
Abstract
Perforations of the nasal septum have many etiologies and occasionally result from intranasal medicated spray use. This case report describes a perforation related to the use of desmopressin nasal spray, which has not been previously reported in the literature. Clinical considerations presented in this article include appropriate technique of nasal spray application, appropriate monitoring of patients on intranasal sprays, and indications for evaluation by an otolaryngologist. Septal perforation treatment success is improved with an early diagnosis.
Introduction
Perforations of the nasal septum are not uncommon. A Swedish population study found a 0.9% incidence of septal perforation. 1 A 2.05% perforation prevalence was noted reviewing facial bone computed tomography (CT) scans taken in a New York City trauma hospital. 2 Perforations are usually diagnosed on physical examination following the documentation of varied rhinologic symptoms. Perforations positioned anteriorly are more likely to be symptomatic, in part due to the desiccating effect of inspired air. The most common presenting symptoms are crusting, obstruction, epistaxis, and a whistling sound on inspiration. Congestion, rhinorrhea, dysosmia, and facial pain symptoms may be indistinguishable from those experienced with chronic rhinosinusitis. An aesthetic nasal saddle and/or columellar retraction deformity may occur if septal support is compromised.
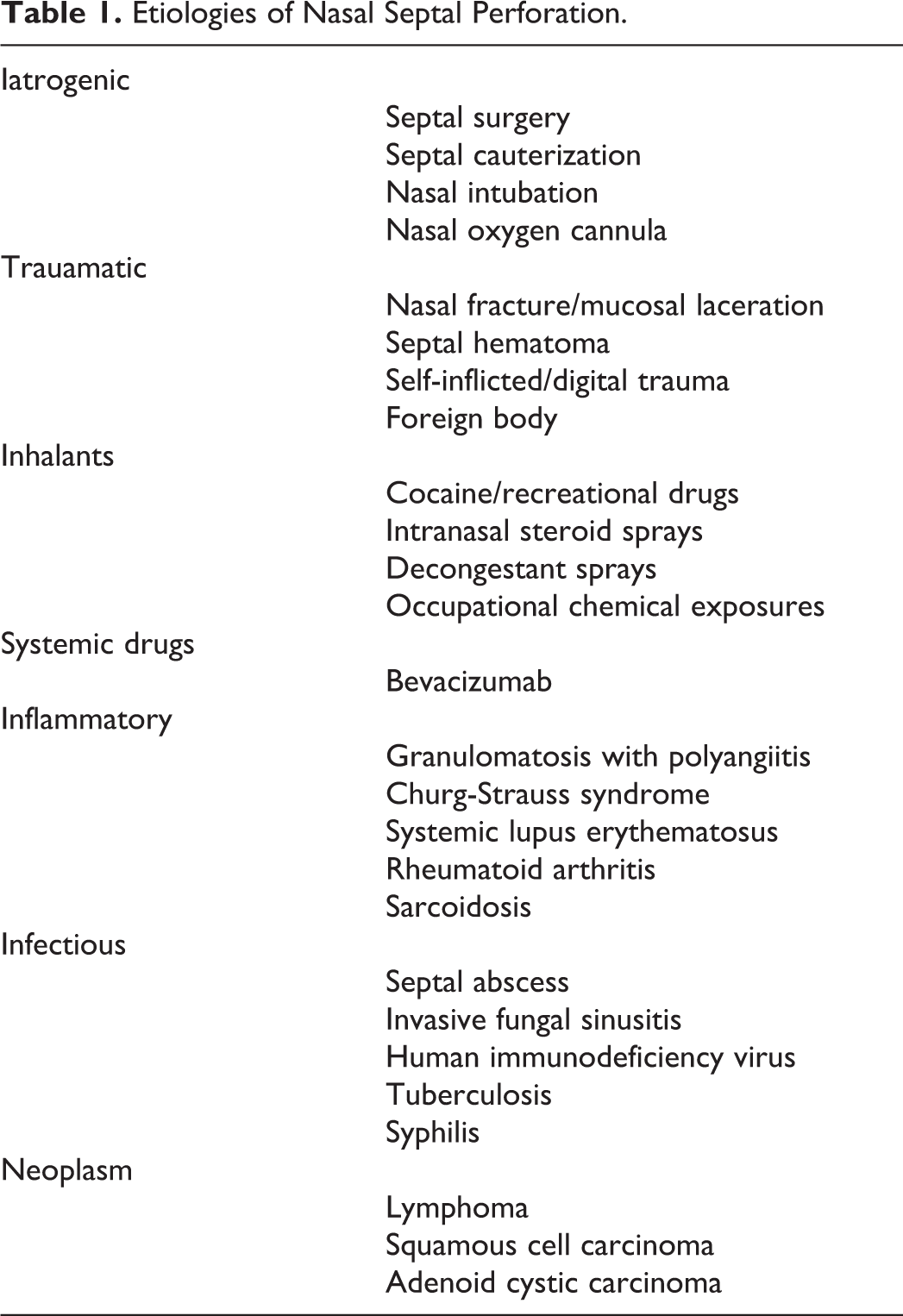
The anterior nasal septum is comprised of the relatively avascular quadrangular cartilage nourished by the overlying and highly vascular mucoperichondrium. Any chemical, physical, or inflammatory septal injury can result in ischemic necrosis of the septal cartilage with progression to perforation. There are numerous and varied etiologies for perforations of septum (Table 1). Presumably, topical septal exposures injure and ulcerate the mucoperichondrium bilaterally resulting in cartilage exposure, devascularization, and necrosis. Inhaled cocaine and decongestant sprays may cause necrosis through mucosal vasoconstriction.
Etiologies of Nasal Septal Perforation.
Desamino-
Case Presentation
A 39-year-old female with a known septal perforation presented with symptoms of nasal crusting, epistaxis, and nasal pain. The patient had undergone a transnasal pituitary adenoma resection 9 years prior to presentation. Review of the operative note confirmed preservation of the septal cartilage and anterior bony septum. There was no evidence of septal perforation on serial postoperative nasal examinations. A head CT scan performed 7 months postoperatively demonstrated an intact, deviated septum.
The patient developed diabetes insipidus which was treated with desmopressin nasal spray. Nasal crusting and bleeding developed after 5 years of spray use, and spray application crossing over to the contralateral nasal cavity was eventually noted by the patient. A perforation was diagnosed, and desmopressin spray use was discontinued. Thirst and polyuria persisted despite the use of oral desmopressin, resulting in reinstitution of the spray application. A CT scan obtained at the time of diagnosis demonstrated an anterior septal perforation which measured 15 mm in length by 11 mm in height (Figure 1, coronal view A, sagittal view B). Nasal symptoms did not improve with moisturizing treatments. Perforation obturation with a customized silastic septal prosthesis was attempted but was not tolerated. At presentation to our practice, anterior rhinoscopy revealed progression of the septal perforation since the time of the CT scan one year prior. The posterior margin of the perforation was ulcerated and crusted with dried blood. Surgical closure was recommended for symptom treatment and to stop perforation progression. The perforation measured 19 by 15 mm at surgery (Figure 1C, intraoperative photo). An obstructing left-sided septal deformity was noted and corrected posterior to the perforation. There was no evidence of prior quadrangular cartilage resection. Perforation closure was performed endonasally utilizing bilateral mucosal flaps supported with a temporalis fascia interposition graft. 4 Mucosa from the undersurface of the left upper lateral cartilage was incorporated into the repair to ensure a complete, tension-free closure following flap advancement and suturing. The intraoperative and postoperative courses were uneventful. Mild septal crusting persisted. Intranasal desmopressin use was resumed 7 months postoperatively after instruction on proper usage. There was no evidence of reperforation one month later.
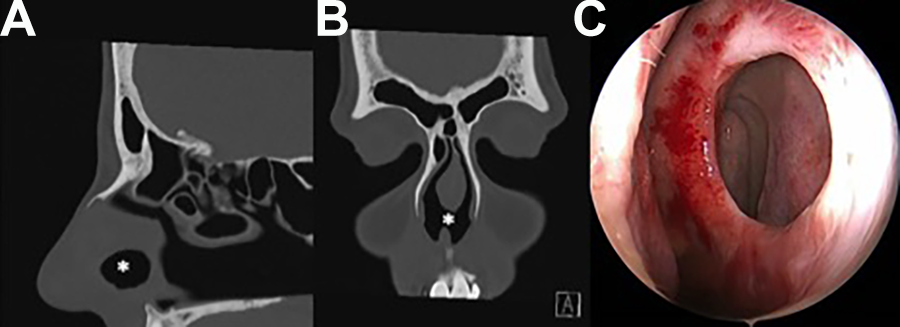
Septal perforation (asterisk). (A) Computed tomography scan at time of diagnosis, sagittal view. (B) Coronal view. (C) Intraoperative endoscopic photo demonstrates progression of perforation size. Asterisk (*) indicates septal perforation.
Discussion
Desmopressin is a synthetic analog of vasopressin, an antidiuretic peptide hormone that increases plasma von Willebrand factor, factor VIII, and tissue plasminogen activator. 3 Water permeability in renal tubular cells is increased by desmopressin, leading to water absorption and increased urine osmolality. 3 Peptide hormone drugs are available as nasal sprays to minimize the degradation noted following oral administration. The bioavailability of the commercial desmopressin tablet is 0.1% while that of the nasal spray is 3% to 5%. 5 Our study patient did not benefit from oral desmopressin.
The effect of intranasal desmopressin on pediatric nasal mucosa following its administration for nocturnal enuresis has been investigated. 6,7 These studies demonstrated no qualitative cytologic changes on mucosal samples collected after 6 months of therapy. In addition, Akoglu et al 6 demonstrated mucociliary clearance time did not change after 6 months of treatment, suggesting the spray did not damage nasal mucosa. Desmopressin treatment is often required beyond 6 months. Lack of prior reports associating perforations with prolonged therapy provides indirect evidence against desmopressin interacting adversely against septal mucosa or cartilage. Desmopressin does not have a mucosal vasoconstrictive effect.
Recognition of the association between intranasal corticosteroid spray use and septal perforation may provide context for our study patient. Regarded as an anecdotal observation in the 1980s, intranasal corticosteroid spray use is now considered to be a risk factor for septal perforation. 8 -10 We have attempted surgical closure of over 400 perforations and have noted a 35% incidence of steroid spray use when no other etiology could be determined. The temporal association between the commencement of spray use and onset of nasal symptoms with subsequent perforation diagnosis was strong for many of these patients. Pharmacological effects on the septal mucosa such as vasoconstriction or delayed hypersensitivity, due to the steroid or preservative, have been advanced to explain the association of steroid sprays with perforation. 11 It has been suggested that prolonged use of nasal steroid sprays can cause mucosal atrophy, drying, and crusting, leading to ulceration and exposed cartilage. However, long-term follow-up studies of patients using nasal steroid sprays have not demonstrated mucosal atrophy. 9
Steroid spray–related perforations may be due to application method rather than a medication side effect. 11 -13 One possible mechanism of injury is trauma from direct contact of the hard plastic tip applicator against the delicate septal mucosa. 12 Alternatively, the repeated force of a spray pointed directly onto the septum could cause recurrent mucosal microtrauma leading to ulceration. We have noted a perforation following 3 months of nasal oxygen cannula use. Patients with a history of conditions potentially affecting septal vascularity (prior septal surgery, nasal trauma, decongestant spray abuse, history of cocaine use) may be at risk for perforation with steroid spray use. Our study patient had undergone prior transseptal pituitary surgery in which neither septal cartilage nor anterior septal bone were removed. Postoperative examinations and CT scan did not reveal a perforation. The patient developed the perforation years after surgery, indicating a lack of correlation between her pituitary surgery and emergence of the perforation. There were no other nasal treatments or manipulations identified which could lead to a perforation. We have linked the use of desmopressin spray to this perforation, likely due to mucosal microtrauma from spray application and not a medication side effect. Reinstitution of spray use following temporary cessation appeared to result in perforation progression.
Clinicians prescribing medicated nasal sprays should educate patients on proper spray technique, including neutral head position, upright posture, and positioning the tip of the applicator to direct the spray away from the septum and in the direction of the ipsilateral medial canthus. 12 Patients should be instructed to discontinue the use of a medicated spray causing prolonged nasal irritation or bleeding and present for nasal reexamination.
Perforations of the nasal septum present under varied clinical circumstances which can pose distinct management challenges for the otolaryngologist. Conservative moisturizing treatments are instituted at diagnosis and serological studies, CT scanning, cultures, and/or biopsy are performed as indicated to determine perforation etiology. Silastic septal prostheses (buttons) may successfully obturate the defect to ameliorate perforation symptoms, which are often substantial. Computed tomography imaging has been utilized to model the perforated septum for the fabrication of custom perforation prostheses. 14 Our study patient did not tolerate this treatment. We have noted that, given the opportunity, most patients would like to be cured of their symptomatic perforation. Numerous closure techniques have been described with most publications reporting on procedures utilizing physiologic nasal mucosal flaps. 15 Closure success rates exceeding 90% have been reported. 5 Septal perforation surgery can be challenging, and closure rates diminish as perforation size increases. Early diagnosis facilitates the successful surgical management of problematic perforations.
Intranasal medicated spray applications may cause a septal perforation. This case report describes a perforation related to desmopressin nasal spray. Patients utilizing a medicated spray should be instructed on proper spray application. Rhinologic evaluation is indicated when nasal symptoms following onset of spray use persist after the spray is discontinued. Septal perforation treatment success is improved with an early diagnosis.
Footnotes
Acknowledgments
The corresponding author certifies that permission has been obtained for the publication of this case report from those acknowledged.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.