
Abstract
Metastatic disease from primary colon cancer in the thyroid is rare. The authors have submitted such a case. What makes this case particularly unusual is that it was in a man. 80% of such cases are in women. It has been speculated that there may be a humoral component. What is even more unique in this case is that it was found during the workup of a symptomatic parathyroid adenoma. The diagnosis was confirmed with immunochemistry using markers Cytokeratin 20 (CK20), Cytokeratin 7 (CK7), and Thyroid Transcription Factor 1 (TTF-1) .
Introduction
Tumor metastasis to the thyroid is well-documented in primary breast, lung, or renal cancer. There have been rare case reports of colon cancer with thyroid metastasis. The numbers are too small to draw any conclusions, but more than 75% of cases involved female patients. This is a case of a male who underwent colon resection, partial hepatectomy, and postoperative chemotherapy 2 years ago. He appeared to be in complete remission. During his workup for a parathyroid adenoma, a thyroid mass was noted. Pathology revealed a parathyroid adenoma and a metastatic thyroid lesion from a primary colon lesion.
Case Report
The case is a 78-year-old male, who underwent right colon resection, right liver resection, and Foxfal chemotherapy for stage IV colon cancer 2 years ago. He appeared to be in complete remission. The routine lab work revealed hypercalcemia. Additional testing revealed elevated parathyroid hormone levels. The preoperative ultrasound imaging demonstrated a mass in the left lobe of the liver and small lesions in the right lobe of the liver. In the operating room, a left parathyroid adenoma was identified and removed. A near-total thyroidectomy was also performed. Pathology revealed a multifocal Hurthle cell adenomatous nodule with partial replacement by metastatic colon cancer in the thyroid’s left lobe (see Figure 1). The immunohistochemical stains tested positive for CK20, and negative for CK7 and TTF-1. This confirmed the diagnosis of metastatic colon adenocarcinoma in the thyroid tissue. Although this immunophenotype is not pathognomonic, it is typical of colorectal cancer. He did not wish to receive additional chemotherapy. He expired within one year.
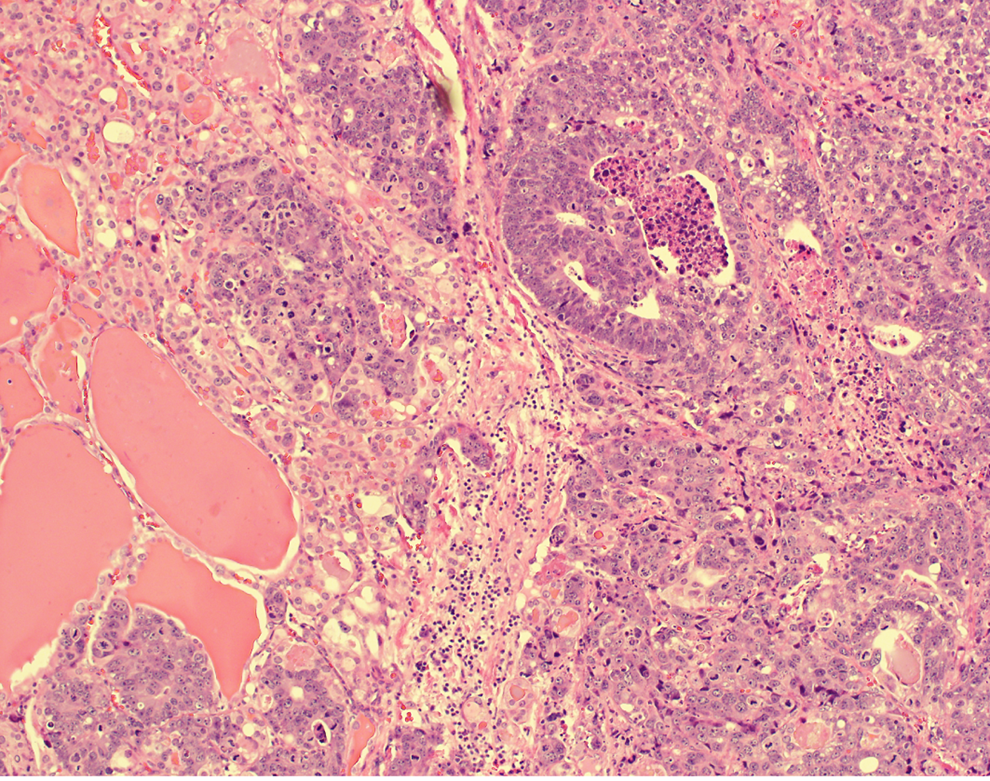
Metastatic adenocarcinoma in the thyroid gland.
Discussion
Metastatic involvement of the thyroid is rare. It has been reported to be as low as 0.05%. The Mayo Clinic has reported only 43 cases in the past 10 years. 1 The most frequent primary tumors were located in the kidney, breast, and lungs. Two possible mechanisms were suggested to contribute to the low incidence of metastatic thyroid involvement. Its rich and fast blood flow makes tumor implantation and adhesion difficult. Alternatively, high iodine concentration and high oxygen saturation contribute to a less optimal tumor cell growth environment. 2 When an organic disorder, such as adenomatous goiter, is present in the thyroid tissue, there is a decrease in blood flow, oxygen, and iodine, making the thyroid tissue more susceptible to metastatic implantation. 3 In this particular case, the metastatic lesion was found in a Hurthle cell adenomatous nodule. This was consistent with Smith’s postulate.
Asymptomatic thyroid metastases, such as the present case, account for 31% to 50% of cases. 4 There is a high index of suspicion for a patient with a thyroid mass and a prior malignancy history. Based on the previous autopsy series, the most common primary site was the lungs. Based on previous clinical series, the most common primary malignancy was renal cell carcinoma. Immunochemistry is required to confirm colon cancer metastases.
This case was unique since the patient presented with a parathyroid adenoma. He was diagnosed with hyperparathyroidism based on standard preoperative laboratory testing. In the OR, the left lower parathyroid was removed. The diagnosis of a parathyroid adenoma was confirmed histologically. The patient underwent palliative treatment. Local resection avoided future problems, particularly swallowing difficulty, and airway compression. His hypercalcemia resolved. Treatment strategies are made on a case-by-case basis depending on the tumor burden in the other sites and the patient’s overall medical condition. In this particular case, the patient previously completed a chemotherapy course, and he decided that he did not want additional therapy.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.