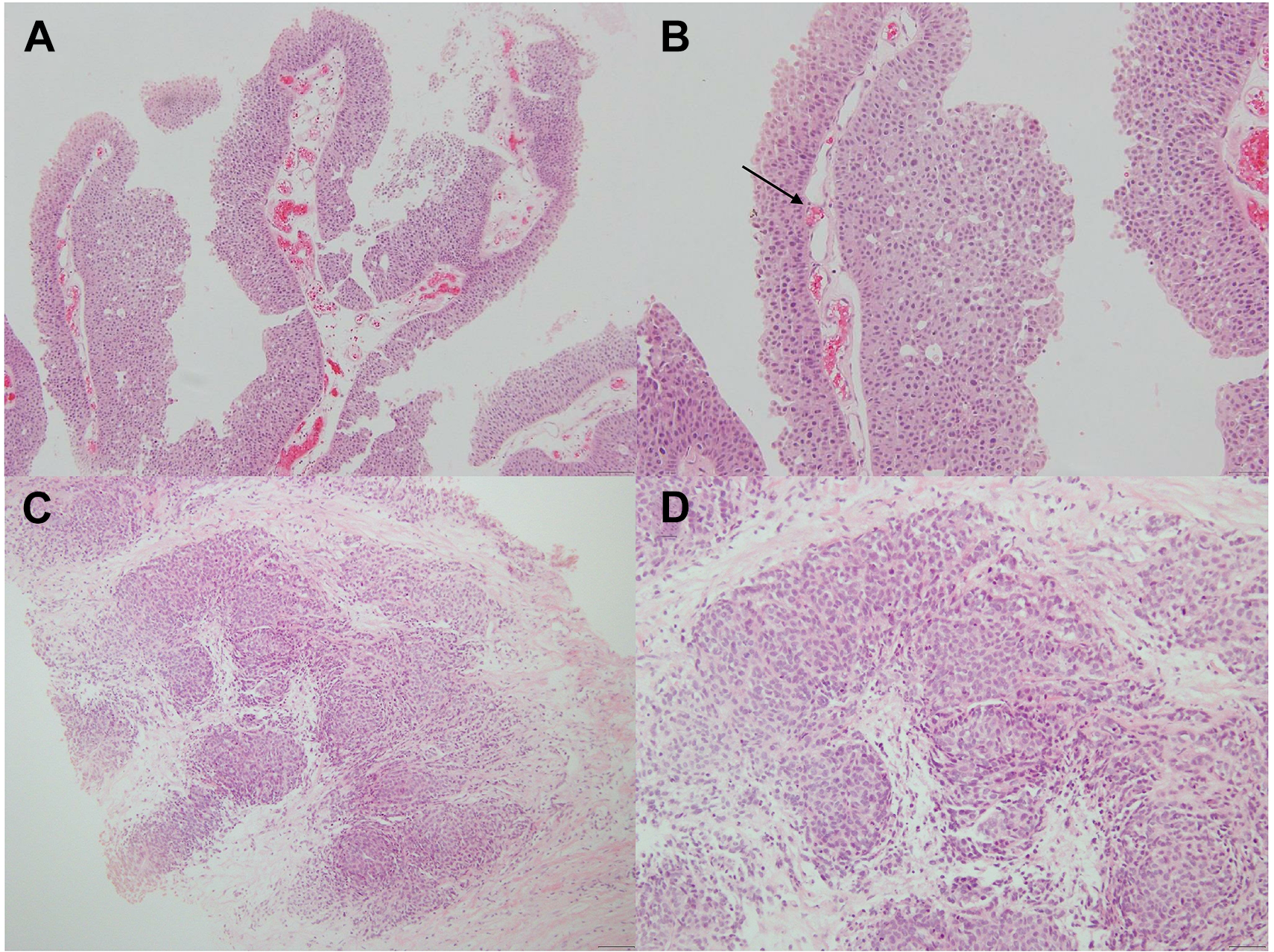
Papillary urothelial carcinoma of the urinary bladder and metastatic papillary urothelial carcinoma in the cervical lymph node. (A) Papillary urothelial carcinoma showed papillary structures are lined by urothelium, which shows minimal cytological and architectural disorders (H&E stain, ×100). (B) Arrow indicates a fibrovascular core of papillary urothelial carcinoma (H&E stain, ×200). (C) Metastatic cervical lymph node showed urothelial carcinoma growing as a nest (H&E stain, ×100). (D) Metastatic papillary urothelial carcinoma showed pleomorphism and loss of polarity (H&E stain, ×200). H&E indicates hematoxylin and eosin.
Bladder cancer is the fourth most common cancer in the United States, the fifth most common cancer in males in Western societies. 4,5 Papillary urothelial carcinoma represents 90% of malignant tumors of the bladder and is an aggressive and high tendency to metastasize. 6 Supraclavicular lymph node metastases are rare, and very few cases of papillary urothelial carcinoma metastasize to the cervical lymph nodes. 2 Hessan et al 7 identified 3 (1.4%) of 207 cases of cervical lymph nodes, and one case was reported as the first sign of neck metastasis. Our patient presented with cervical lymph node metastasis from papillary urothelial carcinoma of the bladder.
Bladder carcinoma metastasizes to the head and neck through lymphatic or hematogenous dissemination. 3 These metastases in the head and neck are most common in the nasal cavity, paranasal sinus, larynx, tongue, thyroid, and salivary glands. The invasion of the cervical lymph node by metastasis of primary cancer is mainly squamous cell carcinoma or adenocarcinoma, and it is highly likely to be at an advanced stage. 8 In metastatic squamous cell carcinoma, lung, esophageal, and cervical cancers are more likely to be primary cancers. In adenocarcinoma, the origin is likely to be the lung, breast, stomach, pancreas, and urogenital neoplasm. 9 The presence of cervical lymph node metastasis is likely to result in a high proportion of micrometastases, reflecting an advanced-stage disease. 3 In addition, survival is very poor once metastases are present. Therefore, a correct diagnosis is essential, as these patients may achieve remission and prolonged survival with chemotherapy or radiation therapy.
To the best of our knowledge, there has not been a case of confirmed metastasis to cervical lymph nodes after several years in patients with bladder cancer having papillary urothelial carcinoma, as in our patients. Therefore, clinicians should include squamous cell carcinoma or adenocarcinoma and papillary urothelial carcinoma in the differential diagnosis when cervical lymph node metastasis is present in patients with a history of bladder cancer.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.