
Abstract
We report a rare case of isolated malleus dislocation into the external auditory canal with lateralized intact tympanic membrane following a head trauma. The patient was a 63-year-old woman who presented at the outpatient department of our institute with hearing loss of 10 years’ duration after a bicycle accident. During physical examination of the patient, total dislocation of the malleus-like bony structure into the external auditory canal on the right side was observed. In the computed tomography scan, an isolated malleus dislocation with intact incus-stapes articulation was identified. The patient was successfully treated with endoscopic exploratory tympanotomy and partial ossicular replacement prosthesis. The isolated malleus dislocation can rarely occur after trauma. A careful diagnostic step through history, physical examination, and temporal bone computed tomography scan are needed to confirm this rare condition.
Introduction
Temporal bone trauma is usually associated with hearing loss and can manifest as sensorineural hearing loss, conductive hearing loss, or mixed type of hearing loss, depending on the cause of the injury such as ossicular disruption or damage to the oval and round window. 1,2 Conductive hearing loss after trauma can occur by hemotympanum, tympanic membrane perforation, and ossicular dislocation or fracture. Hemotympanum resolves spontaneously, usually within a few weeks without intervention, and traumatic perforation of the tympanic membrane at either the anteroinferior quadrant or anteroposterior quadrant may heal spontaneously without causing any hearing problem. 3 However, if conductive hearing loss persists for >2 months after the tympanic perforation and middle ear lesions are resolved, clinicians should consider the possibility of ossicular disruption. 4 Ossicular disruption includes various types, of which incus-stapes (IS) dislocation is the most common type, followed by incus dislocation and fracture of the suprastructure of the stapes, and occurrence of multiple ossicular injuries is more common than that of isolated injury. 5 -7 In particular, since the malleus is stabilized by the tensor tympani muscle and tympanic membrane, isolated dislocation malleus is extremely rare. 8
Herein, we present a rare case of isolated malleus dislocation into the external auditory canal (EAC) without other ossicular injuries following head trauma.
Case Report
A 63-year-old woman visited the ENT Department of our institute with complaints of progressive right-sided hearing loss. She had experienced hearing loss for 10 years due to traumatic head injury following a bicycle accident. At the time of accident, no evaluation and management of her hearing loss was performed. During initial physical examination, dislocated malleus into the posterosuperior portion of the EAC with an intact tympanic membrane was observed (Figure 1). Pure tone audiometry was conducted, and in the results, conductive hearing loss was detected with accompanied 30 to 40 dB air–bone gap in the right ear (Figure 2A). On the temporal bone computed tomography (CT) scan, a disrupted ossicular chain with a malleus-like bony structure in the EAC of the right ear was observed, but IS articulation was intact without fracture (Figure 3). Decision of surgical management was made after obtaining sufficient information from the patient. Endoscopic exploratory tympanotomy was performed, and during the procedure, elevation of the tympanomeatal flap revealed dislocated malleus at the posterosuperior wall of the EAC with bony integration (Figure 4A). The malleus was carefully removed, while maintaining mobility of the incus and stapes (Figure 4B). Partial ossicular replacement prosthesis (PORP, 2.5 mm, titanium) was placed after removal of the incus between the stapes head and tympanic membrane (Figure 4C). Finally, the tympanic membrane was restored using tragal cartilage. Postoperatively, the patient reported improvement of hearing, and pure tone audiometry performed at postoperative 2 months showed complete closure of the air–bone gap (Figure 2B).
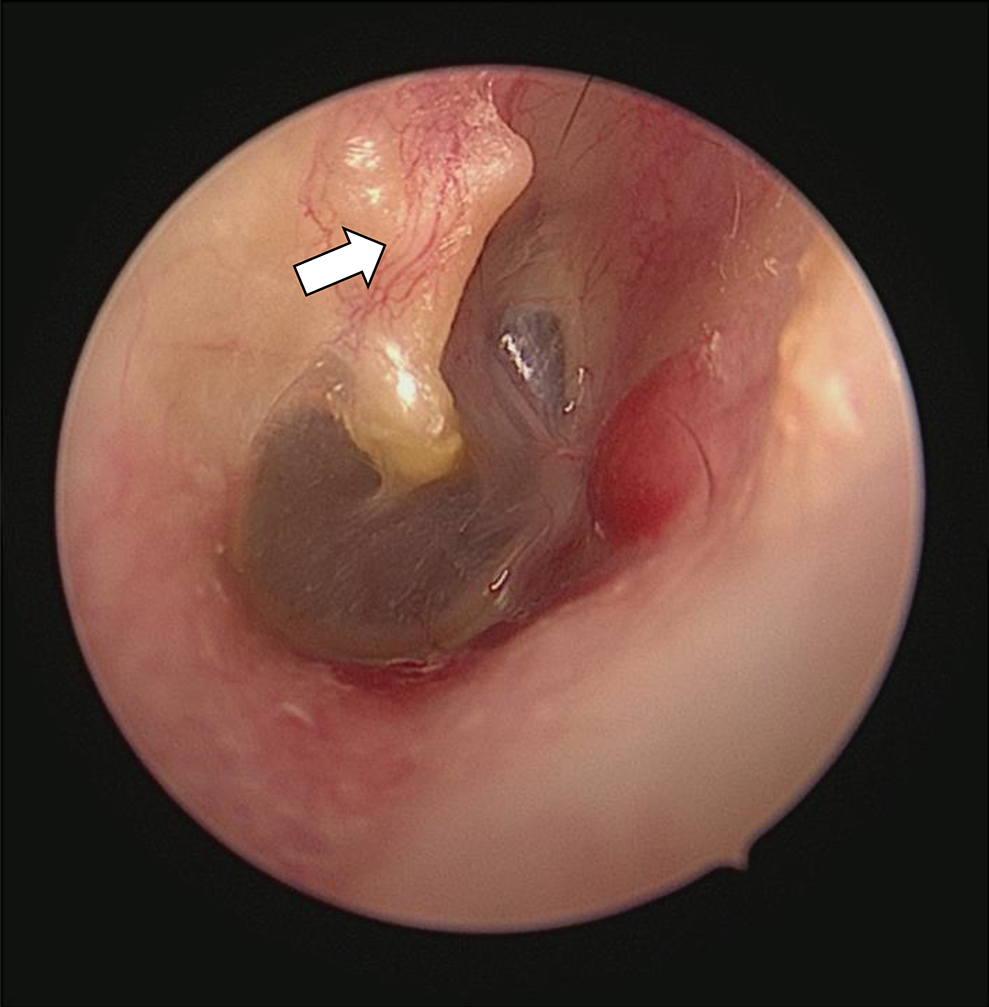
Otoscopic examination shows dislocated malleus with intact tympanic membrane (malleus, white arrow) abutting to the superior–posterior wall of the external auditory canal in the right ear.
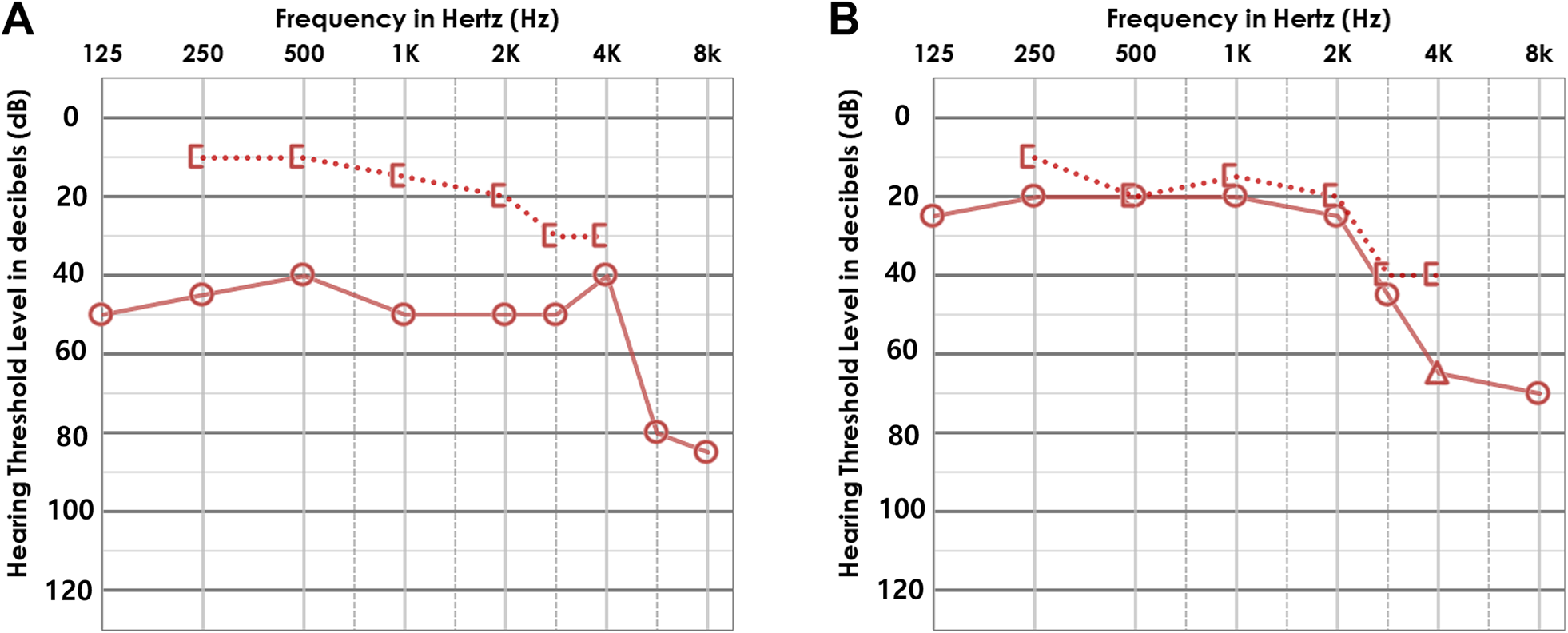
(A) Preoperative audiometry with moderate conductive hearing loss. (B) Postoperative audiogram at 2 months after endoscopic ossiculoplasty demonstrating complete closure of air–bone gap.
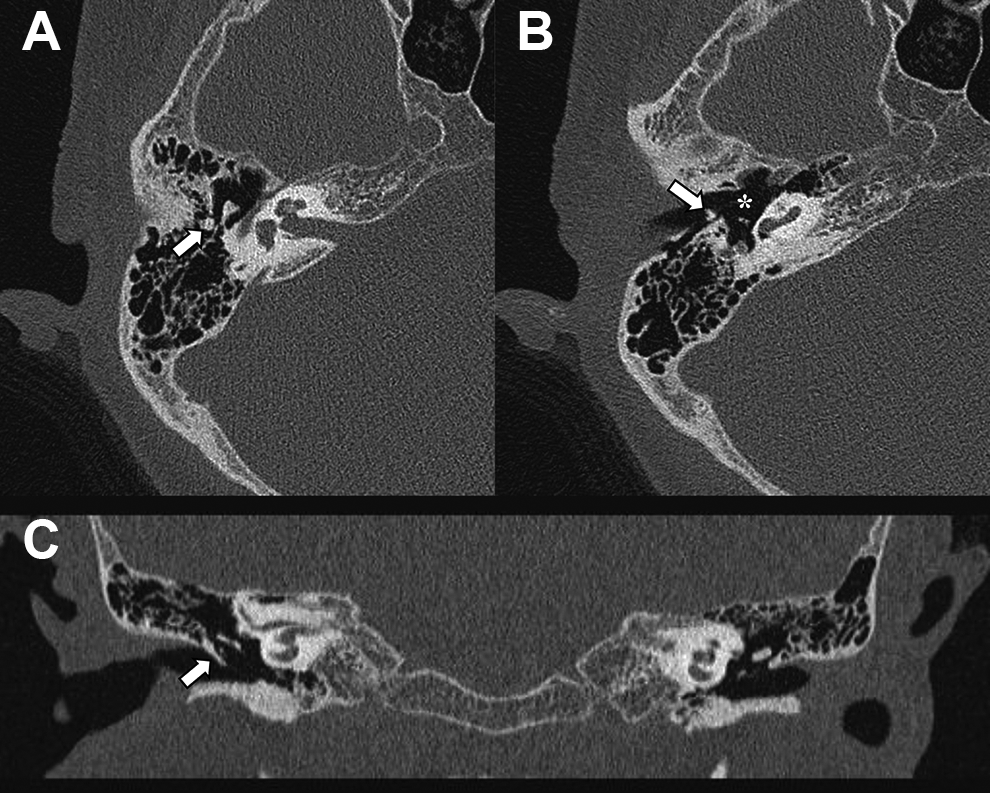
(A and B) Axial temporal bone computed tomography (CT) clearly showed isolated malleus dislocation to the external auditory canal (white arrow) and intact incus-stapes articulation (asterisk). (C) Coronal CT also showed malleus dislocation to the superior wall of external auditory canal (white arrow).
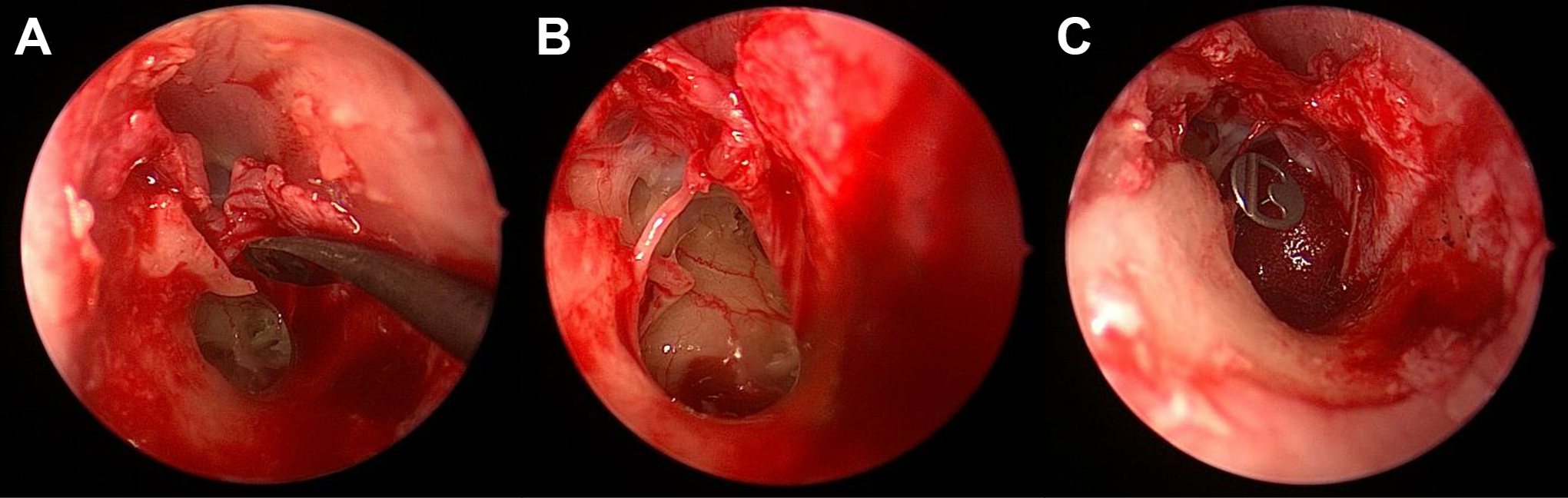
Operating finding. (A) Totally dislocated malleus was noted at the posterosuperior wall of external auditory canal (EAC) with bony integration. (B) After removal of dislocated malleus intact incus-stapes articulation was noted. (C) Partial ossicular replacement prosthesis (PORP, 2.5 mm, titanium) was placed at the stapes head.
Discussion
We experienced a rare case of a patient with total dislocation of the malleus into the EAC without other ossicular injuries following an event of head trauma. Among various type of ossicular injury, IS dislocation is the most common ossicular chain disruption after trauma. 7,9 Compared with the incus, the malleus and stapes are relatively stable against disarticulation or traumatic injury, and among the ossicles, the malleus is more firmly attached and stabilized by the tympanic membrane, tensor tympani tendon, and anterior and lateral mallear ligaments. 9 In addition, the incudomalleolar joint is protected within the epitympanic recess. Due to these anatomic characteristics, in cases of trauma, the malleus maintains its position or moves only slightly. The stapes is also protected by the annular ligament and stapedial tendon, whereas the incus is suspended only by the ligamental structure. Strohm reported that IS articulation was the weakest joint that tolerated 52 g of external force, followed by the incudomalleolar joint (67 g), stapes (166 g), and long process of the incus (674 g). 10
Based on the anatomical positions and physical properties of the ossicular chain, the incus is most vulnerable to trauma and susceptible to dislocation due to tenuous suspension between the malleus and stapes 8 ; therefore, kinematically, malleus dislocation usually occurs with that of the incus, which is referred to as incudomalleolar dislocation, and isolated malleus dislocation is unlikely to occur as compared to other types of injury. To the best of our knowledge, no reports on isolated malleus dislocation at the EAC are available in the literature. The exact mechanism of isolated malleus dislocation is very complex and depends on the direction of vector and fracture line, flexibility of the skull, and amount of energy transmitted to the ossicular chain during injury. 9,11 Harris and Butler reported that implosive force may produce fracture or dislocation of the malleus, which is rare and usually accompanies other ossicular injuries. 12 In our case, fracture of the posterosuperior wall of the EAC occurred during the traumatic event, and the dislocated malleus was trapped by the implosive force generated.
High-resolution temporal bone CT finding of loss of normal articulation of the ossicles contributes to the diagnosis of traumatic ossicular disruption. 13 In our patient, we made a diagnosis of dislocated malleus with intact IS joint by CT; moreover, we confirmed that the malleus was dislocated and trapped in the posterosuperior wall of the EAC during surgery. Ossicular reconstruction of conductive hearing is achieved through an autologous incus graft, PORP, or a total ossicular replacement prosthesis, depends on the type and location of injury to the ossicular chain. 7,14
Supplemental Material
Supplemental Material, sj-pdf-1-ear-10.1177_01455613211026529 - Isolated Traumatic Dislocation of the Malleus into the External Auditory Canal
Supplemental Material, sj-pdf-1-ear-10.1177_01455613211026529 for Isolated Traumatic Dislocation of the Malleus into the External Auditory Canal by Jong Hwan Lee, Ji Woong Choi, Do Yoon Jeong, Sultan Mohammed Alanazy and Gi-Sung Nam in Ear, Nose & Throat Journal
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by research fund from Chosun University, 2021.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.