
Abstract
Objectives:
The total laryngectomy is one of the most standardized major surgical procedures in otolaryngology. Several studies have proposed the Clavien-Dindo classification (CDC) as a solution to classifying postoperative complications into 5 grades from less severe to severe. Yet more data on classifying larger patient populations undergoing major otolaryngologic surgery according to the CDC are needed. Predicting postoperative complications in clinical practice is often subject to generalized clinical scoring systems with uncertain predictive abilities for otolaryngologic surgery. Machine learning offers methods to predict postoperative complications based on data obtained prior to surgery.
Methods:
We included all patients (N = 148) who underwent a total laryngectomy after diagnosis of squamous cell carcinoma at our institution. A univariate and multivariate logistic regression analysis of multiple complex risk factors was performed, and patients were grouped into severe postoperative complications (CDC ≥ 4) and less severe complications. Four different commonly used machine learning algorithms were trained on the dataset. The best model was selected to predict postoperative complications on the complete dataset.
Results:
Univariate analysis showed that the most significant predictors for postoperative complications were the Charlson Comorbidity Index (CCI) and whether reconstruction was performed intraoperatively. A multivariate analysis showed that the CCI and reconstruction remained significant. The commonly used AdaBoost algorithm achieved the highest area under the curve with 0.77 with high positive and negative predictive values in subsequent analysis.
Conclusions:
This study shows that postoperative complications can be classified according to the CDC with the CCI being a useful screening tool to predict patients at risk for postoperative complications. We provide evidence that could help identify single patients at risk for complications and customize treatment accordingly which could finally lead to a custom approach for every patient. We also suggest that there is no increase in complications with patients of higher age.
Keywords
Introduction
Head and neck cancers are the seventh most common malignant tumors globally. 1 The majority of head and neck cancers are squamous cell carcinomas, and the global incidence of all subtypes of head and neck cancers has been growing in recent years. 2 The risk factors for all subtypes of head and neck cancers are well established, with tobacco and alcohol use, as well as certain subtypes of the human papillomavirus, being the most important. 3,4 Regional differences in the incidence of different subtypes of head and neck cancers exist, which seem to be related to differences in the occurrence of preventable riskfactors. 5,6
The larynx is anatomically subdivided into 3 different structures: supraglottic, glottic, and infraglottic. 7 Total laryngectomy is the treatment of choice for locally advanced laryngeal cancer in which a surgical resection seems possible. Organ preservation approaches are available, yet they seem to be less effective in achieving disease-free survival. 8 Although laryngeal cancers are ranked 18th of the most prevalent cancers worldwide, 1 the morbidity of treatment is significant and surgical decision-making challenging, inherent to the often invasive nature and the involvement of surrounding anatomic structures. 9
The workload for head and neck surgeons is substantial and will increase due to the aging population of the western civilization. 10 Therefore, with increasing cost pressure in the health care system, the reduction in postoperative complications is also essential importance. Comorbidities leading to a higher risk for specific complications in otolaryngologic surgical procedures have been analyzed sufficiently. 11 -14 Several studies show what types of complications to expect after total laryngectomy as either first treatment or as salvage operation. 15 -17 Common complications are pharyngocutaneous fistulas, postoperative bleeding, and insufficiency of the voice prosthesis. Complications and complication rates are not described uniformly in the literature. There is a lack of comparability of studies, for example, to identify and characterize groups with a higher risk of complication. Therefore, studies are needed to prepare the data in a standardized way.
The Clavien-Dindo classification (CDC) is a method to uniformly classify surgical complications in a way that is internationally recognized. It has been established as leading method for classifying postoperative complications in recent years. 17,18
Predicting postoperative complications is often based on established clinical tools and expert opinion. The most commonly used scoring systems generalize and neglect the variety of surgical disciplines, as well as the variety in surgeries within a discipline. Machine learning is a subfield of artificial intelligence and has been reintroduced in recent years as a method to make predictions based on the characteristics of individual patient groups in various clinical settings. 19 -21 A variety of machine learning algorithms has been proposed, yet the choice of the best algorithm is usually highly dependent on the patient characteristics in the dataset.
Our study aims at analyzing known comorbidities for complications after total laryngectomy by grading them according to the CDC. We hope that linking the risk factors to a uniform grading system and predicting postoperative complications using machine learning will ultimately lead to better identification of high-risk patients and to a more patient-tailored approach in choosing the right treatment.
Patients and Methods
Patients
All patients who underwent a total laryngectomy at our institution, a large university medical center, between January 01, 2010, and December 31, 2018, were included. We are one of the largest tertiary referral hospitals in central Europe. Data were obtained from the Comprehensive Cancer Center (CCC) from all 3 hospital locations. Approval by the Ethical Commission was granted before the start of the data collection (EA1/059/19). The analysis was performed retrospectively. Patients with histology other than squamous cell carcinoma were excluded.
Clinical Variables
All clinical data were obtained through the electronic health records (EHRs) in the hospital. The EHR started a comprehensive data collection as of 2010. Therefore, making it the starting point for our study. Collected data included sex, age, tumor localization, tumor differentiation (well, moderate, poor), TNM staging system, R-status, body mass index (BMI), American Society of Anesthesiologists (ASA) classification, information about previous therapy methods (including pre-irradiation), and history of tumor recurrence. The surgical report was reviewed for the length of procedure and whether intraoperative reconstruction was performed with tissue transfer methods. Information about adjuvant treatment was obtained by screening the physician letters written at discharge and additionally by reviewing the report of the CCC. Visits to our outpatient department were screened as well. All postoperative complications with procedure-specific complications occurring within 30 days after procedure were included.
Perioperative Procedures
Laryngectomy was performed according to current standards with the removal of the hyoid bone and the infrahyoidal muscles. Two suction drains were inserted at the end of the surgery. Routine perioperative antibiotic prophylaxis with ampicillin/sulbactam or cefuroxime and metronidazole was given until 7 to 10 days postoperatively. During surgery, a nasogastric tube was inserted and remained there for 7 to 10 days. After removal of the nasogastric tube, a feeding test was performed, a visual check for pharyngoesophageal insufficiency was done. The following day, blood tests to assess whether surgical site infection or mediastinitis would develop were performed.
After surgery, the patient remained in the intensive care unit (ICU) for 24 hours except when the surgeon decided against postoperative ICU surveillance. Standard of care included anticoagulation with low-molecular-weight heparins after surgery for the duration of the stay of the patient. Blood samples for CRP, small blood count, and creatinine were obtained every other day.
Reconstruction was performed after decision was made by either the local CCC or the consultant head and neck surgeon. Choice of reconstructive procedure was with performing by the surgeon. Reconstruction is performed when substantial defects due to big tumors are expected or patients deemed to be high risk sustaining postoperative complications. Jejunal interpositional grafting is performed in rare cases in which large segments of the esophagus needed to be removed surgically by our team.
Comorbidity
Comorbidity was assessed by using the Charlson Comorbidity Index (CCI), 22 which is clinically validated and acquires information about preoperative conditions. A score between 0 and 33 gives an estimation of the 10-year survival prognosis of a patient. The system has been proposed in 2004 and is progressively implemented into clinical practice. 23
Complications were graded according to the CDC with scores between I (any deviation from the normal postoperative course) and V (death of a patient). Patients with CDC IV or higher were those with severe postoperative complications in need of treatment in the ICU. All other patients either had no complications or minor to moderate deviations from clinical practice. The aim of this study is to analyze whether certain risk factors and comorbidity scores make patients more prone to develop a severe postoperative complication (CDC ≥ IV) and to build a machine learning model predicting these uniformly classified high-grade complications.
Statistical Analysis and Development of Machine Learning Algorithm
Baseline values were analyzed by descriptive statistics or absolute numbers with percentage points and standard deviation where applicable. Univariate binary logistic regression analysis of the different variables was performed. Significant results of the univariate analysis were used for multivariate analysis. All results were analyzed by making use of the statistical software package SPSS Version 25. Significant results of the analysis were used to build a machine learning model to predict postoperative complications. We made use of the graphic user interface to the R Programming language, RStudio (Version 1.2.5042). Data were split into different training and testing datasets using 5-fold cross-validation, and a reusable train control object for all models was built using the caret package to ensure all models were build based on the same training and testing data. Four different machine learning models, 2 logistic regression models (generalized linear model (glm) for binary outcomes and glmnet) and 2 tree-based models (AdaBoost and gradient boosting machine) were compared based on the area under the curve (AUC). No custom tuning of the models was performed as the tuning parameters embedded in the models were deemed sufficient. The best model was fitted onto the complete dataset to obtain sensitivity, specificity, positive, and negative predictive values.
Results
Demographics
In total, 4880 new patients with head and neck cancer were treated between January 01, 2010, and December 31, 2018, at the Charité – Universitätsmedizin Berlin. Of these, 850 had newly diagnosed laryngeal SCC; 148 of the 850 patients with laryngeal SCC were treated with total laryngectomy.
All demographics of patients included are listed in Table 1. Most patients were male with a mean age of 64 years. The most common tumor grade was T4a and occurred in the larynx. The majority of patients did not have a lymph node metastasis at pathological examination. The majority of patients were ASA stage 2 and 3 with 62 and 69, respectively, while the mean CCI score was 4.8. Reconstruction using pedicled flaps or free tissue transfer was performed in 21 cases. Used flaps were pectoralis major flap (11 cases), free radial forearm flap (4 cases), supraclavicular artery island flap (1 case), jejunal graft interposition after esophagectomy (2 cases), and local tissue transfer (4 cases). In some cases, 2 flaps were used, each flap was counted separately.
Demographics of the Study Population.
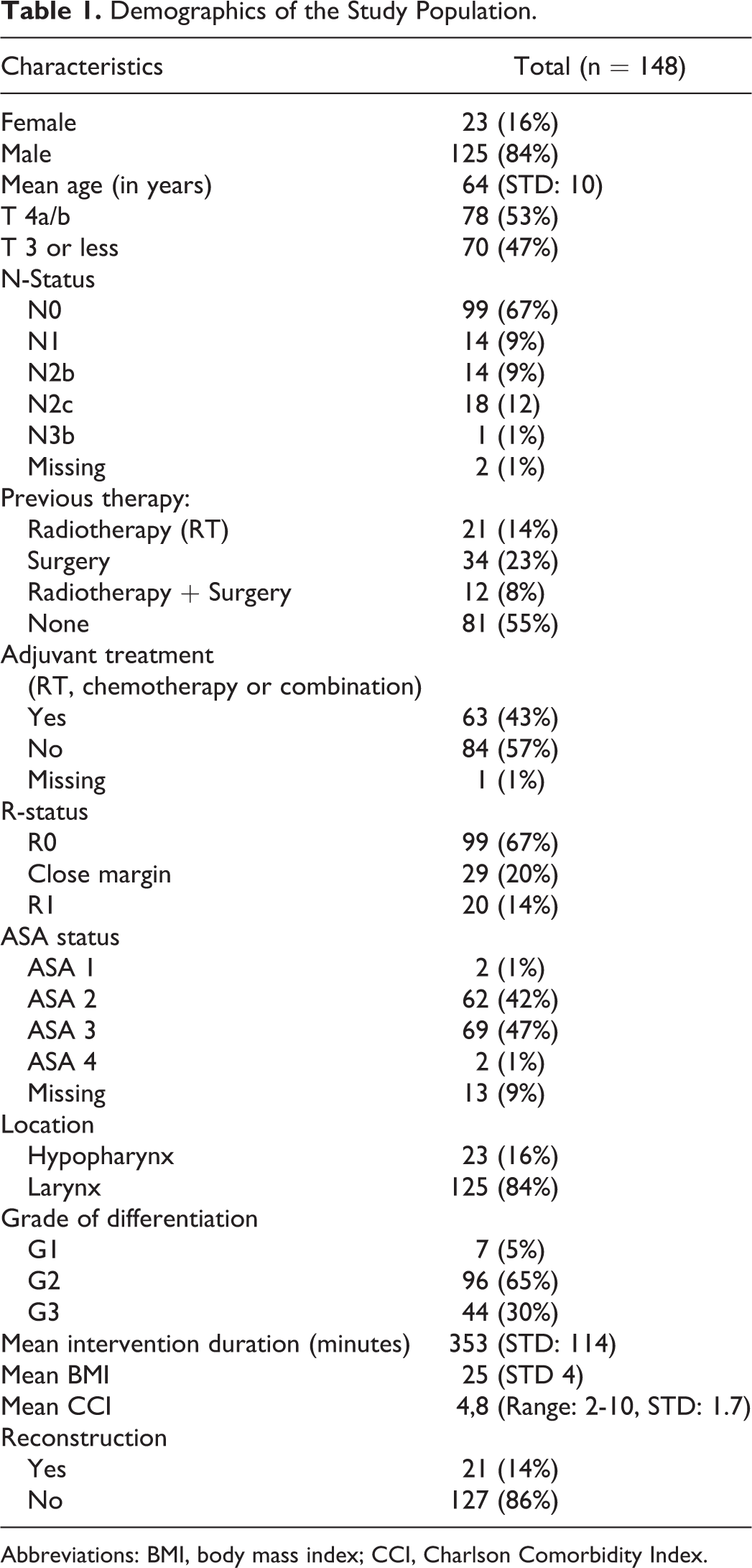
Abbreviations: BMI, body mass index; CCI, Charlson Comorbidity Index.
Patients receiving reconstruction were more likely to have had previous radiotherapy with 12 (57%) cases, compared to 22 (17%) cases in the group of patients without reconstruction. Also, patients receiving reconstructing were slightly more likely to have a T4 carcinoma with 12 (57%) cases compared to 65 (51%) cases.
Perioperative Parameters
The mean intervention duration was 353 minutes (STD: 114) and the mean length of stay was 16.8 days (STD: 10.3; Table 1).
Complications
One (0.7%) patient died after surgery due to myocardial infarction after fulminant lung artery embolism. In total, there were 48 (28%) grade III and IV complications, 21 (14.2%) CDC grade IV complications, 26 (17.5%) were grade I complications, and another 26 (17.5%) were grade II complications (Table 2).
Complications During the First 30 Days After TL for All Patients With CDC ≥ 3.
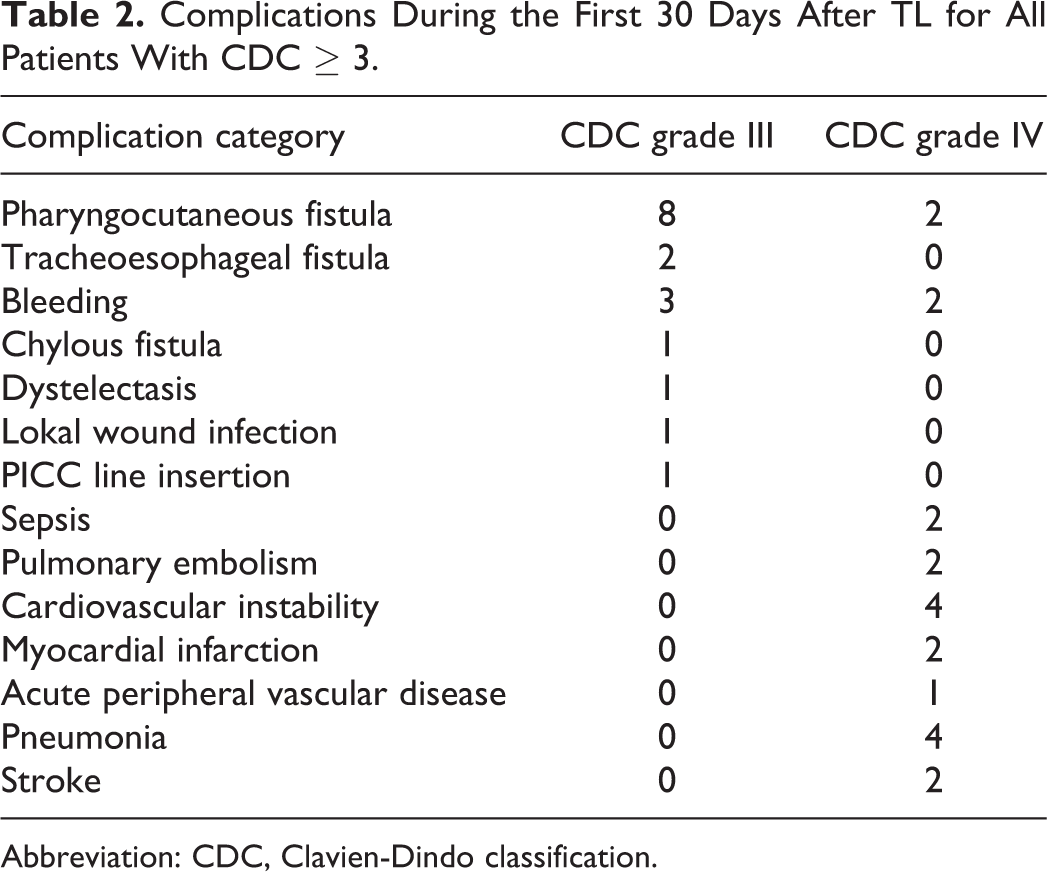
Abbreviation: CDC, Clavien-Dindo classification.
Univariate Logistic Regression
The univariate analysis showed that the CCI and reconstruction after laryngectomy to be predictors of postoperative complications with odds ratios of 1.907 and 3.733, respectively. Previous surgery and radiotherapy, a certain sex, the BMI, operation time, age, and recurrence did not achieve significance (Table 3).
Univariate Logistic Regression With Estimation of an Odds Ratio for All Patients With Serious Adverse Events CDC ≥ 4.
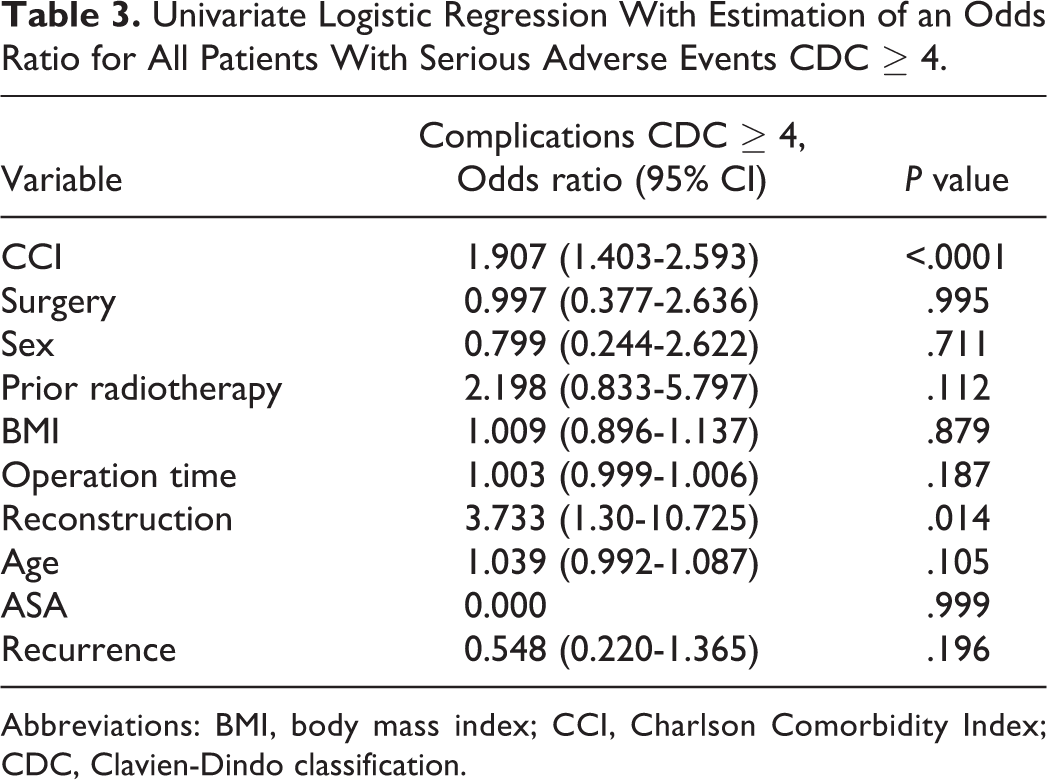
Abbreviations: BMI, body mass index; CCI, Charlson Comorbidity Index; CDC, Clavien-Dindo classification.
Multivariate Logistic Regression
Multivariate analysis showed a significantly increased risk of high-grade complications (CDC score ≥ 4) with increasing CCI scores resulting in an odds ratio of 2.002. Surgical reconstruction of tissue defects also led to a significant increase in CDC ≥ 4 complications with an odds ratio of 5.782 albeit in a small patient sample of 21 patients (Table 4).
Multivariate Logistic Regression of Significant Risk Factors in Univariate Analysis With Estimation of an Odds Ratio for Serious Adverse Events (CDC ≥ 4).
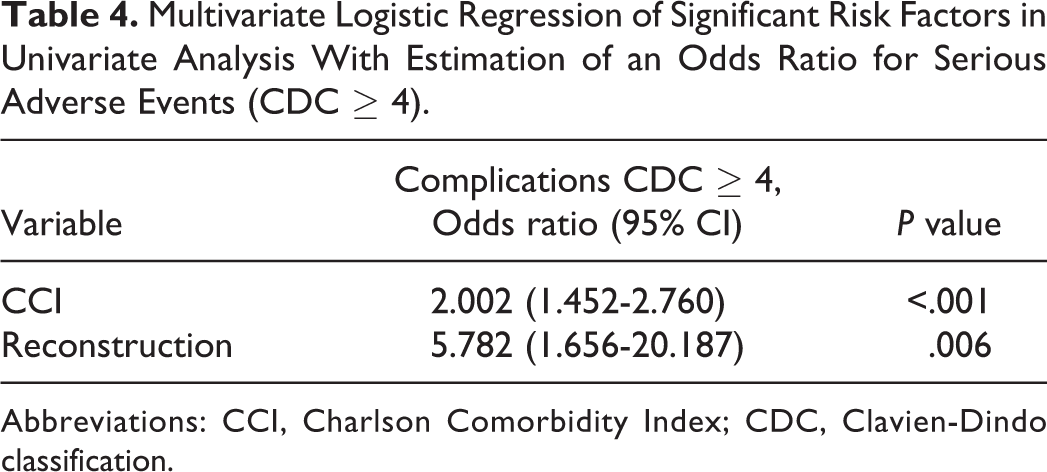
Abbreviations: CCI, Charlson Comorbidity Index; CDC, Clavien-Dindo classification.
Model Comparison
All models had good predictive properties with an AUC above 0.7. The 2 models with the highest AUC were AdaBoost (0.769) and glmnet (0.766). Accordingly, the AdaBoost model with the highest AUC was chosen for further analysis on the dataset.
The Adaboost Model
Fitting the AdaBoost model on the complete dataset yielded an accuracy of 89%, with a sensitivity of 32% and a specificity of 99%. A positive predictive value of 88% and a negative predictive value of 89% were found. Accordingly, our model was able to predict 7 complications correctly (Table 5). This is one person more correctly classified than by the logistic regression model in our SPSS output; 125 persons were correctly classified as sustaining no complications. A total of 16 persons were wrongly classified resulting in an overall accuracy score of 89.19%. In the logistic regression model, sensitivity was lower due to the fact that only 6 patients were correctly classified as sustaining a complication in contrast to the 7 correctly predicted complications of AdaBoost algorithm.
Confusion Matrix of the Results of the Adaboost Model After Prediction on the Complete Dataset With 148 Patients.
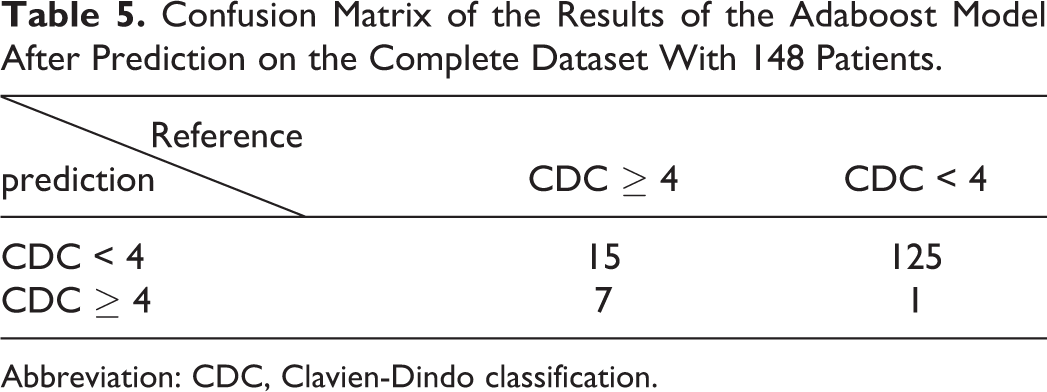
Abbreviation: CDC, Clavien-Dindo classification.
Discussion
After years of using the CDC for postoperative complications in other surgical fields, it has emerged as a method to uniformly classify postoperative complications in an internationally accepted way. 18 Although previous studies have researched the association between risk factors and postoperative complications, the total number of patients included have been less or the studies focused their assessment on different risk factors. 17,24,25
Although minor complications can be managed by routine care, major complications need to be addressed differently. A thorough screening process might help to identify patients prone to postoperative complications, which may help caregivers to focus more on certain patients.
Of the different risk factors analyzed, the CCI and whether reconstruction was performed were significant. Every point of increase in the CCI led to a 1.9-fold increase in the risk of having a CDC IV or higher complication. As the CCI is already in routine use, it is an easy-to-implement scoring system. Ten-year survival is estimated by an incremental score for each comorbidity. Recent studies have used the CCI as well as the modified frailty index to assess comorbidity. 17,25 We find the CCI best suited because of an easy scoring system that is readily available on many online sources. Also, the modified frailty index, which is used in other studies, often assesses similar conditions as the CCI with a comparable scoring system. 25 -27
Patients who underwent a reconstructive procedure with tissue transfer showed a markedly increase in severe postoperative complications. Albeit this group was relatively small the results achieved significance. Although the teams that performed these types of surgery are usually more experienced, patients who received a reconstruction often had more extensive tumors and more often received salvage surgery, therefore, having a higher risk of developing complications.
There has been conflicting research about the implication of doing surgery on patients of higher age. Our study did not seem to support the hypothesis that increasing age leads to the occurrence of more postoperative complications, which is supported by some studies, 17 yet disputed by others. 24,28 Radiotherapy, which has been a well-known risk factor for postoperative complications, did not achieve significance. 29 This may be partly due to the relatively small study size with 33 (22%) patients who underwent the previous radiotherapy, since an odds ratio of almost 2.2 suggests an increased risk for complications yet not achieving statistical significance.
Machine learning has reemerged in recent years due to the change in digital infrastructure, the availability of digital clinical data, and the number of skilled personnel. Numerous applications in machine learning in the clinical setting have emerged in various clinical specialties, otolaryngology being one of them. Our research shows that machine learning has not been applied to predict postoperative complications in a patient group solely undergoing a laryngectomy to date. The algorithms developed using machine learning have good predictive abilities with an AUC of 0.77 in patients of this subset, even in the presence of a relatively small sample size. The model deployed showed a slightly higher sensitivity than binary logistic regression on the dataset.
Conclusion
Adverse events in modern hospital services occur on a daily basis. The CDC is an opportunity to assess postoperative complications uniformly among surgical specialties worldwide. A uniform approach will lead to higher comparability, which can ultimately contribute to an improvement in the quality of care. Our study shows that a reasonable estimate of postoperative complications can be made using machine learning algorithms. Bigger databases covering various surgeries are needed in order to train more elaborate models and integrate them into the clinical workflow.
Footnotes
Authors’ Note
German Society for Otolaryngology (DGHNO), Summer 2020. Joint European Congress on Head and Neck Oncology (ECHNO) and the International Congress on Innovative Approaches in Head and Neck Oncology, Summer 2021 (Abstract accepted in 2020 and due to COVID moved to 2021).
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: We acknowledge support from the German Research Foundation (DFG) and the Open Access Publication Fund of Charité – Universitätsmedizin Berlin.