
Abstract
Introduction:
Distortion product otoacoustic emission (DPOAE) was measured to investigate the effect of mask use and type on oxygen saturation on cochlear function in health care professionals during the COVID-19 pandemic.
Material and Methods:
Group 1 participants wore surgical masks; Group 2 participants wore N95 masks. Distortion product otoacoustic emission and oxygen saturation were measured in both groups before and after mask use.
Results:
Comparison of signal-to-noise ratio (SNR) values before and after surgical mask use in DPOAE measurements of group 1 revealed statistically significant difference in the right and left ears. Comparison of the SNR values in DPOAE measurements of group 2 before and after 8 hours of N95 mask use revealed statistically significant differences in the right ear at 988, 2963, 4444, and 8000 Hz and in the left ear at 8000 Hz.
Conclusion:
We found that prolonged mask use may affect the outer hair cells in the cochlea, causing deterioration in DPOAE values.
Introduction
The World Health Organization declared COVID-19 disease a pandemic on March 11, 2020, as more than 118 000 cases were detected in 114 countries by that date. 1 The primary route of transmission of COVID-19 disease is probably tiny droplets that are emitted by carriers of the virus as they speak, breathe, cough, or sneeze. Many health authorities recommend and even enforce the use of masks in public places by healthy individuals to ensure resource control. 2 Many professional study groups initially suggested that a standard surgical mask provided satisfactory protection, except where a clinician needed to perform high-risk procedures, such as airway intervention. Those masks were considered equally effective at protecting against droplet infections, according to a previous study comparing the efficiency of surgical masks versus N95 masks against influenza virus in health care professionals. 3 A meta-analysis on the protection provided by N95 and surgical masks against acute respiratory infection reported that the evidence was insufficient to determine whether N95 masks are superior for protecting health care professionals against respiratory infection in clinical settings, even though N95 masks offer greater protection (better sealing, less risk of penetration, etc) compared to surgical masks under laboratory conditions. 4
N95 masks are also reported to increase CO2 levels by 1.8% to 3%, possibly because of CO2 accumulation due to expired respiratory air within the N95 mask. 5 Tong et al 6 evaluated the respiratory effects of long-term N95 use in pregnant women and found that pregnant women could not maintain ventilation while breathing in an N95 mask (mean tidal volume decreased, ventilation decreased, oxygen consumption, and carbon dioxide expiration increased significantly), although this did not affect their oxygen saturation measured from the fingertip and did not change their respiratory frequency. Therefore, even though the use of N95 masks seems to be more effective in preventing infectious disease under pandemic respiratory disease conditions, surgical masks with less airway resistance are considered suitable in appropriate environments because they have fewer respiratory side effects, including hypoxia. 3
Ischemic hypoxia is an important factor in sudden hearing loss. Cochlear function may be severely impaired when blood PO2 decreases or when blood flow to the cochlea is inadequate. Many mechanisms of injury and etiopathologies have been postulated, but they share the common result of hypoxia of the organ of Corti, leading to hair cell–cilia fusion, synaptic and dendritic swelling, and sustained depolarization. Of all the various treatments tried, only corticosteroids and hyperbaric oxygen (HBO2) therapy have shown benefits in randomized controlled trials. Park et al showed that the cochleas of mice exposed to hypoxia showed significant histological aging and damage compared with the unexposed control group. 7 Auditory hair cell damage and apoptosis were observed as a result of hypoxia-induced oxidative stress and mitochondrial dysfunction. 7 Similarly, Yılmaz et al found that hypoxia caused a decrease in hearing thresholds, deterioration of distortion product otoacoustic emission (DPOAE) results, and long-term prolongation of the interpeak latencies I to V in the auditory brainstem response in a study of 60 patients with chronic obstructive pulmonary disease (COPD). However, they were unable to determine the critical oxygen level that impairs hearing functions. 8
Hearing damage can be detected using otoacoustic emission (OAE), a type of sound energy produced by the cochlea that can be recorded in the external ear canal. Otoacoustic emission reflects the functional status of the outer hair cells in the cochlea and is categorized as spontaneous OAE and evoked OAE (EOAE). A further type of EOAE that is commonly used in clinical practice is DPOAE, a type of acoustic energy induced by 2 pure tones (f1 and f2). 9 These OAEs deteriorate under hypoxic conditions due to the high sensitivity of the cochlear outer hair cells in the early period of hypoxia.
Some researchers have suggested that cochlear changes caused by hypoxia can be evaluated by OAE measurements in the early period. 8 The aim of the present study was to investigate the effect of COVID-19 pandemic mask use and type of oxygen saturation and cochlear DPOAE measurements in health care professionals.
Materials and Methods
The age, gender, and mask type worn by 128 health personnel working at Adana City Training and Research Hospital were recorded between October 2020 and December 2020. Participants using surgical masks were included in group 1 (control; n = 27) and those using N95 masks were included in group 2 (n = 28). Participants were included in the study if they showed a normal otoscopic examination in an ENT examination and had no previous ear surgery history. Personnel working in environments such as the intensive care unit and telephone exchange, where noise exposure in the working environment is constant, was excluded from the study. The participants were doctors, nurses, secretaries, and workers from the polyclinic. Personnel with chronic diseases, such as ischemic heart disease and chronic lung disease, was not included in the study. Patients with increased hearing loss at high frequencies were not included in the study.
Audiometry examination tests were conducted by the same audiometrist. Air and bone conduction hearing thresholds were recorded at 250, 500, 1000, 2000, 4000, and 8000 Hz using the right ear pure tone audiometry test and clinical audiometry/otometrics/Madsen Astrera model. Personnel with a pure sound average of 20 dB and below was included in the study. Oxygen saturations were measured and recorded using the “Fingertip Pulse Oximeter (YonkerGlife Yk-81a)” device.
The DPOAEs, which are low-level acoustic signals measurable from the ear canal in the presence of an external acoustic stimulus, were measured using a Neuro-Audio/OAE device (version 2010, Neurosoft) set at 500 to 8000 Hz and recorded as a distortion-product (DP-gram). The DPOAE stimulus intensity was set to 55 for the L1 and L2 levels; the ratios of the f1 frequency (65 dB SPL) and the f2 frequency (55 dB SPL; f2/f1) were set to 1.22. The signal-to-noise ratio (SNR) values were recorded at different frequencies (0.988, 2.222, 2.963, 5.714, and 8.000 Hz). The DPOAE and saturation values (8 hours shift) were measured in both groups before and after mask use. The data of both groups were compared statistically.
Our study was conducted in accordance with the Declaration of Helsinki. Signed informed consent was obtained from every participant. Ethics Committee Approval (Meeting Number: 70, Decision Number: 1129, Date: 18/11/2020) was obtained from the Ethics Committee.
Statistical Analysis
The normal distribution of continuous variables was evaluated with Shapiro-Wilk statistics. An independent t test was used to compare 2 independent groups that had a normal distribution. A χ2 test was used for the categorical variables. A paired t test was used for dependent variables. Numerical variables were expressed as mean ± standard deviation values, and categorical variables were expressed as frequencies and percentages in summary statistics. A value of P < .05 was considered statistically significant. All analyses were performed using the IBM SPSS 22 software package trial version.
Results
In total, 72 people using surgical masks (group I) and 56 people using N95 masks (group II) were included in our study. Of those who used surgical masks (group I), 24 (33.3%) were female and 48 (66.7%) were male, whereas 28 (50%) of those who used N95 masks were female and 28 (50%) were male.
Evaluation of the type of mask used according to age revealed a mean age of 33.11 ± 8.08 years for group I and 37.29 ± 9.71 years for group II; this difference between the 2 groups was statistically significant. The use of an N95 mask was preferred as the age increased (P = .009).
The mean oxygen saturation value for group 1 was 98.78 ± 0.92 before mask use and 97.33 ± 2.0 after mask use, and the difference was statistically significant (P < .001). The mean oxygen saturation value for group 2 was 99.00 ± 0.00 before mask use and 97.93 ± 1.35 after mask use, and the difference was statistically significant (P < .001). Both the surgical and N95 masks caused a decrease in oxygen saturation.
Comparison of the SNR values at 988, 1481, 2222, 2963, 4444, 5714, and 8000 Hz frequencies for the DPOAE measurements in group 1 before and after surgical mask use revealed a statistically significant difference in the right ear at 5714 Hz (P = .034) and in the left ear at 1481, 2222, 4444, 5714, and 8000 Hz (P = .002, .009, <.001, <0.001).
Comparison of SNR values at 988, 1481, 2222, 2963, 4444, 5714, and 8000 Hz frequencies for the DPOAE measurements in group 2 before and after 8 hours of N95 mask use revealed a statistically significant difference in the right ear at 988, 2963, 4444, and 8000 Hz (P = .004, .008, .001, .003) and in the left ear at 8000 Hz (<.001; Table 1).
The Relationship Between the Use of Surgical Mask and N95 Mask With O2 Saturation and DPOAE Values Before and After Shifts.
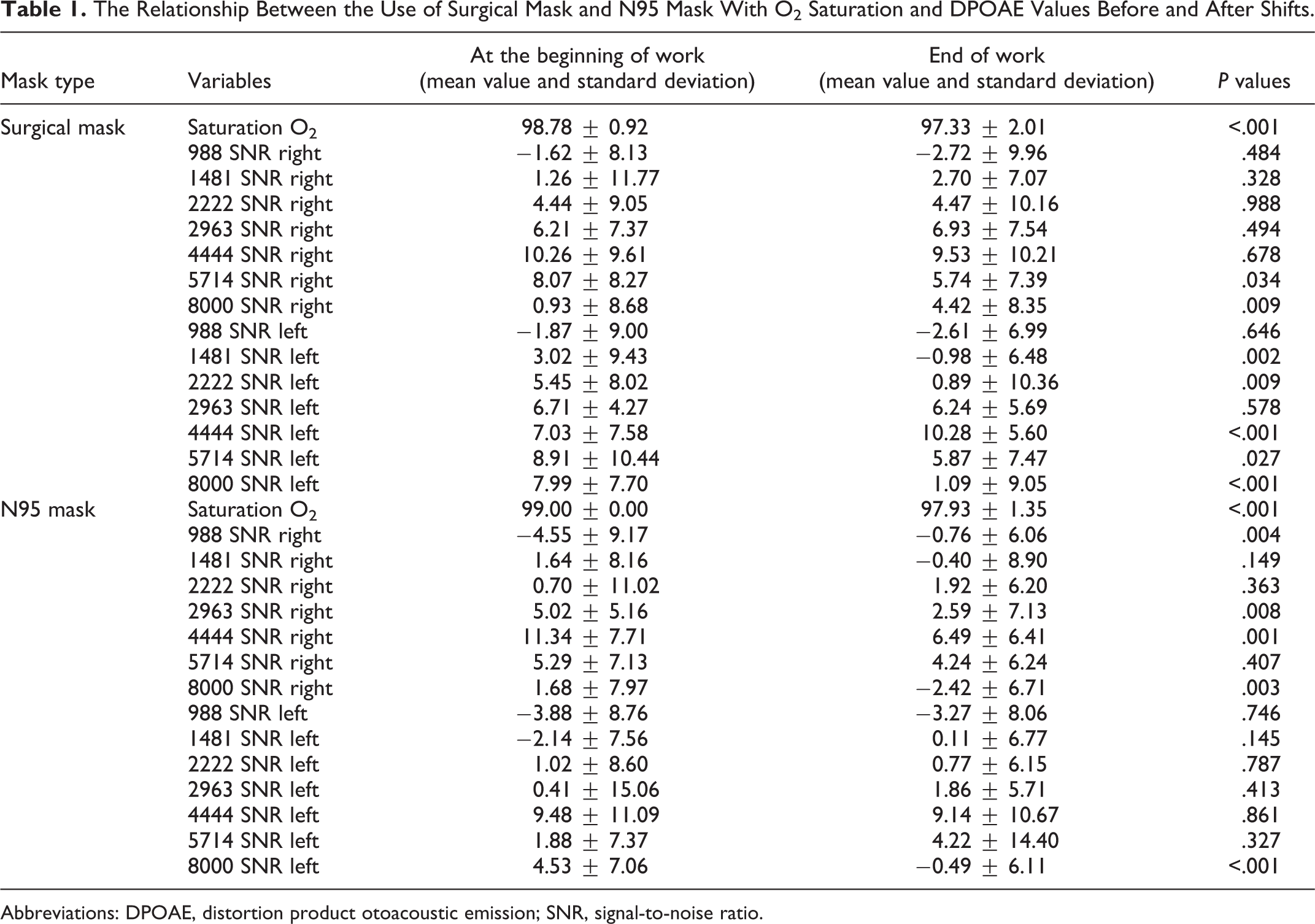
Abbreviations: DPOAE, distortion product otoacoustic emission; SNR, signal-to-noise ratio.
The hearing values for a person using a surgical mask are shown in Figures 1 and 2 at the beginning and end of working hours.
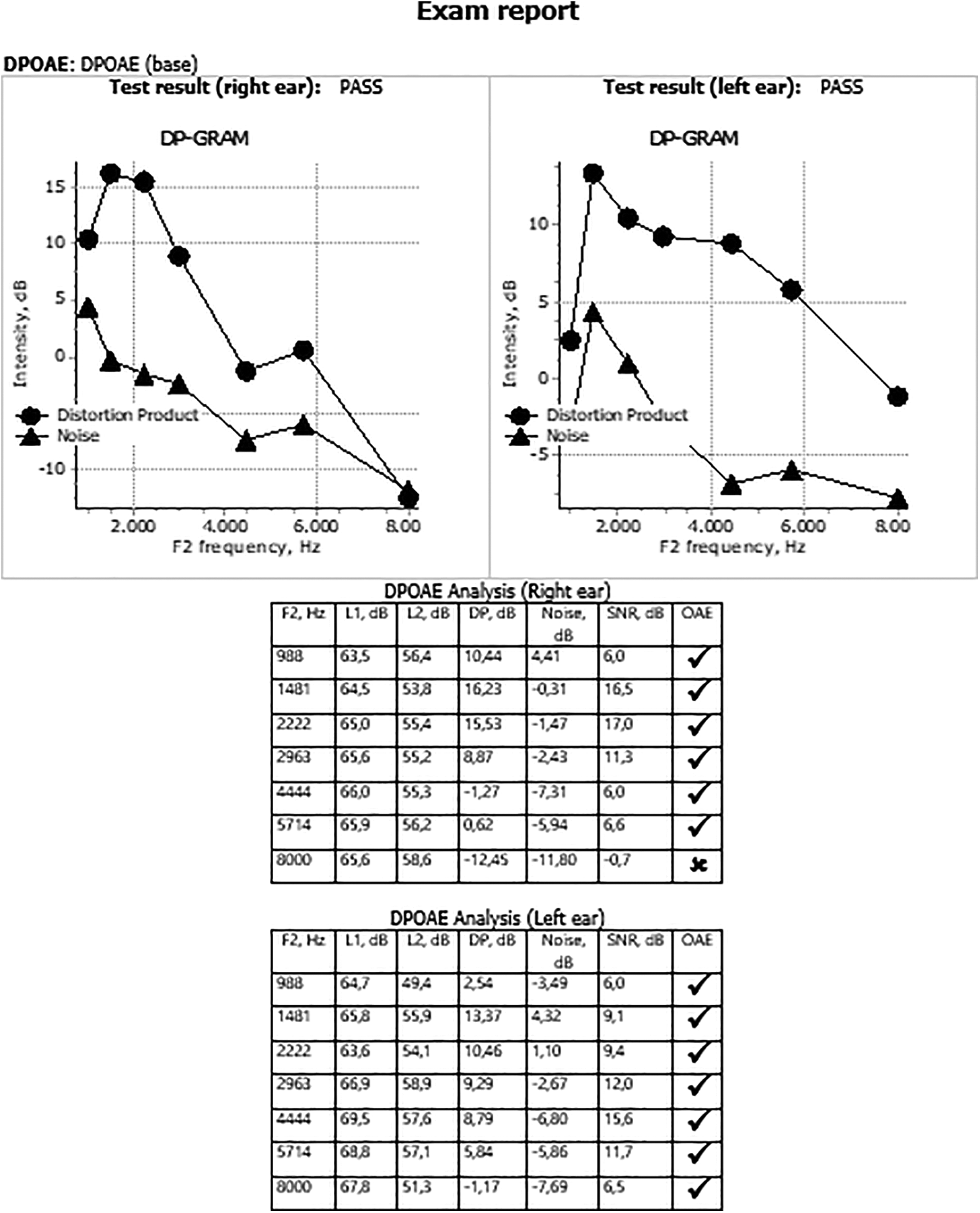
Distortion product otoacoustic emission (DPOAE) measurement sample before the shift.
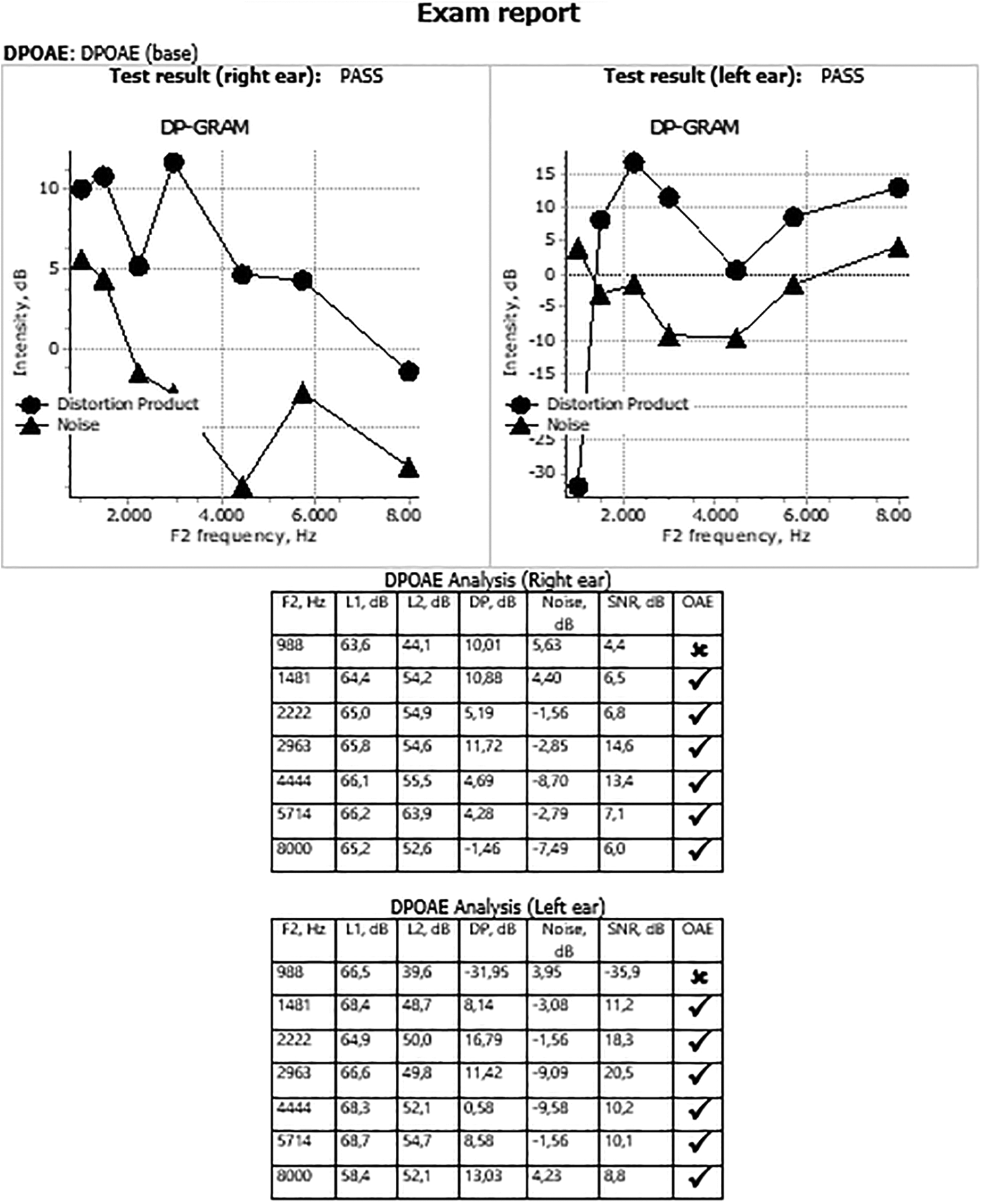
Distortion product otoacoustic emission (DPOAE) measurement sample after the shift.
Discussion
COVID-19 is transmitted through droplets and causes severe respiratory failure. It has affected most countries worldwide and continues to pose a serious threat to public health. Currently, mask use is mandated by many authorities despite differences in the recommendations for mask use. 10 The aim of the present study was to use OAE to reveal the cochlear changes caused by hypoxia due to mask use, rather than to determine the differences between N95 masks and surgical masks, even though N95 respirators are reported to have significantly greater side effects than surgical masks. 11 Hypoxia affects OAEs because it affects hearing thresholds, leading some researchers to suggest that cochlear changes caused by hypoxia can be evaluated by OAE measurements in the early period. 8
Li et al 9 conducted a study on 58 patients with obstructive sleep apnoea–hypopnoea syndrome (OSAHS) and on 20 patients without OSAHS and found that DPOAE amplitude decreased significantly in OSAHS patients even though no hearing loss was observed. They concluded that chronic hypoxia of the cochlea may damage the outer hair cells in the cochlea, thereby impairing cochlear function in OSAHS patients. They stated that DPOAE could be used to monitor the cochlear function of OSAHS patients, as the changes in DPOAE amplitude were observed to occur earlier than changes in hearing thresholds. 9
Tong et al 6 presented evidence to support the view that pregnant health care professionals should refrain from using long-term N95 mask use in the third trimester. Their study on 20 pregnant health care professionals in 2015 revealed that breathing through N95 masks increased oxygen intake and carbon dioxide production, both during rest and at low work intensity, as a result of the increased workload on respiration caused by the use of masks. 6
Yılmaz et al 8 reported a mean SNR of 17.6 (8.3-27.0) for DPOAE in the control group versus 5.4 (0.2-15.0) for patients with COPD. This difference in DPOAE was statistically significant (P < .001), and they concluded that hypoxia due to COPD caused a long-term decrease in hearing thresholds and a deterioration in the DPOAE results. 8
Our results in the present study indicated that the use of N95 masks was preferred in health care workers with increasing age (P = .009). This preference may reflect the department policies where the health care personnel worked or the fact that this age group may exhibit more protective behavior because of the more aggressive course of COVID-19 in persons of advanced age. The importance of using masks to prevent the spread of COVID-19 is indisputable, but we show that the use of either surgical or N95 masks causes a decrease in oxygen saturation. The mean oxygen saturation value for group 1 was 98.78 ± 0.92 before mask use and 97.33 ± 2.0 after mask use and the difference in oxygen saturation was statistically significant (P < .001). The mean oxygen saturation value for group 2 before mask use was 99.00 ± 0.00 and 97.93 ± 1.35 after mask use, and the difference was again statistically significant (P < .001).
Comparison of SNR values at the different frequencies used for DPOAE measurements before and after surgical mask use revealed statistically significant differences in the right ear in group 1. Similarly, a comparison of the SNR values at the different frequencies for DPOAE measurements before and after 8 hours of N95 mask use revealed statistically significant differences in the right and left ears. We found that prolonged mask use may affect the outer hair cells in the cochlea, causing deterioration in DPOAE values.
We believe that our study will guide further research into potential hearing loss due to long-term mask use. Our findings contribute to the current literature by revealing the undesirable effects of the prolonged use of protective masks and the importance of taking measures in this regard. The present gap in our knowledge regarding prolonged mask use may have an impact on populations other than health care staff, given the protective mask recommendations made for patients with chronic diseases (ie, congestive heart disease and COPD).
Footnotes
Author’s Note
Ragıp Onur Oztornaci is also affiliated with Department of Biostatistics and Medical Informatics, Faculty of Medicine, Mersin University, Mersin/TURKEY.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.