
Abstract
Significance Statement
Petrous cholesteatoma is rare but frequently leads to complications. A thorough radiological evaluation helps in identifying the pathology and the extent of disease. Sound anatomical knowledge is vital for the planning of surgical approach to get adequate access without damaging important structures. Presentations in congenital lesions are varied due to the uneven growth model of the temporal bone. To the best of our knowledge, the pattern of involvement in this case has never been reported earlier.
Case
A 35-year-old patient presented with a slowly progressive right-sided facial weakness for 6 months. He gave history of sudden onset of right-sided hearing loss 10 years ago. There was no history of ear discharge, trauma, ototoxic drug intake, ear surgery, or meningitis. Tympanic membrane was intact. The facial nerve had House-Brackmann (HB) grade 3 palsy. Right-sided profound sensorineural hearing loss was found on pure tone audiometry. Caloric testing and cervical—vestibular evoked myogenic potential—revealed a nonfunctional labyrinth on the right side. All other cranial nerves functions were normal.
A high-resolution computerized tomography scan of the temporal bone (Figure 1A) showed 2 separate soft tissue lesions. The first soft tissue density was in the right petrous apex, extending up to the temporal lobe and posterior–inferior to the internal jugular vein, eroding the internal auditory canal, and the basal turn of cochlea. A second lesion was identified in the mastoid region, extending up to the sigmoid sinus. On magnetic resonance imaging (Figure 1B), both the petrous and mastoid lesions appeared isointense on T1and hyperintense on T2 imaging. There was no contrast enhancement. Diffusion restriction was present. No communication between these 2 lesions was detected. Based on radiology, the diagnosis of 2 unilateral synchronous temporal bone cholesteatomas was made.
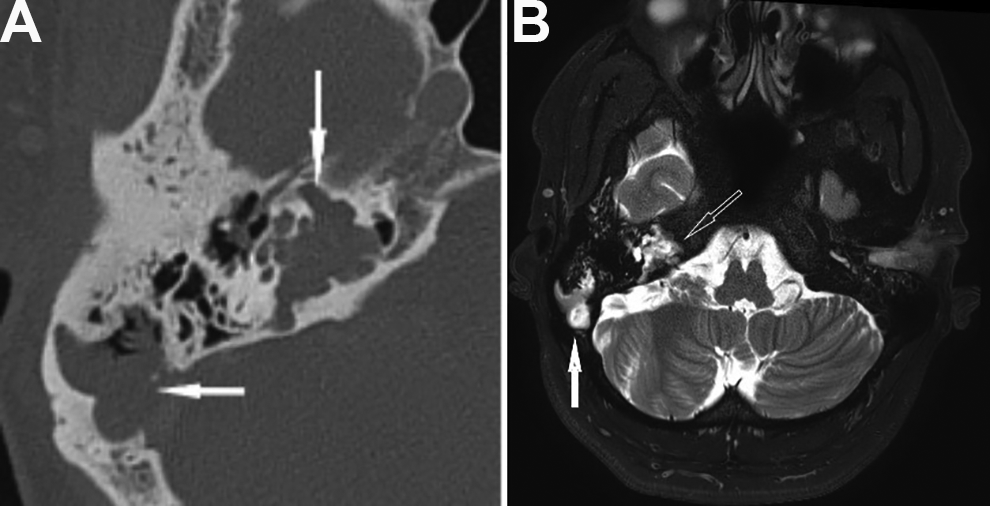
(A) Lesions in right petrous apex (vertical white arrow) and mastoid (horizontal white arrow). Bone erosion in the region of IAC, petrous apex, and facial nerve canal and sigmoid plate. (B)T2-weighted magnetic resonance imaging (MRI) hyperintense lesions in petrous apex and mastoid.
Postaural transotic approach was chosen for removing these lesions. During surgery, the mastoid lesion (Figure 2) was identified first. The sigmoid sinus was exposed by the lesion. The supra and retrolabyrinthine cells were intact, but they were harboring cholesteatoma flakes. After the labyrinthectomy, a large cholesteatoma was found, encasing the nerve bundle of the internal auditory canal, eroding the basal turn of cochlea, and extending toward the petrous apex (Figure 3). The middle and posterior fossa dura and the sigmoid sinus were also exposed. At the end of the surgery, cerebrospinal fluid (CSF) leakage from the porous region of the internal auditory canal was noted, eustachian tube was blocked and the cavity was obliterated by fat with cul-de-sac closure of the external auditory canal.
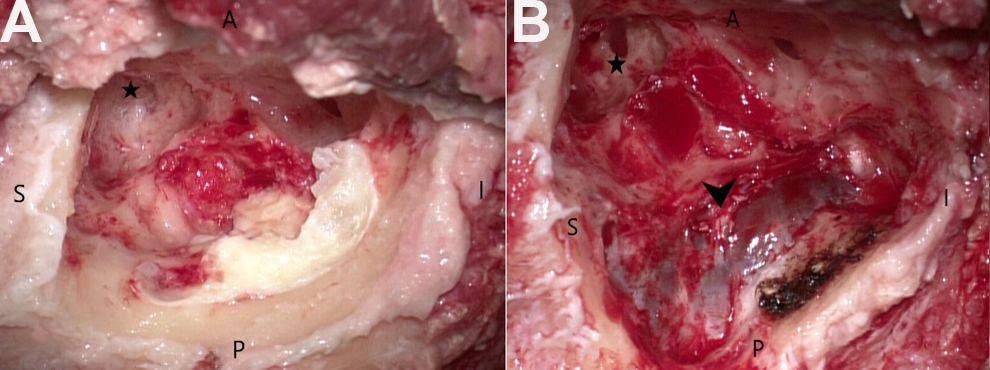
(A) Lateral cholesteatoma mass identified in the mastoid region. (B) After removal of mastoid cholesteatoma, sigmoid sinus was exposed. Part of the sac wall (black arrow) adherent to the sinus was carefully dissected off. A indicates anterior; Black star, antrum; I, inferior; P, posterior; S, superior.

(A) Before labyrinthectomy. Black stars—Semicircular canals; small black arrow: Cholesteatoma appearing posterior to the canals inside intact retrolabyrinthine cells (visible after uncapping of retrolabyrinthine cells). (B) After labyrinthectomy. Black arrow—Cholesteatoma medial to the labyrinth (C) Facial nerve exposed after removal of cholesteatoma. White arrowhead—first Genu; Yellow arrowhead—second Genu of facial nerve; Black arrow—Cholesteatoma medial to facial nerve; White star—Meatal segment of facial nerve.
The histopathology confirmed the diagnosis of cholesteatoma. There was no sign of CSF leak, vertigo, or meningitis in the postoperative period. However, the facial nerve remained at HB grade-3 after 3 months of follow-up.
Discussion
Petrous bone cholesteatomas (PBCs) are epidermoid cysts of the petrous part of the temporal bone. They constitute about 4% to 9% of petrous pyramid lesions and <3% of temporal bone cholesteatomas. The rarity, slow growth, complex location in the skull base, and proximity to vital neurovascular structures make the treatment challenging. The proximity to the labyrinth and the facial nerve puts hearing and nerve function at risk, with the incidence of facial nerve palsy reported at 34.6% to 100%. 1
Sanna et al 2 classified PBCs into 5 types according to their location, which they further expanded to include extension outside the temporal bone. The classification allows for planned surgical management, which facilitates functional preservation while minimizing the risk of complications and recurrence.
The aim of the surgery should be complete eradication of disease with preservation of nerve functions and prevention of complications. Hearing is affected in most patients but when present, an effort should be made to preserve it. Complete removal of adherent matrix from the sigmoid sinus, jugular bulb, and the dura is challenging but these remnants can be safely cauterized. 3 Obliteration of the cavity prevents CSF leak, provides protection to vital structures, and avoids cavity problems. 4 The disadvantage is that recurrence cannot be visualized, and detection of occult disease development needs regular radiological evaluation.
A thorough search of literature did not reveal any reports of more than one, distinct cholesteatomas in the same temporal bone or cholesteatomas with a growth pattern of 2 expansile lesions connected by an array of intact cells. The microscopic involvement of intervening cells underlines the importance of exenteration of the surrounding cells in cholesteatoma surgery and examining these cells for evidence of disease.
Petrous bone cholesteatomas are hypothesized to arise from embryonic epithelial cell nests. 5 In this case, as the cholesteatoma was present in the petrous apex and posterior part of the temporal bone, its embryological origin may be from the posterior saccules part of saccus medius. 6 The presence of cholesteatoma flakes in the intervening cells led us to think that the 2 larger lesions were connected in the early part of ear development but were separated and became distinct lesions with the growth of temporal bone leaving a trail cholesteatoma flakes in the intervening cells.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.