
Abstract
Middle ear adenomatous neuroendocrine tumors (MEANT) are rare, mainly benign neoplasms and account for less than 2% of the middle and inner ear neoplasms. There are no specific radiological or clinical findings; therefore, the diagnosis is often difficult. Biopsy prior to surgery is often proposed. The definite treatment is the complete surgical resection. We present an uncommon clinical report of a MEANT, which was treated successfully with surgical excision.
Case Description
A 43-year-old man was referred to our ear, nose, and throat (ENT) outpatient clinic with a 6-month history of progressive left hearing loss and ear fullness. His personal and family medical history were unremarkable. Otomicroscopy revealed an ear mass filling the left external auditory canal. Due to the volume of the mass, it was not possible to clarify its starting point or to visualize the tympanic membrane. Both the Weber and Rinne tests indicated conductive hearing loss on the affected side. Audiometry confirmed conductive mild hearing loss at low and middle frequencies and moderate hearing loss at high frequencies on the left side. The rest of the ENT clinical examination was normal. A contrast-enhanced computed tomography (CT) scan was performed revealing a soft tissue mass arising from the middle ear, extending into the external auditory canal (Figure 1). The mass localized into the middle ear with extent to the attic, pushing and dislocating the ossicles, without affecting the medial wall and promontory. A biopsy of the visible mass was taken under local anesthesia after the CT scan. The mass was quite hemorrhagic and adrenaline–xylocaine solution was required. Histopathology and immunochemistry showed a middle ear adenomatous neuroendocrine tumor (MEANT).
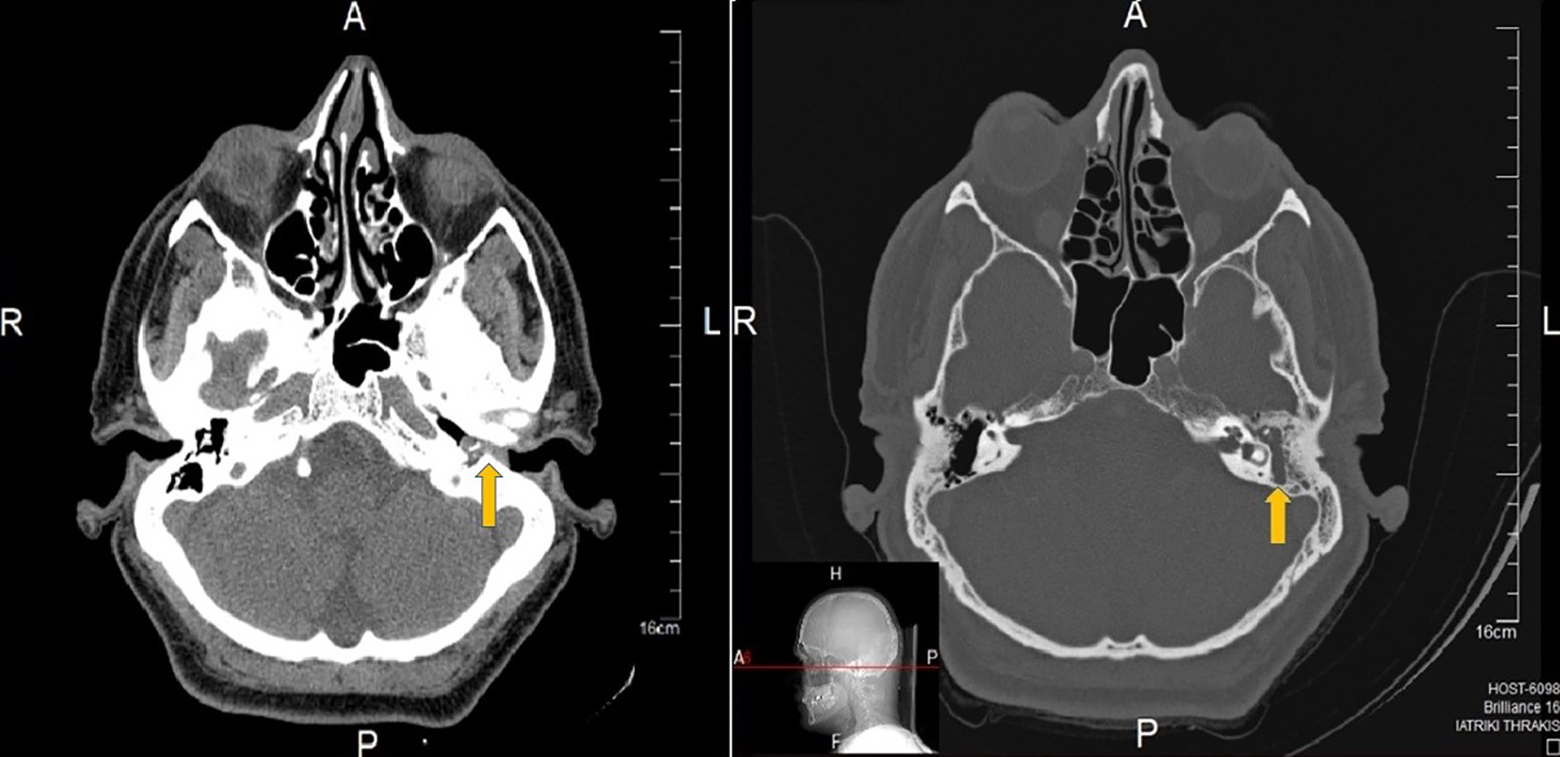
Axial CT images of temporal bones showing the mass filling the middle ear cavity, extending to the external auditory canal (yellow arrows). CT indicates computed tomography.
The treatment plan included an exploratory tympanotomy and a complete surgical excision of the mass under general anesthesia. Finally, a tympanotomy and atticoantrotomy were performed to completely excise the tumor. During the procedure, it was found that incus was disarticulated from both malleus and stapes. However, the preoperative gap between air and bone conduction was not big, probably due to the existing mass. After the removal of the mass, a tympanoplasty type III was performed using a chondral–perichondrial graft from tragus. Histopathological and immunohistochemical examinations confirmed the mixed adenomatous and neuroendocrine differentiation of the tumor (Figure 2).
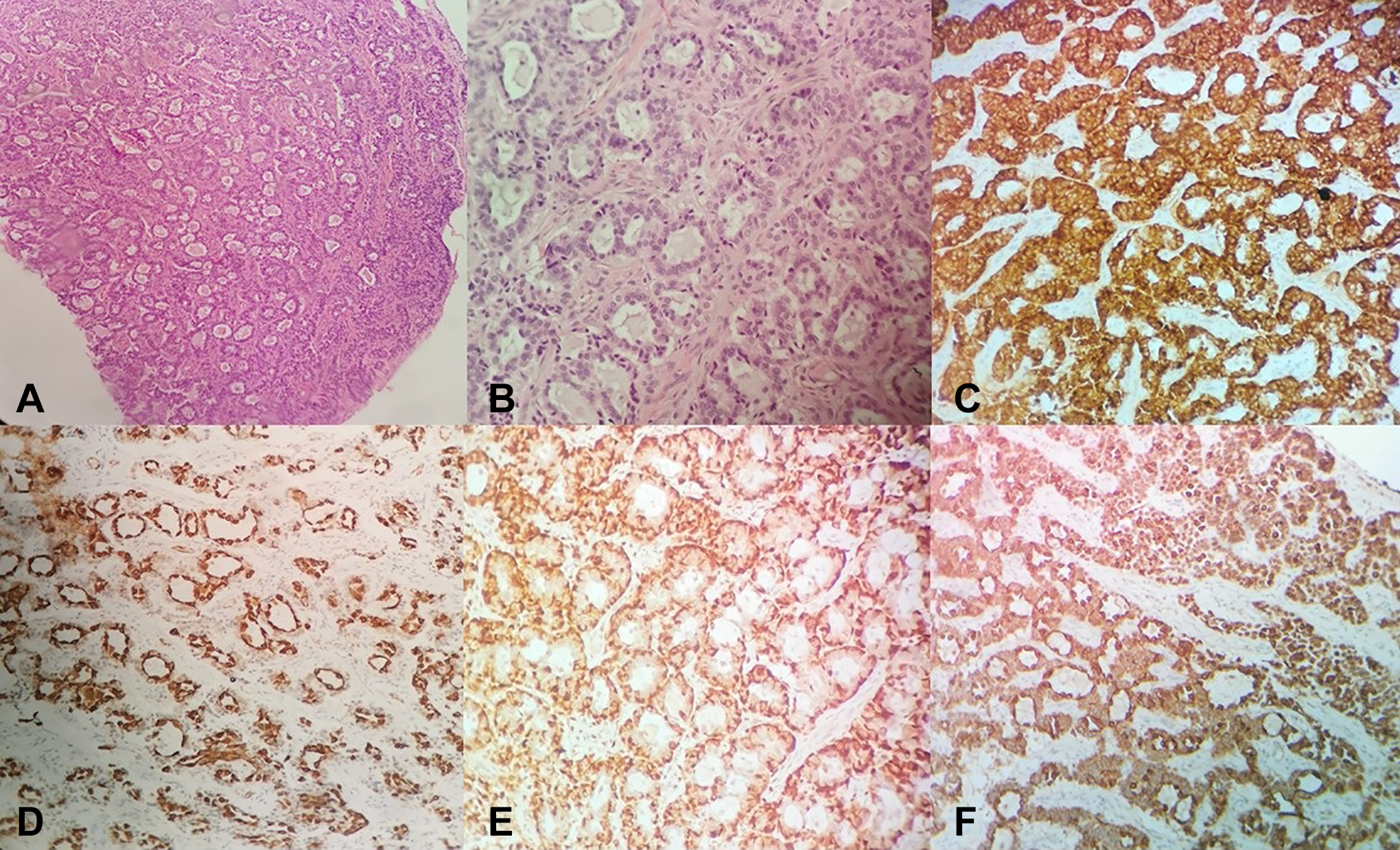
Histopathological and immunohistochemical examinations. (A) Neoplastic cells are organized to great extent in crowded glandular formations, while surrounding stroma is characterized by fibrosis and hyalinosis (H&E, ×20), (B) neoplastic cells in forming 2 lines (H&E, ×40), (C) synaptophysin +, (D) keratin 7 in luminal cells +, (E) p63 in basal cells +, (F) pankeratin +. H&E indicates hematoxylin and eosin.
Octreoscan was performed after the histopathology results, and no local or distant metastases were described. The patient was classified as T2cN0M0S0, using the Tumor, Node, Metastasis, Secretory tumor (TNMS) staging system for adenomatous neuroendocrine tumors of the middle ear. 1 The immediate postoperative as well as the 3-month follow-up period was without complications. One year postoperatively, clinical examination and magnetic resonance imaging (MRI) of temporal bones did not reveal any evidence of recurrence or metastases of the tumor.
Discussion
Middle ear adenomatous neuroendocrine tumors are extremely rare (less than 2% of middle and inner ear neoplasms), mainly with benign characteristics. 2 They derive from the glandular components of middle ear and they differentiate into glandular, neuroendocrine, or both directions. 3 Concerning epidemiology, there is not a specific decade of onset, while there is not male or female predominance. 4 It is still under investigation whether MEANTs and carcinoid tumors are separate diseases or expression of the same entity.
The most frequent symptoms are hearing loss, ear fullness, tinnitus, and/or ear pain. 4 As MEANT is a rare clinical entity with nonspecific symptoms, it is not a first-line diagnosis. Differential diagnosis includes clinical entities that present as ear masses with progressive hearing loss, such as middle ear otitis and cholesteatoma, schwannoma, glomus tumor, encephalocele, pleomorphic adenoma, or adenocystic carcinoma. 5
Screening tests are demanded in order to examine hearing, middle ear status (eg, ossicles and mastoid process condition), the presence or not of vascular components in the tumor or its relation to brain. Computed tomography scan is carried out more often, while MRI is also used. Due to its relationship with carcinoid tumors, it is proposed to perform scintigraphy with octreotide, an analogue to somatostatin whose receptors have been found in similar tumors. 6
High clinical suspicion is recommended, while most surgeons prior to the main surgical procedure perform biopsy in order to reach diagnosis. 4 Complete surgical resection is the treatment of choice. Most patients undergo tympanomastoidectomy with microsurgical removal of the tumor, when epitympanium, external auditory canal, or mastoid are involved. When there is adhesion to the ossicles, they are removed, and the chain is reconstructed when it is necessary. For tumors with no involvement of other structures that are limited in the mesotympanum, transcanal surgical approach is preferred. 5 Radiotherapy has been used for metastases, while chemotherapy is not recommended in current literature. 4,7 As cases with aggressive tumor behavior or even malignancy, with or without metastases, have been described, a staging system for more accurate diagnosis and treatment was proposed by Marinelli et al. 1 Systematic follow-up is recommended in order to exclude recurrence.
Footnotes
Authors’ Note
The authors declare that written informed consent for patient information and images to be published was provided by the patient.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.