
Abstract
Olfactory neuroblastoma (ONB) is a rare malignancy of the sinonasal cavity, originating from neuroepithelial olfactory cells. Olfactory neuroblastoma can be difficult to diagnose due to its anatomic position and variable symptomatic presentation, leading to diagnosis at a more advanced stage. Here, we present the case of a 35-year-old man with no previous medical history who had a bicycle accident secondary to syncope. He was found to be hyponatremic and suspected to have syndrome of inappropriate antidiuretic hormone secretion (SIADH). In the workup of SIADH, a brain magnetic resonance imaging revealed a mass in the left middle meatus. The lesion secreted inappropriate amounts of ADH, resulting in symptomatic paraneoplastic SIADH. This ultimately led to the early recognition and successful resection of this rare ONB. The patient has remained disease-free for over 5 years. This case is a fortunate example of a functional malignancy of the sinonasal tract that was discovered early and successfully treated as a result of symptomatic SIADH.
Keywords
Introduction
Olfactory neuroblastoma (ONB) is a rare malignancy of the nasal cavity, which was first described in 1924 by Berger. Olfactory neuroblastoma originates from the neuroepithelial cells of the sinonasal tract. This malignant neoplasm represents 3% of all nasal and sinus neoplasms, 1 and most frequently appears in the second and sixth decades of life. 2 Olfactory neuroblastoma is treated with surgical resection in conjunction with radiation therapy. Chemotherapy may be used if the lesion has metastasized or if the lesion is unresectable. Olfactory neuroblastoma can be asymptomatic in the early stages, contributing to a more advanced stage at diagnosis. Moreover, the nonspecific and seemingly benign symptoms 3 combined with the rarity of ONB make diagnosis difficult.
Here, we present a case of ONB diagnosed and resected early, secondary to symptomatic paraneoplastic syndrome of inappropriate antidiuretic hormone secretion (SIADH). To our knowledge, there are 41 cases in the literature of functional ONB inducing SIADH. 4 -10
Case Report
A 35-year-old man with no previous medical history experienced a bicycle accident secondary to syncope. He was seen at urgent care, where he was found to have hyponatremia (Na, 119 mEq/L). His sodium level improved to 131 mEq/L following treatment with salt tablets and Lasix. The hyponatremia was believed to be secondary to SIADH, due to his response to treatment and the overall clinical picture. Subsequent brain magnetic resonance imaging (MRI) revealed a sinonasal mass, 2.6 cm in maximum diameter, at the left middle meatus (Figure 1).
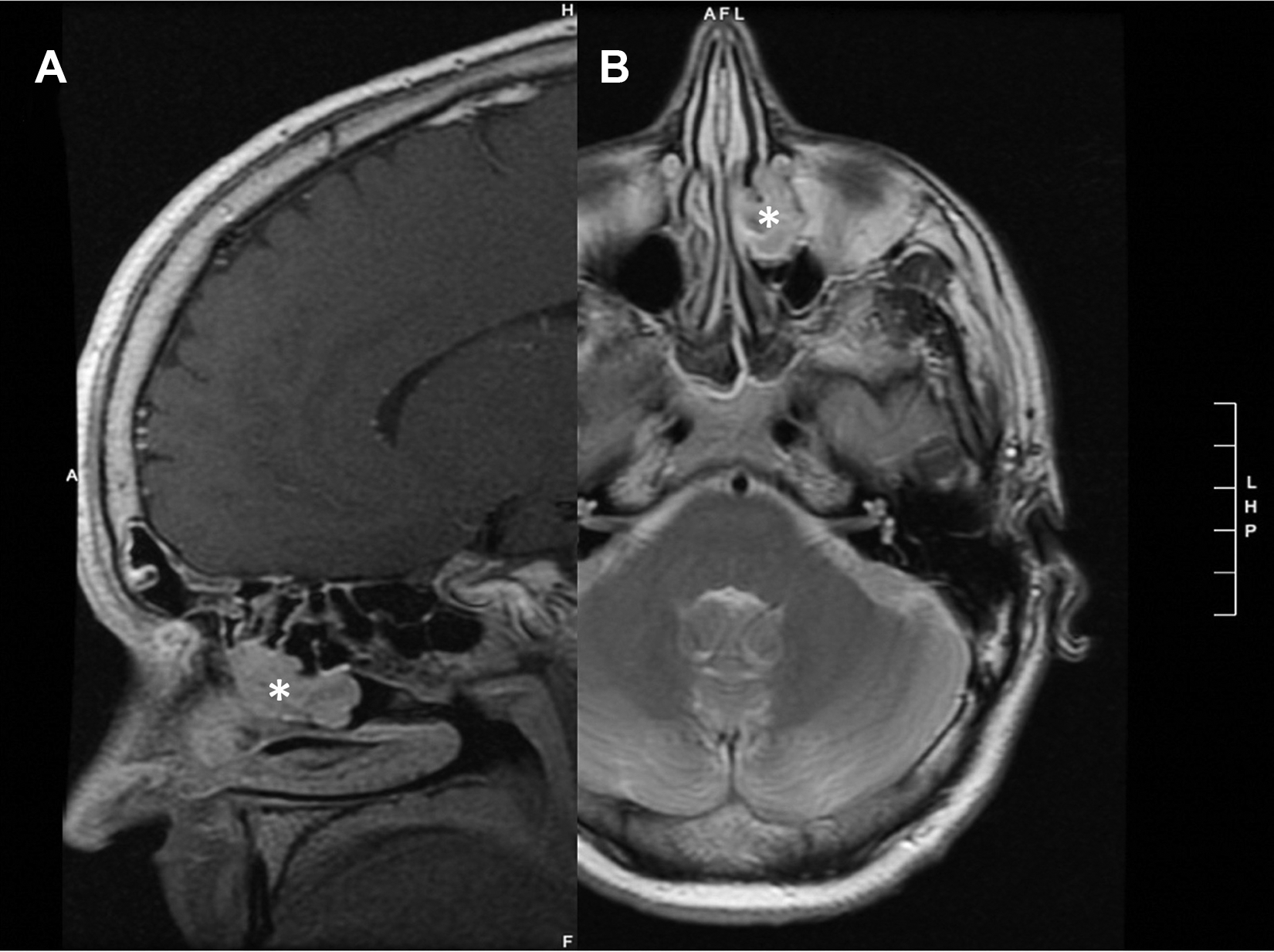
Sagittal (A) and axial (B) MRI of the head confirming that the mass (*) is limited to the left nasal cavity, left maxillary, and anterior ethmoid sinuses. MRI indicates magnetic resonance imaging.
Computed tomography (CT) of the sinus showed that the mass was limited to the left nasal cavity, left maxillary, and anterior ethmoid sinuses. Left-sided endoscopic resection was performed 5 months later. The tumor measured 3.0 × 2.5 × 1.5 cm and was removed en bloc. The final diagnosis was an ONB, Kadish B (Figure 2).
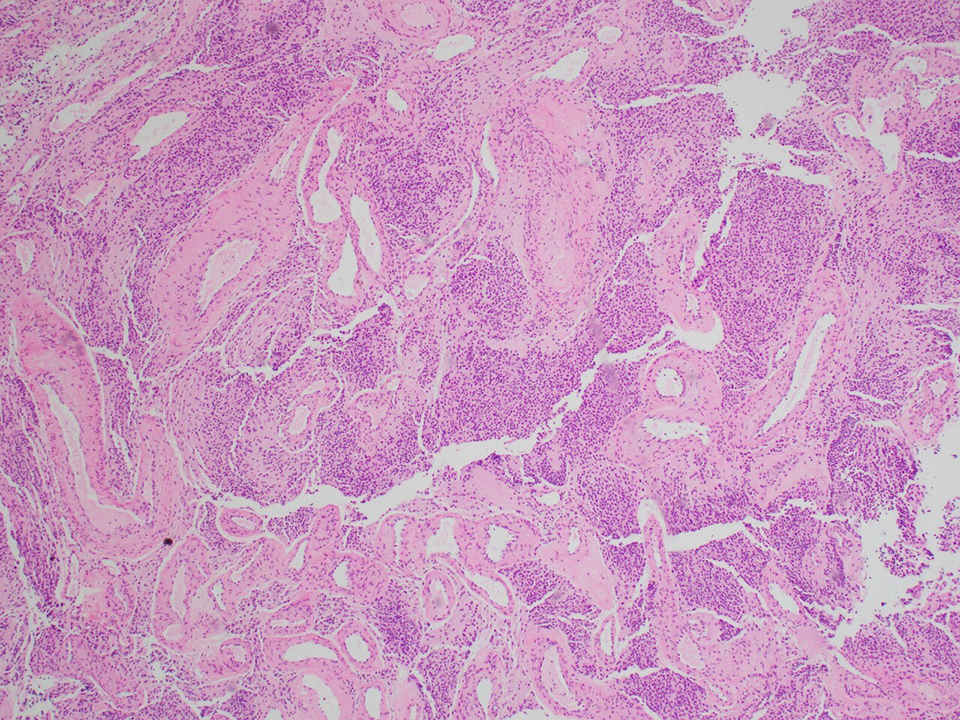
Pathology with rosette formation is present, with eosinophilic fibrillary matrix and prominent vessels. The cells are strongly positive for neuron-specific enolase. S-100 highlights peripheral sustentacular cells.
There was a positive margin remaining in the left maxillary and anterior ethmoid sinuses. One month later, a left medial maxillectomy was performed. Final pathology demonstrated a 1-mm focus of residual ONB at the left medial/orbital floor junction with a clear margin.
The patient’s sodium normalized postoperatively at 143 mEq/L and has remained within the normal range for the last 5 years. Left intermittent epiphora was the sole complication and was addressed with open dacryocystorhinostomy 4 years after tumor resection. No cervical metastases were observed. Radiation oncology followed the patient and decided that external beam radiation therapy was not necessary. The patient has remained disease-free for more than 5 years.
Discussion
Olfactory neuroblastomas are frequently diagnosed late because of their nonspecific and unremarkable symptoms. 3 This is of clinical importance, as survival rates decrease significantly in more advanced stages. The ONB is often staged using the Kadish staging system. Kadish A is limited to the nasal cavity, Kadish B is limited to the nasal and paranasal sinuses, and Kadish C is characterized by spreading outside of the nasal and paranasal sinuses. 11 Kadish D can also be used to describe the involvement of cervical or distal metastases. 12
The patient in the above case presented with a Kadish B malignancy. Symptomatic paraneoplastic syndrome resulted in early recognition and treatment of this malignancy. The majority of ONB are discovered as Kadish C, and the survival rates are as follows: Kadish A: 75% to 91%; Kadish B: 68% to 71%; and Kadish C: 41% to 47%. 2 However, it is important to note that metastases can develop regardless of tumor staging. 2
Syndrome of inappropriate antidiuretic hormone secretion is an uncommon, yet known paraneoplastic syndrome seen in 1% to 2% of all patients with cancer. 13 Syndrome of inappropriate antidiuretic hormone secretion is characterized by hypotonic plasma, hyponatremia, increased sodium excretion in urine, high urine osmolality relative to plasma osmolality, lack of edema, and normal renal function. 14 The patient in this case presented with the sole symptom of hyponatremia. No sinonasal complaints were observed.
Syndrome of inappropriate antidiuretic hormone secretion is seen in only 3% of head and neck cancers, 15 and ONB represents only 3% of sinus and nasal malignancies. 1 This makes SIADH induced by ONB exceptionally rare. The first description of SIADH induced by ONB was in 1967, 16 and as previously mentioned, there are 41 cases in the literature of functional ONB inducing SIADH. 4 -10
Tumors causing paraneoplastic SIADH in the head and neck are most commonly squamous cell carcinomas of the oral cavity, pharynx, and parapharyngeal space. The second most common functional malignancies of this category are ONB of the sinonasal cavity, small cell neuroendocrine carcinoma, adenoid cystic carcinoma, and undifferentiated carcinomas. 17 Despite their infrequent occurrence, the functional properties and symptoms of these malignancies are worth considering because of their utility in the diagnosis of head and neck malignancy.
In cases of SIADH secondary to ONB, SIADH is discovered before the diagnosis of ONB 76% of the time. 18 As in the case of this patient, SIADH was discovered before the ONB. This ultimately led to the discovery of the malignancy before the development of CNS involvement or regional or distant metastasis. The fact that this tumor was secretory, resulting in SIADH, has allowed serologic follow-up as a marker to indicate that he remains free of disease. However, it is important to note that ONB with SIADH can dedifferentiate into non-SIADH-inducing metastases. 19
Conclusion
When evaluating a patient with SIADH of unknown origin, it is important to consider functional malignancies, including those of the head and neck, as part of the differential diagnosis. If head and neck etiology is suspected, this should be further evaluated with contrast-enhanced CT or MRI followed by otolaryngology evaluation.
Footnotes
Authors’ Note
Verbal informed consent was obtained from the patient for their anonymized information to be published in this article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.