
Abstract
Petrified pinna is clinically characterized by an unbending rigid stone hard ear. Usually, the majority of the patients are asymptomatic but occasionally may experience pain from local pressure while sleeping. This uncommon condition is reported to be in association with local trauma, hypothermia, inflammation, and several life-threatening endocrine and systemic diseases. Awareness and knowledge to identify this entity is essential as it might be helpful in treating several systemic conditions and thus any untoward events.
Case Report
A 63-year-old male presented to our otolaryngology department with progressive stiffening of both the pinna since 2 years. He also gave a history of pain and discomfort over the pinna while sleeping in a lateral position. His family history was not contributory. There was no history of any physical trauma to the ear or exposure to cold weather. He denied any symptoms of hearing loss. Findings on physical examination of the head and neck were unremarkable. Examination of the ears revealed a normal appearance of both the pinna. The overlying skin and sensation over the pinna was also normal. On palpation, the pinna was unbending, rigid, and stony hard in consistency; however, the ear lobule was spared. Otoscopic examination revealed a normal external auditory canal and tympanic membrane. The patient denied any weakness of the facial nerve or any tenderness on palpation. An audiometric evaluation revealed symmetric mild high-frequency hearing loss in both ears probably age related. No other systemic findings were observed on general examination. Laboratory investigations that included complete blood count, blood glucose, serum electrolytes, serum calcium, serum phosphorous, parathyroid hormone, thyroid function tests, alkaline phosphatase, morning cortisol, uric acid, C-reactive protein, antinuclear antibodies, and liver and renal function tests were all within normal limits. Imaging of the temporal bone with high-resolution computed tomography (HRCT) revealed partial ossification (Figure 1) of the auricular cartilage in both ears. This presentation was consistent with petrified ear, most likely idiopathic. No surgical intervention was considered for this patient as he was relatively asymptomatic, and all the laboratory investigations were within normal limits.
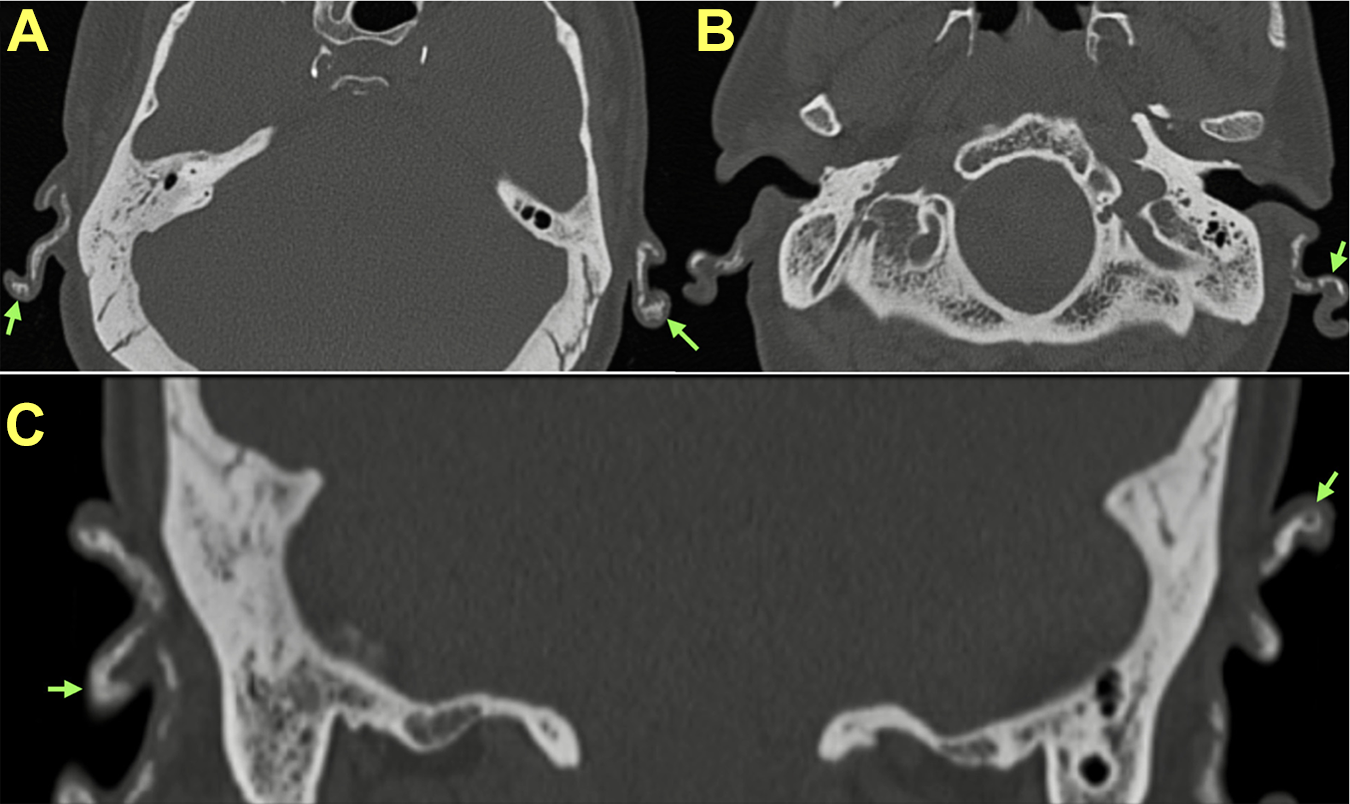
High-resolution computed tomography (HRCT) temporal bone (A, B) axial view and (C) coronal view showing partial ossification (green arrow) of the pinna bilaterally.
Discussion
Petrified ear is a rare clinical entity in which the entire pinna becomes stony hard due to calcification or ossification. It was first reported in 1866 by Vincent Bochdalek in Prague in a 65-year-old male cadaver. 1 The auricle is normally made up of elastic cartilage. Petrification of the auricular cartilage could be due to dystrophic calcification, metastatic calcification, or ectopic ossification. The petrification process can be initiated due to mechanical trauma, frostbite, or as a result of systemic or inflammatory conditions. The most common cause of petrified ear according to literature is frostbite. 2,3 Systemic conditions associated with petrified ear include hyperparathyroidism, diabetes mellitus, acromegaly, hypopituitarism, hyperthyroidism, Addison’s disease, sarcoidosis, ochronosis, systemic chondromalacia, Milk-alkali syndrome, familial cold hypersensitivity, and age related or following radiation therapy. Petrified ear appears to occur more commonly in men than in women. It is seen commonly in individuals older than the age of 60, and bilateral involvement is more frequent. Most of the patients are asymptomatic; however, some may complain of pain and discomfort when sleeping on the affected side. On physical examination, the pinna is rigid and immobile, and the ear lobule is usually spared. Rarely, patients complain of subjective hearing loss which can be assessed by audiogram. As the petrified ear is associated with the various endocrine disorder and systemic conditions, laboratory evaluation is fundamental to detect any underlying condition. Imaging with plain radiography and HRCT temporal bone is diagnostic. On an X-ray, skull hyperdense areas of calcification or new bone formation may be seen. High-resolution computed tomography temporal bone shows uniform hyperdense areas indicating calcification and radiolucent spaces within hyperdense areas representing the trabecular bone formation seen in ossification. 3,4 Histopathological examination is not mandatory in all cases but can confirm the diagnosis as it distinguishes between calcification and ossification. Histopathological examination will show fibrocartilaginous tissue being replaced by lamellar bone and osteocytes in cases of ossification of the pinna. Identifying and treating the underlying metabolic or endocrine disease may help in preventing further progress of calcification and hardening. As most of the patients are asymptomatic, no specific treatment may be necessary and most patients choose to forgo surgery, as in our case. According to literature, patients who are symptomatic have shown improvement with wedge resection of the affected cartilage or conchal reduction surgery.
Conclusion
It is important to have adequate knowledge to diagnose petrified ear as it would be useful for all clinicians, particularly considering its association with potentially serious and life-threatening metabolic, and endocrine or systemic conditions. There is no known treatment to reverse the calcification or ossification process. As the majority of the patients with auricular ossification are asymptomatic and no treatment is required. Supportive therapy may be adequate in treating symptomatic patients for alleviation of pain and insomnia associated with the petrified ear.
Footnotes
Acknowledgments
The authors would like to gratefully acknowledge and thank the faculty, patient, and attendants for accepting for publication. Informed consent was obtained from the patient.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.