
Abstract
Significance Statement
Pulsatile tinnitus with erythematous tympanic membrane mass suggests vascular pathologies such as dural arteriovenous fistula, glomus tympanicum, or aberrant carotid artery. Jugular bulb aneurysmatic diverticulum is rare but should be suspected in a case with the presence of aneurysm in other organs. An imaging study is mandatory to confirm the diagnosis. Patient must avoid digging ear as it can cause profuse bleeding. Treatment option can be open surgery or endovascular treatment.
Clinic
A 67-year-old female with a background history of chronic lung disease complicated with pulmonary hypertension complained of an insidious onset of right-sided tinnitus along with reduced hearing for the past 5 years. The tinnitus was pulsatile and persisted throughout the day. Her symptoms progressively worsened for the past 6 months, which prompted her to a clinic visit. Otherwise, she denied otorrhea, otalgia, and vertigo. There was also an absence of focal neurological symptoms. An otoscopic examination (Figure 1) of the right ear revealed a pulsatile mass medial to an intact tympanic membrane. The lesion was lobular and appeared hyper vascularized, obscuring the view of the mesotympanum and hypotympanum. Tuning fork assessment showed a conductive element of right hearing loss, which correlated with audiometry finding of a right mixed hearing loss with an air-bone gap of 20 to 40 dbHL. Neck and other cranial nerves’ assessments were unremarkable.
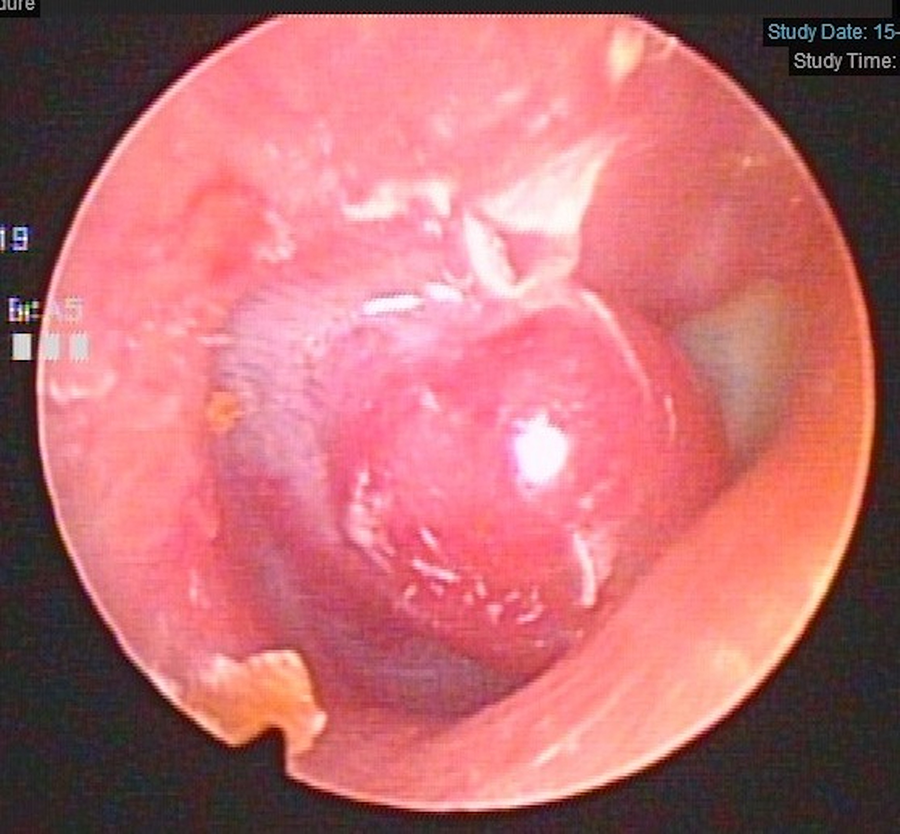
Rigid otoscopy shows reddish outpouching mass over superoposterior part of the right tympanic membrane.
High-resolution computed tomography (HRCT) of the temporal bone (Figure 2) revealed an outpouching jugular bulb through a bony defect of the right jugular foramen. The jugular diverticulum further protruded into the retrotympanum, coherent with the otoscopic finding of a hyperemic pulsatile mass medial to the pars tensa. Intriguingly, a concurrent HRCT of the thorax intended to assess her chronic lung disease also unveiled multiple dilated paravertebral vessels (Figure 3). A transcanal endoscopic compression of the jugular diverticulum was offered, to which the patient declined and opted for conservative treatment with conventional hearing aid. The lesion remained static in size at her 6-monthly surveillance.
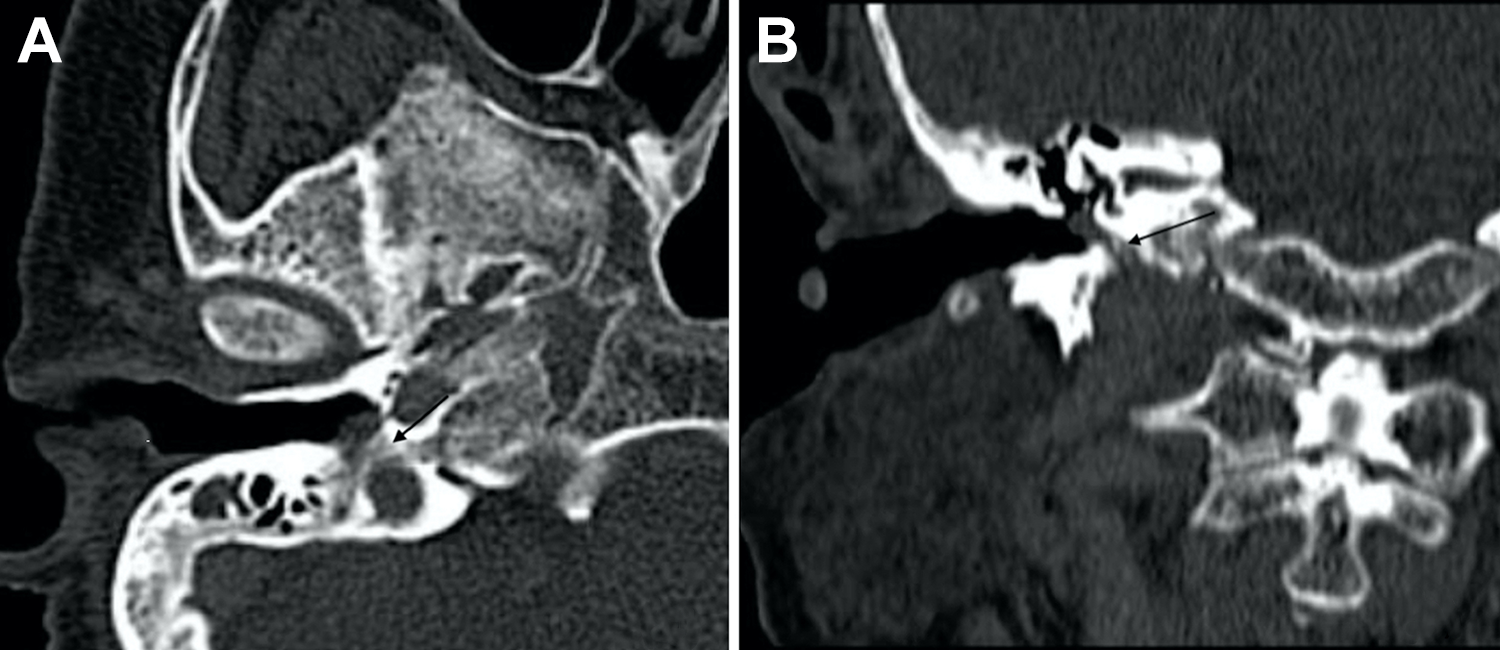
High-resolution computed tomography (HRCT) temporal bone in axial view (A) and coronal view (B) shows bony dehiscence (marked by arrow) over anterior jugular bulb, with outpouching from the jugular bulb into the middle ear and against the tympanic membrane.
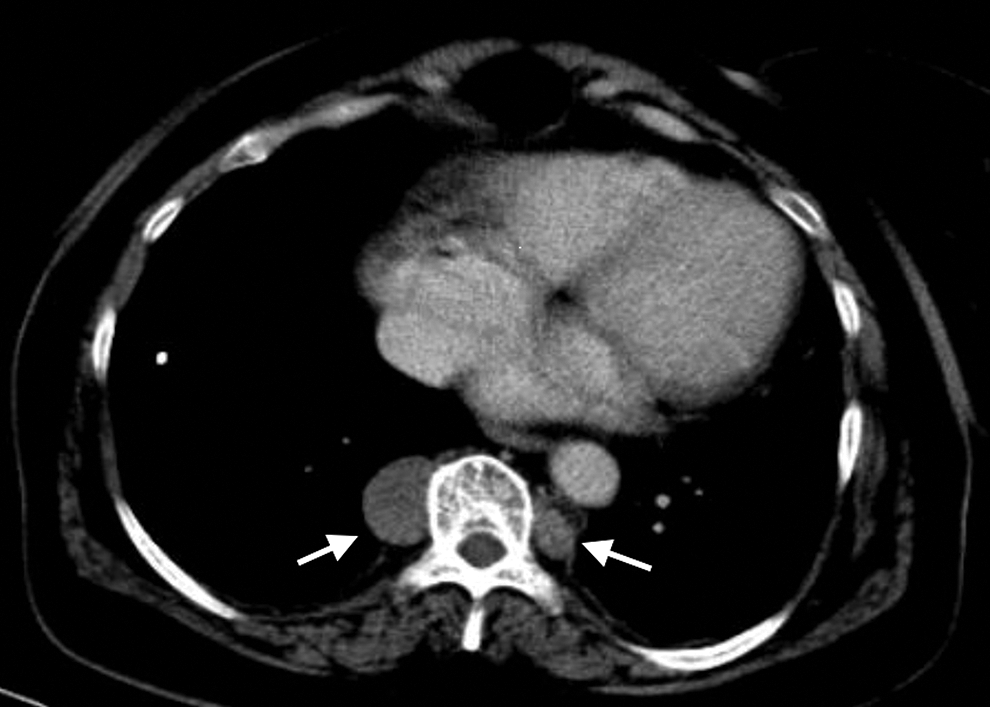
Axial view of computed tomography (CT) thorax shows dilated bilateral azygos veins (marked by white arrow) at the paravertebral region with the right being larger than the left.
A heterogeneous spectrum of jugular bulb deformities can be detected incidentally up to 8% on radiological imaging. 1 In a majority of cases, the patients will remain symptom-free. Uncommonly, some may experience pulsatile tinnitus. A jugular diverticulum represents a rare occurrence characterized by an outpouching from the jugular bulb. The turbulent venous flow resulting from hypertension is postulated to have contributed to a weakened jugular vessel wall, giving rise to an elevated jugular bulb. 2 Rarely, jugular bulb diverticulum may constitute a focal disease or local manifestation of systemic diseases such as Ehler-Danlos and Marfan syndrome. 3 Besides pulsatile tinnitus, the mechanical hindrance of the diverticulum within the middle ear cavity may contribute to conductive hearing loss. The endolymphatic duct may be at risk if the inner ear structures are affected, giving rise to Ménière’s syndrome with episodic vertigo and fluctuating hearing loss. 4,5 Recurrent facial nerve palsy in a case of jugular bulb diverticulum has also been reported. 6
Other differentials of a pulsatile reddish mass medial to an intact tympanic membrane may include neoplasms such as an adenoma, hemangioma, or glomus tumor. Therefore, radiological imaging is essential to evaluate the characteristic of the lesion, its extension and to facilitate surgical planning. In a case of a jugular diverticulum, HRCT of the temporal bone may reveal outpouching of the jugular bulb with focal bony erosion. Magnetic resonance imaging and digital subtraction angiography are more specific and provide a detailed diagnostic assessment. 5 Magnetic resonance imaging of the thorax and brain may be warranted in a clinically suspected systemic aneurysm. The management of a jugular bulb diverticulum should be tailored accordingly to the individual. The treatment goal is to restore the laminar blood flow in the affected venous system. Hearing rehabilitation with hearing aids may be offered as part of the conservative management. 6 Medical control of underlying hypertension also aids to alleviate tinnitus. The surgical interventions include mastoidectomy with compression of the jugular diverticulum or endovascular stenting of the aneurysm. 1,4
The jugular bulb diverticulum represents an unusual etiology of pulsatile tinnitus. Clinical assessment may reveal a reddish pulsatile mass within the middle ear cavity, indifferent from a middle ear tumor’s manifestation. A detailed evaluation of radiological imaging remained paramount to facilitate further management. Ear picking should be avoided at all causes to prevent catastrophic bleeding.
Footnotes
Authors’ Note
All the authors have participated sufficiently in the conception and design of the work, in the analysis of the data and in writing the manuscript to take public responsibility for it. Written informed consent was obtained from the patient for publication of the article and accompanying images. Consent was obtained from the subject of the case for publication of his/her clinical data and photography.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.