
Abstract
Significance Statement
Pharyngeal fistulas to the cervical spine resulting in vertebral osteomyelitis are a rare, yet clinically important, complication of total laryngectomy performed in conjunction with chemoradiotherapy or radiation therapy. This complication is likely underdiagnosed and can have a high mortality rate. It is very important that clinicians are aware of this complication as early diagnosis and management may improve patient outcomes.
Case Presentation
A 79-year-old male presented with a chief complaint of blood at his tracheostomy site for one day. He had a history of supraglottic squamous cell carcinoma treated with radiation therapy, salvage total laryngectomy, lymph node dissection, and pharyngeal reconstruction that was complicated by a benign cervicoesophageal stricture requiring percutaneous endoscopic gastrostomy (PEG) feeding. Direct laryngoscopy showed blood clots in the neopharynx. Esophagogastroduodenoscopy showed a pharyngeal fistula with a protruding bony fragment and active oozing (Figure 1) proximal to a benign-appearing intrinsic severe stenosis, 15 cm from the incisors. Biopsy of the fistula site showed active mucositis and necrotic bone with adjacent mixed inflammation and bacterial colonies (Figure 2). A magnetic resonance imaging short tau inversion recovery image of the spine showed a hyperintense tract extending from the pharynx to the C3-C4 disk space with hyperintensity of the adjacent C3 and C4 vertebral bodies (Figure 3). The patient was started on broad-spectrum antibiotics for osteomyelitis. Surgical correction of the pharyngeal fistula was deferred due to poor functional status. After antibiotic therapy, PEG-guided feeding, and rehabilitation, the fistula was surgically repaired by a left pectoralis major myocutaneous flap reconstruction. He also underwent C3-C4 cervical arthrodesis for cervical instability. The patient’s bleeding resolved after surgical correction.
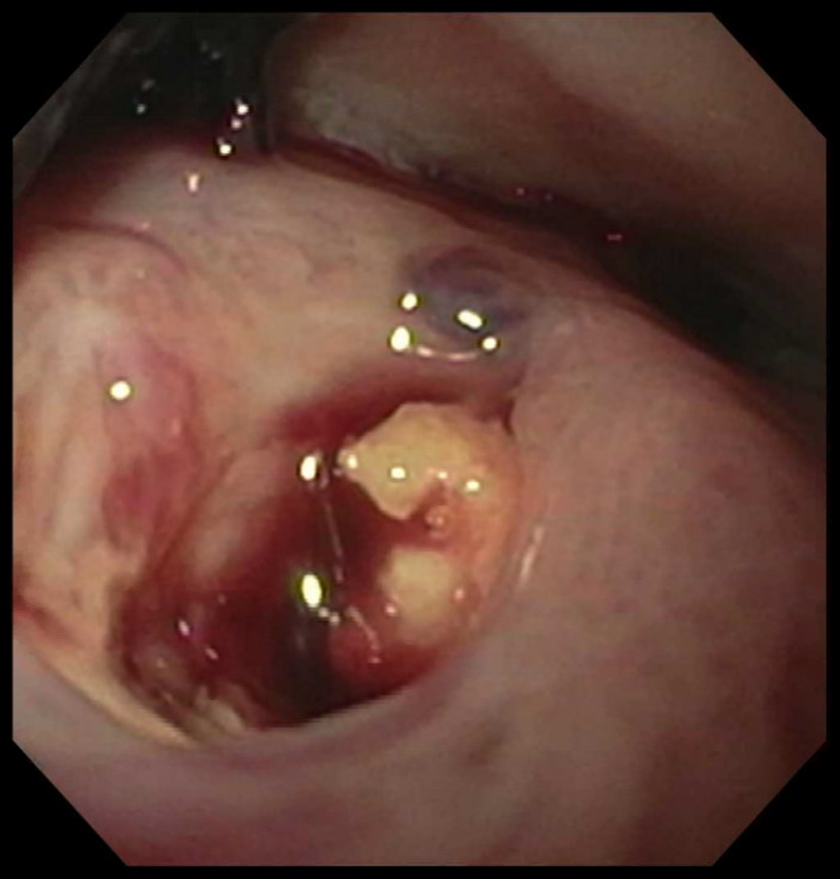
A pharyngeal fistula with a protruding bony fragment and active oozing.
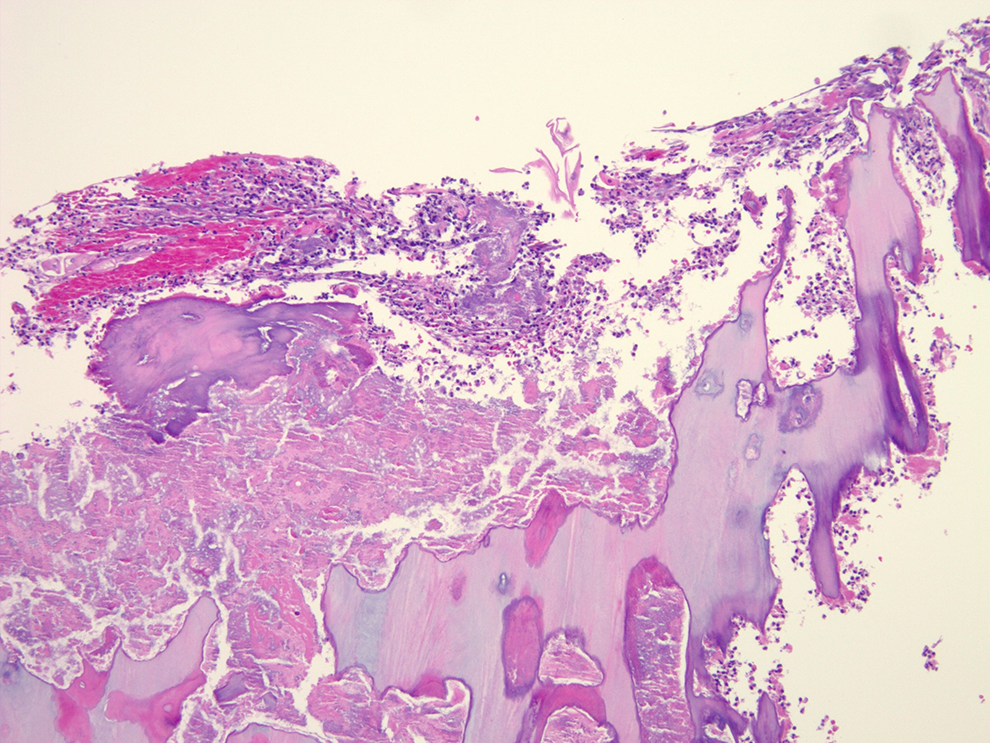
A biopsy showing necrotic bone with adjacent mixed inflammation and bacterial colonies.
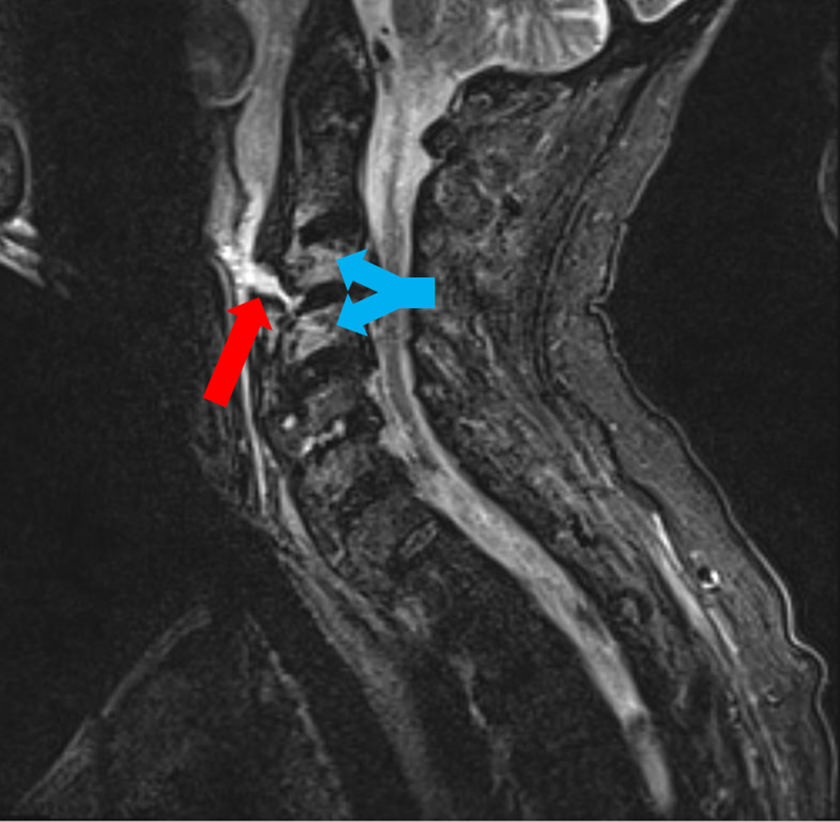
A magnetic resonance imaging (MRI) short tau inversion recovery (STIR) image demonstrating a hyperintense tract (red arrow) extending from the pharynx directly to the C3-C4 disk space with adjacent C3 and C4 vertebral body hyperintensity (blue arrows) consistent with osteomyelitis.
Discussion
Pharyngeal fistulas commonly occur following salvage total laryngectomy. Following total laryngectomy with radiation therapy, pharyngocutaneous fistulas (PCFs) developed in 15% of patients in one study. 1 Pharyngocutaneous fistulas negatively affect wound healing, nutrition, length of hospitalization, and quality of life. 2 Although PCFs are relatively common, this case describes a pharyngeal fistula communicating with the cervical spine resulting in osteomyelitis. There are limited reports of cervical vertebral osteomyelitis following treatment of pharyngeal carcinoma with laryngectomy in conjunction with chemoradiotherapy or radiation therapy. 3 This complication is likely underdiagnosed and has a mortality rate of up to 40%. 3 In a case series of 10 patients with osteomyelitis from a pharyngeal cervical spine fistula, 90% of patients had a neurologic deficit at the time of diagnosis. 3 Cervical pain was often the first presenting symptom and was present in 70% of patients at diagnosis. 3
In a patient with a history of laryngectomy, symptoms of cervical pain, fever, or neurologic symptoms should raise suspicion for cervical spine osteomyelitis. 3 Imaging studies and bone biopsy should be performed to confirm the diagnosis and to obtain microbial culture data. 3 Once the diagnosis is confirmed, patients should be treated with systemic antibiotics and surgery to close the defect and stabilize the cervical spine. 3 Although endoscopic images of PCFs have been previously reported in the literature, to our knowledge, this is the first report to include endoscopic images of a pharyngeal fistula with direct communication to the cervical spine. 4
Footnotes
Authors’ Note
The patient detailed in this report is deceased. Informed consent was obtained from the patient’s spouse for publication of his information and imaging. All identifying patient information has been removed.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.