
Abstract
Although peripheral facial paralysis and sudden sensorineural hearing loss are not as common as anosmia, they are reported neurological manifestations of severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2). We present a 62-year-old, serologically COVID-19 positive woman with seventh and eighth nerve involvement showed electrophysiologically with Auditory Brainstem Response and electroneurography and radiologically with internal acoustic canal magnetic resonance imaging. This single case report suggests a possible association between the SARS-CoV-2 infection with simultaneous sudden sensorineural hearing loss and isolated facial paralysis. However, further studies are needed to determine whether this relationship is coincidental or occasional.
Introduction
Severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) is a member of the family of coronaviruses, isolated from human airway epithelial cells. This virus transmitted through droplets and direct contact, with an average incubation period of 5 to 7 days. Its main symptoms are fever, fatigue, and a dry cough, often with pulmonary involvement. Other reported symptoms include headache, myalgia, odynophagia, nasal obstruction, runny nose, anosmia, dysgeusia, and gastrointestinal manifestations. 1
Although peripheral facial paralysis and sudden sensorineural hearing loss (SSHL) are not as common as anosmia, they are the neurological manifestations of SARS-CoV-2 reported in an increasing number of cases in the literature. From the beginning of the pandemic to until now, 11 cases of SSHL with a positive SARS-COV-2 reverse transcription polymerase chain reaction (RT-PCR) test were reported from 9 clinics around the world. 2 -10 Likewise, 14 cases of isolated peripheral facial paralyses from 7 clinics with positive RT-PCR test have been published. 11 -17 However, to the best of our knowledge, no COVID-19 patient has been reported in which SSHL and peripheral facial paralysis are seen as the first sign at the same time.
Here, we present a COVID-19 patient with seventh and eighth nerve involvement showed electrophysiologically with auditory brainstem response (ABR) and electroneurography (ENoG) and radiologically with internal acoustic canal (IAC) magnetic resonance imaging (MRI).
Case Report
A 62-year-old woman was admitted to the clinic with left-sided facial weakness that had persisted throughout the day. She had also experienced hearing loss, pain in the left ear, fatigue, chills, and myalgia for 2 days. She visited another health center with these symptoms 2 days ago, and the results of the nasal swab SARS-CoV-2 RT-PCR test were negative. She decided to visit our clinic when the facial paralysis developed; she had no history of otologic disease, hearing loss, or any systemic disease. The patient presented with unilateral House-Brackmann grade VI facial palsy with severe asymmetry on the left side. The ear, nose, and throat examination showed no abnormal findings on both the external auditory canal and the tympanic membranes; there was no vesicle, no otorrhea, or hyperemia on the tympanic drum. The mucosa of the nose and throat were also normal. The audiological examination of her left ear revealed moderate to severe sensorineural hearing loss—more pronounced at higher frequencies—and a type A tympanogram. The patient, whose fatigue persisted despite the absence of a fever and cough, requested a nasal swab test for SARS-CoV-2 RT-PCR. Complete blood count and C-reactive protein tests were performed. The patient received corticosteroid therapy with 1 mg/kg/d oral methylprednisolone, tapered to 16 mg every 3 days (Prednol, Mustafa Nevzat), and 40 mg H2-receptor antagonist, famotidine, administered (Famodin, Sandoz). Precautions were taken to ensure that the patient’s eyes remained hydrated. One day later, the COVID-19 diagnosis was confirmed by the positive RT-PCR test; the patient was immediately started on 200 mg oral Favipiravir tablets, taken twice daily for 5 days, and 40 mg/0.4 mL enoxaparin sodium administered subcutaneously (Clexan, Sanofi Aventis Pharma) per the Health Ministry’s COVID-19 guidelines. This course of treatment was administered concurrently with the corticosteroid treatment.
When the patient arrived after 10 days of treatment and quarantine at home, she presented with unilateral House-Brackmann grade V facial palsy with minimal movement on the left side of the mouth commissure. The audiological examination revealed that her hearing had improved (Figure 1). An ABR test performed on the patient detected a significant elongation in the interaural wave V latency on the left ear, compared to the right (Figure 2). The ENoG test conducted that the compound muscle action potential (CMAP) amplitude recording from the orbicularis oculi and nasalis muscles was 75% lower on the left compared to the right. The CMAP amplitude recording from the orbicularis oris muscle was 60% lower on the left compared to the right. All audiological and electrophysiological test results are summarized in Table 1. The IAC MRI showed enhancement of the seventh and eighth nerves in the T1 sections after contrast injection (Figure 3). When the patient returned for control testing at the end of the first month, we decided that she would continue treatment by starting the physical therapy program and would have repeat MRIs and electrophysiological tests performed at 6 months.
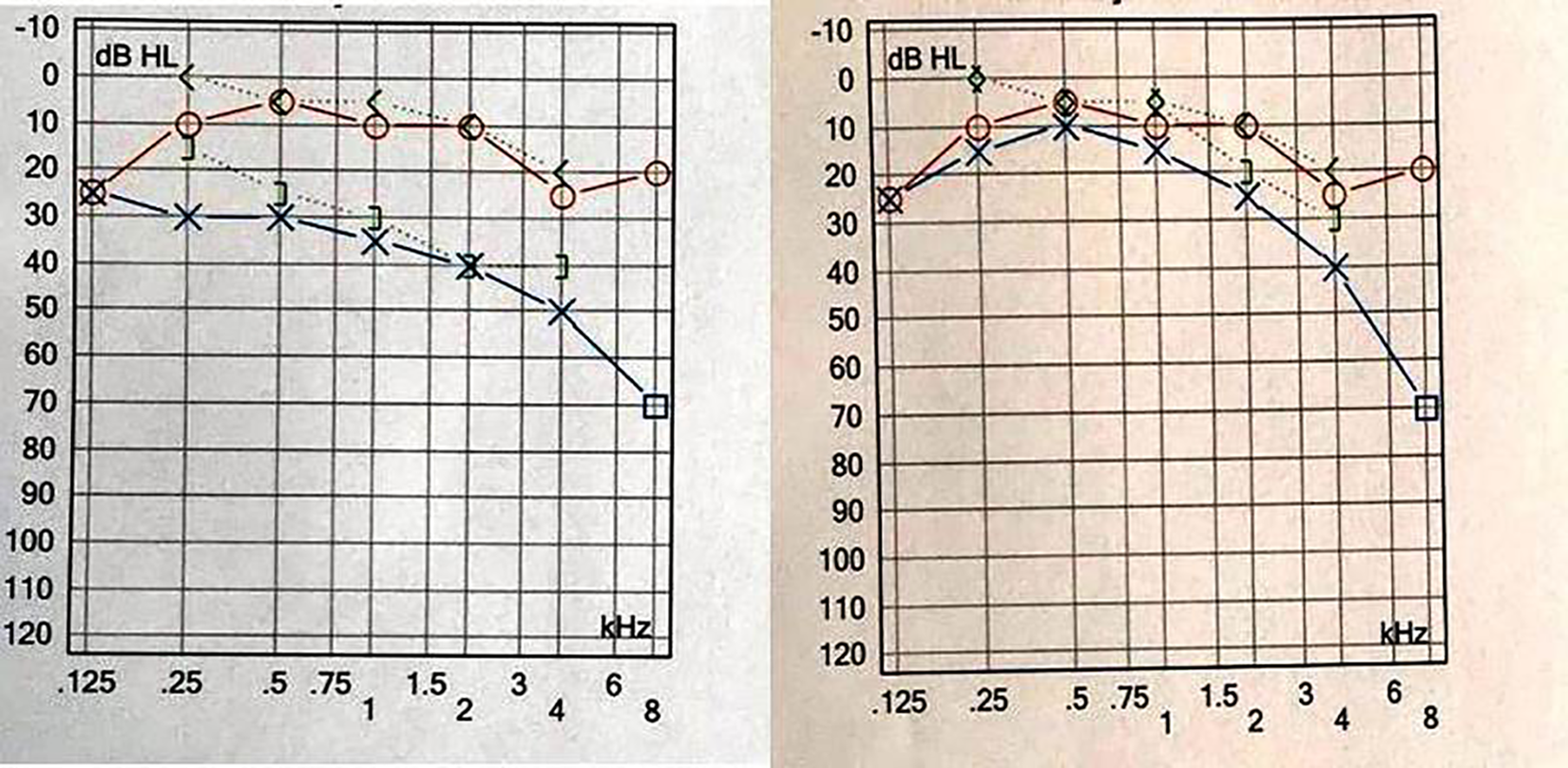
Audiological tests before and after treatment.
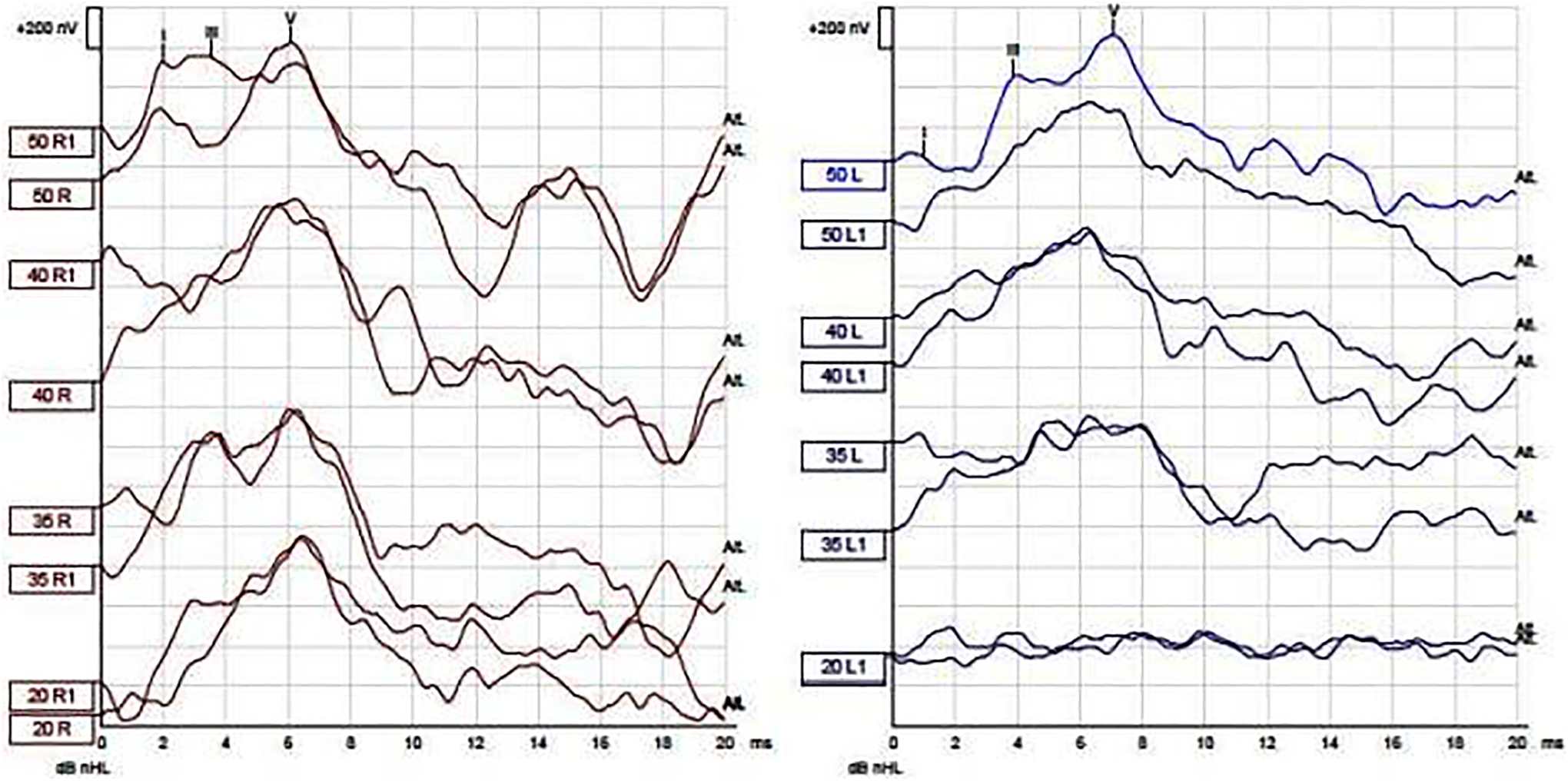
Auditory brainstem response results of patient.
Audiological and Electrophysiological Results of Present Case.
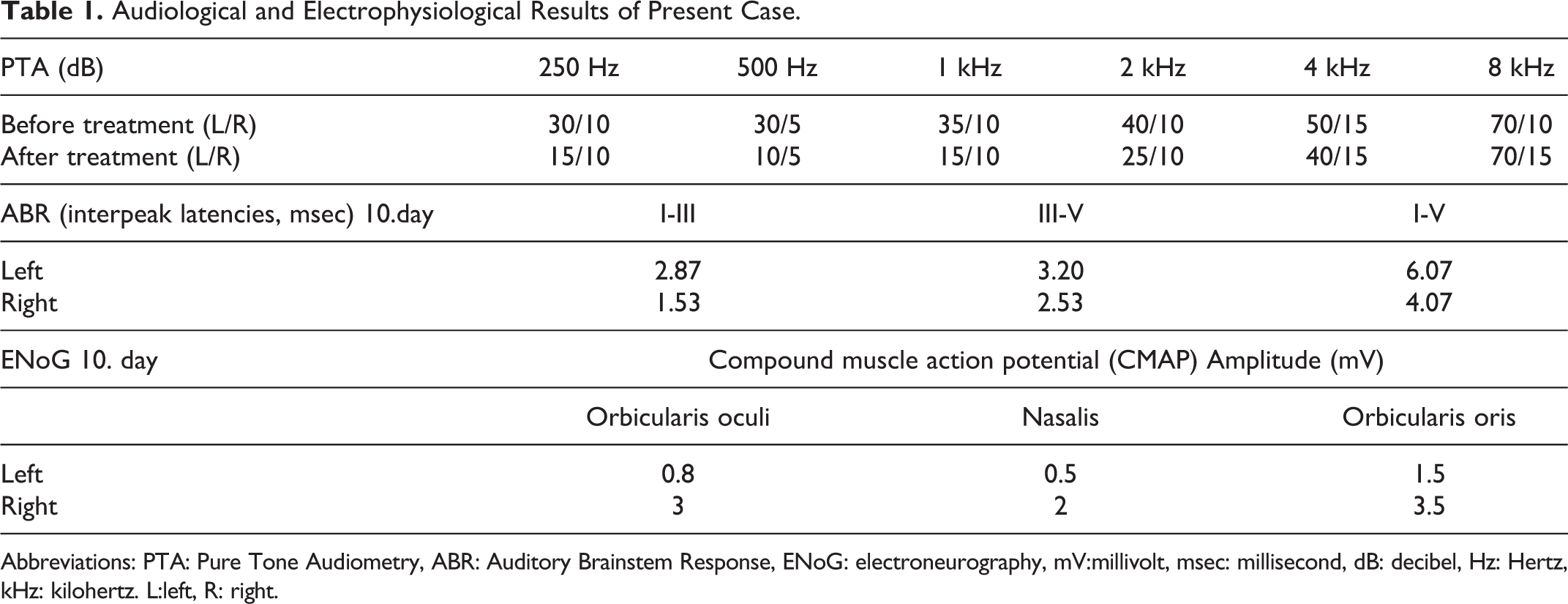
Abbreviations: PTA: Pure Tone Audiometry, ABR: Auditory Brainstem Response, ENoG: electroneurography, mV:millivolt, msec: millisecond, dB: decibel, Hz: Hertz, kHz: kilohertz. L:left, R: right.
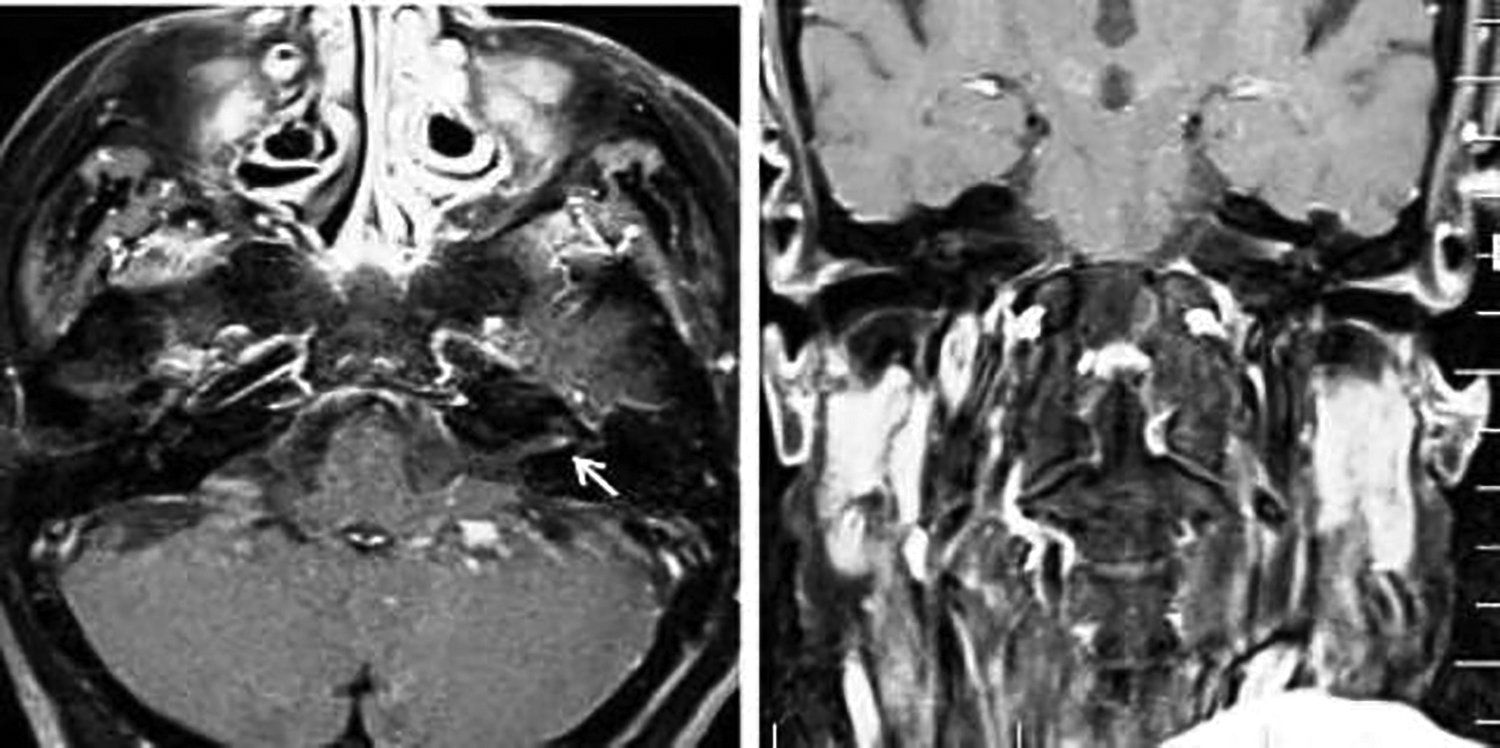
The internal acoustic canal 1.5 Tesla magnetic resonance imaging (MRI) images. Axial and coronal.
Discussion
Infections are common causes of facial paralysis and hearing loss (eg, the Herpes simplex viruses). 18 In experimental animal studies of other members of the coronavirus family, there is evidence showing that these coronaviruses can pass from the lungs to the circulatory system hematogenously or by axonal transport and transneuronal spread from the olfactory and trigeminal nerve endings in the nasal epithelium. These viruses can also access the nervous system from peripheral organs such as the dorsal root ganglia, which usually lack the blood–brain barrier. 19
Studies indicate that the CoV-2 virus uses the angiotensin-converting enzyme 2 (ACE-2) to enter the cell. 20 Angiotensin-converting enzyme 2 is abundant in the brain and the medulla oblongata; therefore, it is also present in the temporal lobe. The assumption is that the CoV-2 virus can easily affect the central auditory pathways in both the brainstem and auditory cortex. 20 A study of Mustafa 21 revealed that the damage caused by excessive cytokine increase and the transition of the cell by binding to the ACE-2 enzyme in the temporal lobe and brain stem are not the only factors affecting hearing in high viral load cases. The author of this study claims that the CoV-2 virus, like other neurotrophic viruses, caused viral damage to the Corti organ and hair cells through the effects of the otoacoustic emissions.
Worldwide, there have been 11 published patients with SSHL with positive COVID-19 serology tests so far (Table 2). Of these patients, 2 experienced bilateral hearing loss; one had bilateral intracochlear bleeding as a virus-related complication. 8 The other patient with meningitis may have had a virus-triggered inflammation of the meninges with subsequent spread to the cochlea, leading to acute hearing loss. The literature indicates this was the only patient—with profound bilateral SSHL—evaluated using the ABR and electrophysiological tests and urgently treated with cochlear implants. 6 The other patients have been tested subjectively with PTA or self-statement.
Cases of SSHL and Peripheral Facial Paralysis With Serologically Positive COVID 19 Published in the Literature.
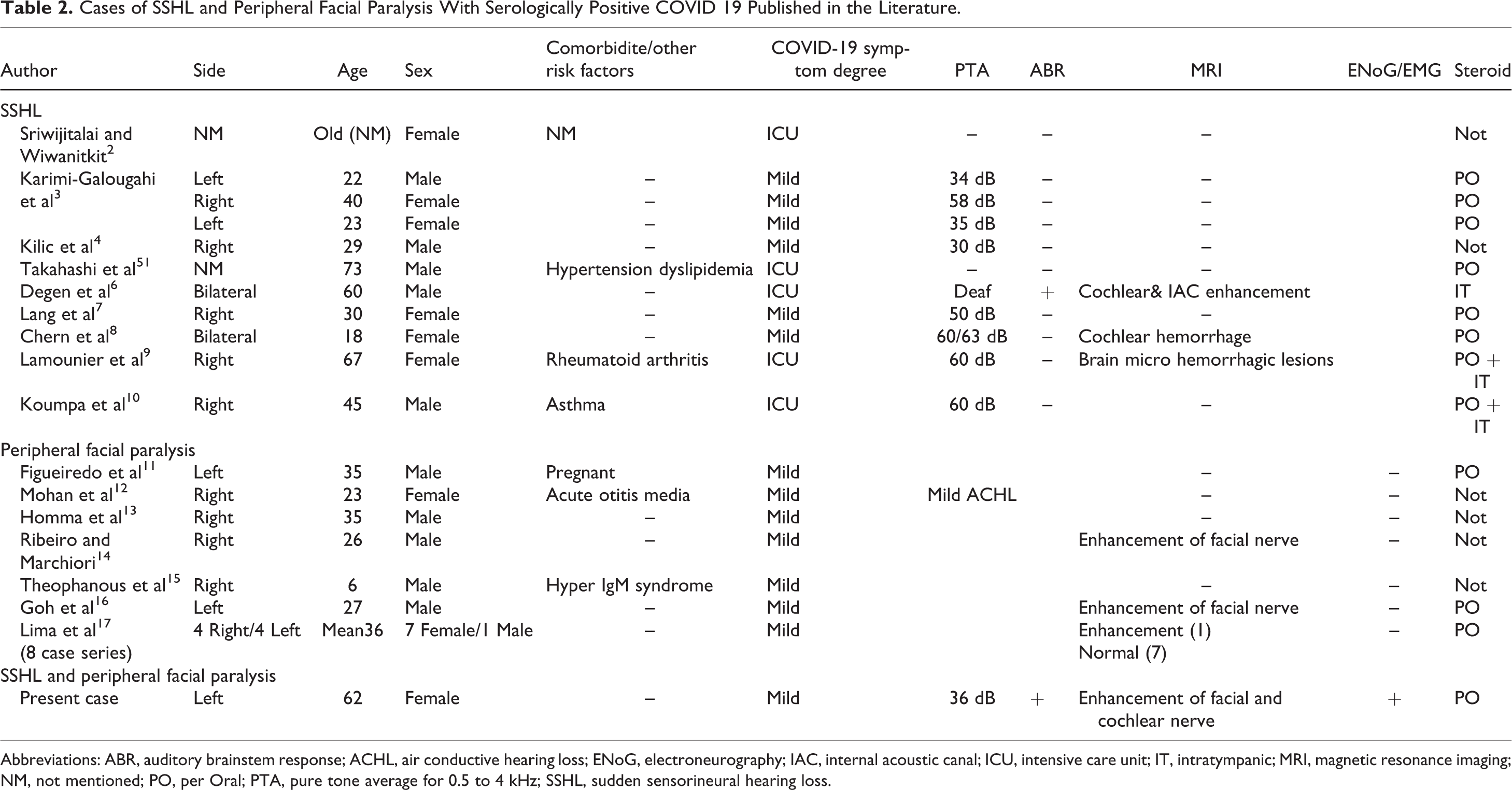
Abbreviations: ABR, auditory brainstem response; ACHL, air conductive hearing loss; ENoG, electroneurography; IAC, internal acoustic canal; ICU, intensive care unit; IT, intratympanic; MRI, magnetic resonance imaging; NM, not mentioned; PO, per Oral; PTA, pure tone average for 0.5 to 4 kHz; SSHL, sudden sensorineural hearing loss.
Reports detailing significant neurological diseases associated with COVID-19, including increased incidences of Guillain-Barre syndrome, encephalopathy, and strokes, were recently published. In an Italian cohort, Guillain-Barre syndrome was reported in approximately 0.5% of patients with COVID-19, with the first symptoms of flaccid paralysis occurring after the onset of acute respiratory symptoms. 22 However, isolated facial paralysis with positive COVID-19 serology tests is uncommon, with only 14 published cases so far (Table 2). Lima et al focused on the female dominance prevalent in the 8 cases reported—our patient is also female. However, when reviewing all publications in the literature, gender does not appear to be a significant factor. In consideration of the effects of age, only one child was present with the rest of the patients aged 30 and above. None of the patients were electrophysiologically evaluated to assess their prognosis.
The assessment of patient cases with the neurological involvement of COVID-19 indicated concerns about the use of corticosteroid treatment; it was only used in recently published cases, presumably due to medical professionals gaining more knowledge and experience about its use. Severe SSHL was observed in patients hospitalized in the intensive care unit with critical cases of COVID-19. However, it was noted that symptoms of hearing loss and facial paralysis were not predictable in patients with mild forms of the disease. For this reason, it may be beneficial to perform both radiological imaging and electrophysiological tests to make an accurate prognosis of COVID-19 patients, specifically when neurological findings occur.
The present case is unique due to the simultaneous involvement of the seventh and eighth nerve, as shown radiologically and electrophysiologically. Since we know that the interaural wave V latency should be no more than a 0.2 to 0.4 ms difference between ears, the elongation of I-V interpeak latency and wave V latency in this case indicates retrocochlear pathology. In addition, the MRI showing the enhancement complex of 7 to 8 nerves has taught us about the IAC and brainstem effect. This process may be initiated through the binding of CoV-2 virus to ACE-2 enzyme. Other possible complications of nerve damage include ischemia and demyelination induced by an inflammatory process. 18 This inflammatory process could be virus-triggered or immune-mediated, and this inflammation may affect nerves 7 and 8, as seen in other neurotropic viruses. 6,17,18
This single case report suggests a possible association between the SARS-CoV-2 infection with simultaneous SSHL and isolated facial paralysis. However, further studies are needed to determine whether this relationship is coincidental or occasional.
During this study, no financial or spiritual support was received neither from any pharmaceutical company that has a direct connection with the research subject nor from a company that provides or produces medical instruments and materials which may negatively affect the evaluation process of this study.
Footnotes
Acknowledgments
“Informed Consent Form for Scientific Research” was taken from the patient.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.