
Abstract
A persistent stapedial artery is a congenital vascular malformation that can cause tinnitus and/or conductive hearing loss. Although rare, this case highlights the importance of recognizing aberrant anatomy as a potential cause of patients’ symptoms. It also demonstrates how to recognize and treat patients with a symptomatic persistent stapedial artery.
A 33-year-old female presented for evaluation of gradual-onset bilateral hearing loss, left worse than the right, which she began to notice approximately 7 years prior to presentation. The patient also reported a history of a pressure sensation in both ears that worsened during flares of her seasonal allergies and a history of pediatric ear infections.
On physical examination, the patient had retraction of the right tympanic membrane against the promontory anteriorly without contacting the ossicles, and left tympanic membrane retracted against the promontory and in contact with the long process of the incus posteriorly. Negative pressure insufflation allowed the tympanic membranes to be elevated off of the promontory, but the tympanic membrane was adherent to the long process of the incus on the left. There was also a poorly visualized pulsation within the left posterior inferior quadrant. Tuning fork testing lateralized to the left at 256, 512, and 1024 Hz with abnormal Rinne results at all 3 frequencies as well. Audiogram showed normal hearing across frequencies in the right ear, and a moderate to moderately severe conductive hearing loss (CHL) in the left ear. A computed tomography (CT) scan was performed due to the pulsatile finding in the left middle ear space. The CT revealed bilateral aerated mastoids and middle ear spaces with a persistent stapedial artery (PSA) in the left middle ear space.
The patient was offered exploratory surgery for the left ear which she accepted. The tympanic membrane was elevated off the incus which revealed demineralization of the long process of the incus. A PSA was noted. The fibrous union was debrided revealing erosion of the anterior crus of the stapes which provided a clear view of the artery (Figure 1). An incudostapedial prosthesis and cartilage tympanoplasty was performed (Figure 2). Her postoperative audiogram showed complete closure of the air-bone gap with only a mild CHL at 4000 and 8000 Hz.
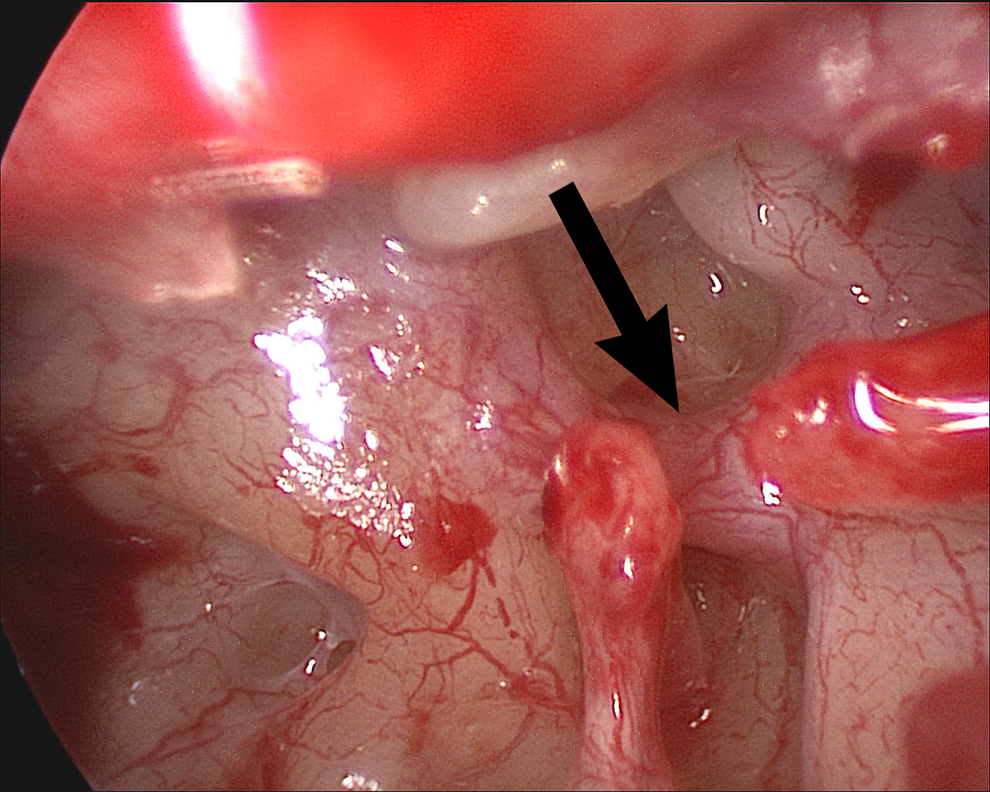
The left middle ear. The malleus is noted at the tail of the black arrow. The arrowhead indicates the persistent stapedial artery. The stapedial tendon and posterior crus (below the arrowhead) are visualized but the anterior crus is absent.
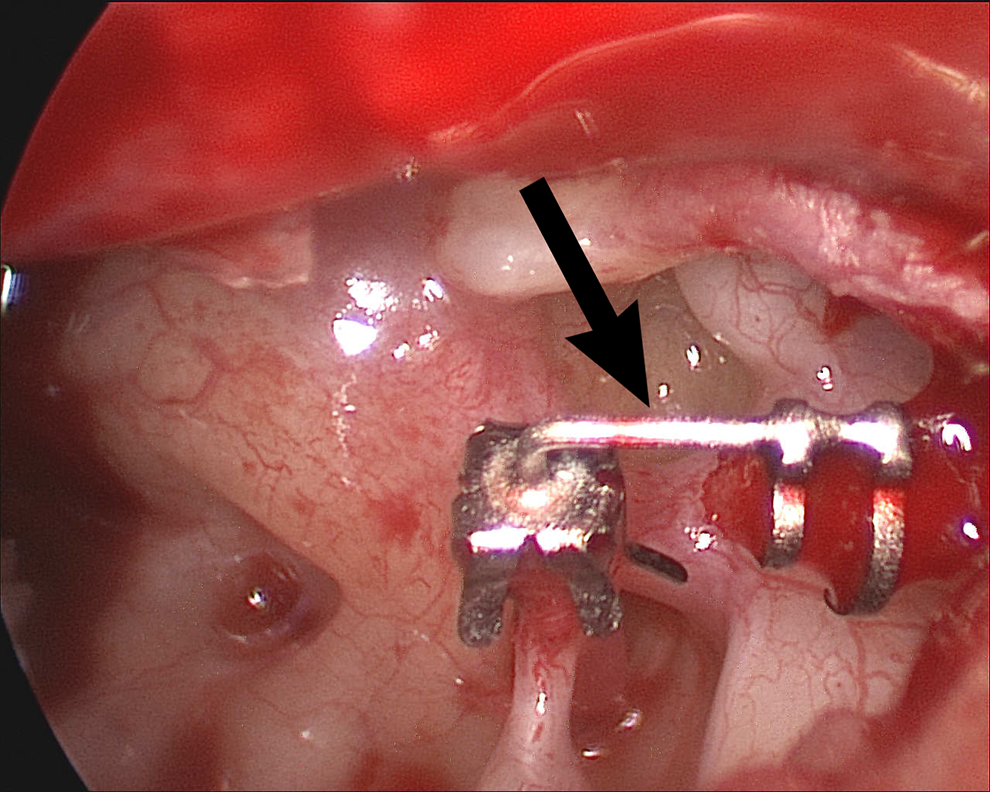
The left middle ear with prosthesis in position. The arrow again indicates the persistent stapedial artery.
The stapes and stapedial artery are derivatives of the second branchial arch. 1,2 The stapedial artery arises during the fourth or fifth week of embryonic development from the hyoid artery and usually degenerates several weeks later. 1,3 The artery transiently exists in the middle ear where it penetrates the ring of the mesenchymal stapes and enters the fallopian canal. The artery ultimately gives rise to the middle meningeal artery (MMA) and enters the intracranial cavity via the foramen spinosum. 3 During the 10th week of development, the stapedial artery usually degenerates, leaving an opening underneath the arch of the stapes called the stapedial foramen. 4,5
In 0.02% to 0.05% of the population, the stapedial artery fails to degenerate, leading to a PSA. 1,6 The persistent artery has a typical course, arising from the internal carotid artery (ICA), traversing a portion of Jacobson’s canal, passing through the stapedial foramen, and entering the fallopian canal posterior to the cochleariform process. 4 In these patients, the MMA typically arises from the stapedial artery, leading to involution of the foramen spinosum. 3 The ICA also typically takes an aberrant course as a collateral to supply the MMA. 1,7
The diagnosis of a PSA is typically made by CT scan, which shows absence of the ipsilateral foramen spinosum and a widened fallopian canal. 8 Other radiologic indicators include a soft tissue density in the region of the proximal tympanic segment of the facial nerve and a widened space between the stapes crura. 1,8
Patients with a PSA may present with pulsatile tinnitus or, rarely, CHL due to the artery limiting the movement of the stapes. 9 Most commonly, patients are asymptomatic with the PSA discovered incidentally as a pulsatile mass on otoscopic examination or during middle ear surgery. 10 Symptomatic PSA may be treated by laser coagulation of the artery, although there are associated risks. 9,11 Since the facial nerve is vascularized by a branch of the MMA (the superior petrous artery), there is risk of facial nerve palsy. This risk is low due to rich anastomoses with the stylomastoid artery. 11 There is also risk of devascularization and resultant ischemia of the pyramidal tract, lemniscus, and trapezoid body with central auditory and vestibular impairment. 11 Since a PSA is an embryologic malformation, patients have often noted pulsatile tinnitus their entire lives. Our patient expressed surprise that pulsatile tinnitus was abnormal. In our patient, we elected to repair the ossicular chain and leave the PSA unmolested.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.