
Abstract
Significance Statement
Head and neck paragangliomas are uncommon pathologies that present with common symptoms such as pulsatile tinnitus and aural pressure. This article highlights an unusual presentation of a patient with facial paresis who was found to have a jugular paraganglioma. Emphasis is placed on how the otologic examination showed a pulsatile middle ear mass that led to the diagnosis. This case illustrates the importance of maintaining a healthy degree of clinical suspicion when encountering common complaints.
An 84-year-old woman presented with a 6-month history of right facial paresis that was preceded by ipsilateral facial twitching. She also noted intermittent right pulsatile tinnitus, aural fullness, and hearing loss. Her medical and otologic history were otherwise unremarkable. Physical examination demonstrated a House-Brackmann 3/6 right facial paresis, and otologic examination revealed a red, pulsatile mass in the middle ear space with erosion of the ear canal (Figure 1 and Video). Computed tomography demonstrated a lesion at the jugular foramen with bone erosion and extension to the middle ear (Figure 2), and magnetic resonance imaging showed a contrast-enhancing lesion of the jugular foramen suggestive of a jugular paraganglioma (Figure 3). Due to the patient’s advanced age and potential morbidity of surgery, she elected for nonsurgical management with stereotactic radiosurgery. Upon completion of treatment, facial nerve outcomes were clinically similar as prior to treatment.
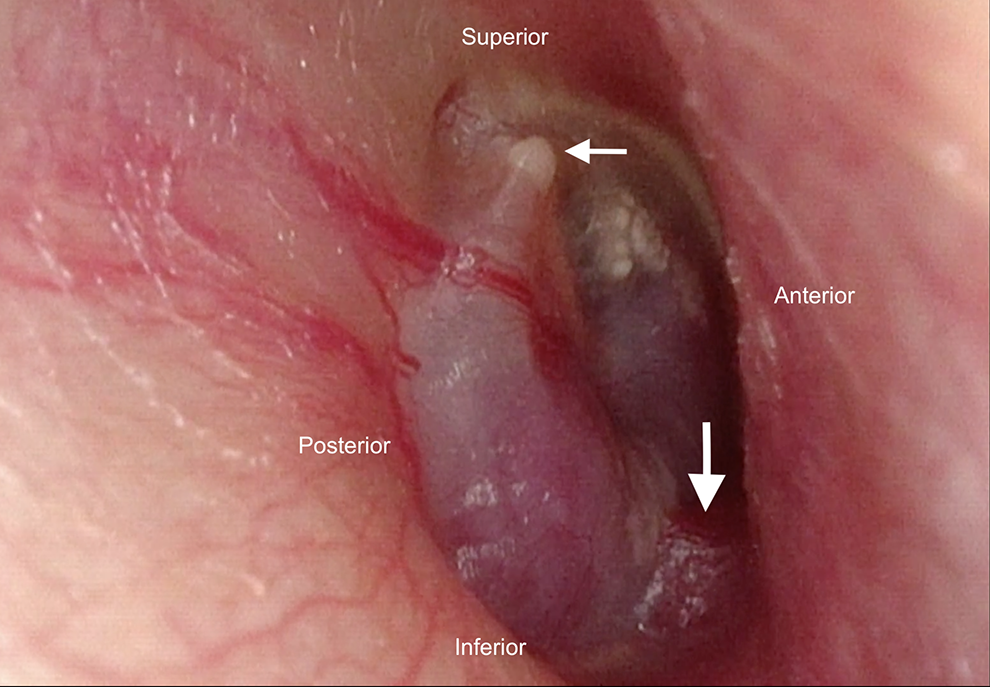
(A) Otoscopic findings of the right ear demonstrating a red middle ear mass with erosion through the inferior ear canal (large arrow). The short process of the malleus is shown for reference (small arrow). (B) The accompanying video highlights the pulsatile nature of the mass, which suggests a vascular lesion.
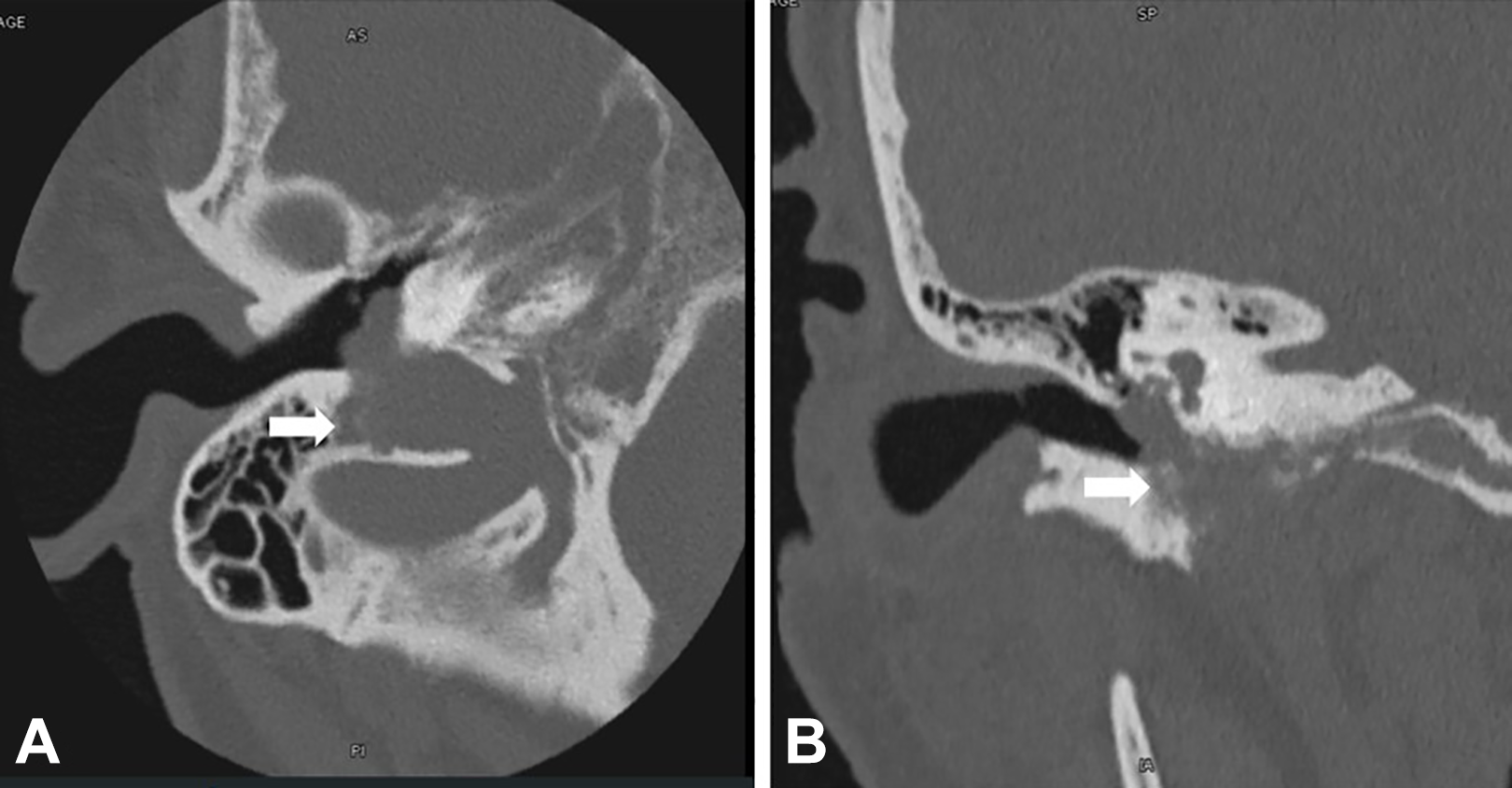
(A) Axial noncontrast computed tomography (CT) scan of the right ear demonstrating an erosive process extending from the jugular bulb (arrow) into the hypotympanum and middle ear space. (B) Coronal noncontrast CT demonstrating erosion of the inferior ear canal (arrow) and extension from the hypotympanum and jugular bulb.

Axial T1 magnetic resonance imaging (MRI) image with contrast showing an enhancing mass of the right jugular foramen. Prominent flow voids (arrow) suggested a vascular lesion, making paraganglioma the most likely diagnosis.
Paragangliomas are neuroendocrine tumors that can arise in the head and neck and often present with symptoms of pulsatile tinnitus and hearing loss. Facial paresis can be a presenting sign of jugular paragangliomas, although this is rare and usually seen in tumors of advanced size. 1,2 In this case, the facial paresis in the setting of a middle ear mass raised the suspicion of various benign and malignant tumors, including facial nerve schwannomas or adenomatous carcinoma of the middle ear. The unilateral cranial neuropathy, along with the unilateral hearing loss and pulsatile tinnitus, represented alarming signs that prompted further investigation. The otologic examination was helpful in determining the appropriate diagnosis because the pulsatile nature of the mass suggested a vascular tumor that made paraganglioma more likely, as opposed to other middle ear tumors. The otoscopic examination also demonstrated subtle areas of erosion along the floor of the ear canal, suggesting that the tumor developed from the hypotympanum, where paragangliomas originate at the jugular bulb. Although histopathological diagnosis was not available, radiologic imaging confirmed the clinical suspicion of a jugular paraganglioma, which was considered given the presented history and examination findings.
This case demonstrates how close inspection of a middle ear mass via otologic examination and appropriate imaging, as well as attention to the pulsatile nature of the mass, can offer insights to the likely diagnosis. This is particularly true when there is an atypical presentation of the mass, as in our patient, who presented with facial paresis in the setting of a jugular paraganglioma.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.