
Abstract
Hemangiomas of the head and neck account for about 7% of all benign tumors in children. Τhey are rare in the nasal cavity and especially in the nasal septum. Only 16 cases of intranasal hemangiomas in childhood have been previously described in the literature and 6 of them arising from the nasal septum. We present a rare case of a nasal septum hemangioma (NSH) in a 9-year-old boy who was treated with transnasal endoscopic resection.
Case Description
Α 9-year-old boy was referred to the ear, nose, and throat department of Papageorgiou general hospital from the district hospital of Veroia with active nose bleeding and a 6-month history of recurrent left-sided nasal epistaxis and obstruction. No other symptoms were reported. The patient had not a similar family history. Anterior rhinoscopy and endoscopic examination of the nasal cavities demonstrated a hemorrhagic pedicled mass, 0.8 × 0.7 × 0.5 cm in size, arising from the left side of the anterior septum (Figure 1).
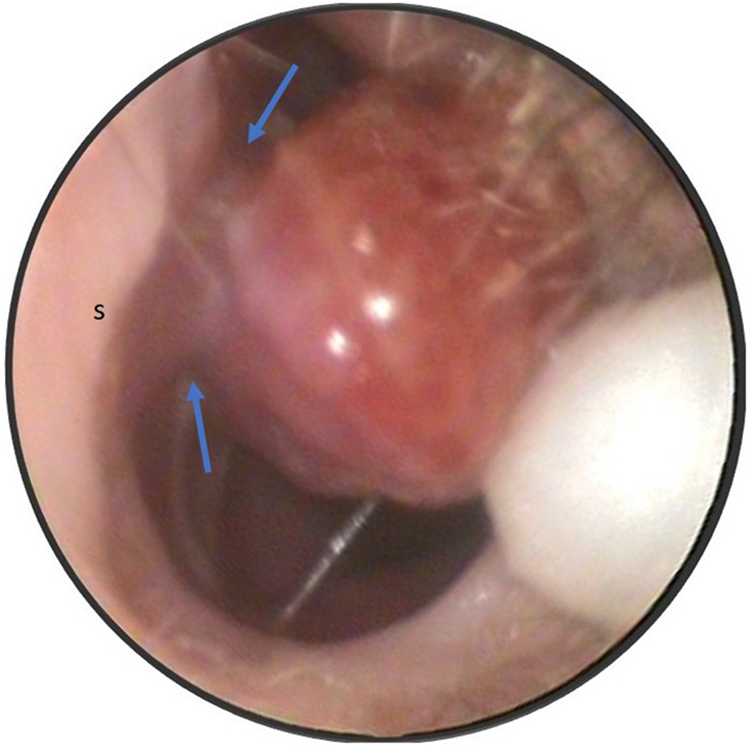
Endoscopic image of hemangioma arising from the left side of the anterior nasal septum (blue yellows: hemangiomas pedicle, s: septum).
An emergency endoscopic resection of the bleeding lesion under general anesthesia was decided. The mass was excised en block with its pedicle endoscopically under general anesthesia using bipolar diathermy and 0° 4-mm nasal endoscope (Figure 2). Packing of left nasal cavity was done and was removed on the second day of hospitalization. After the treatment, the symptoms of epistaxis and nasal obstruction controlled effectively. The little patient was discharged on the second postoperative day. Histopathological and immunohistochemical examination of the specimen revealed a capillary hemangioma of the nasal septum (Figure 3). No other hemangioma was revealed at any other location in patient’s body from the clinical examination. The boy remains symptom-free on 6 months follow-up with no evidence of NSH recurrence.

Postoperative image of the mass.
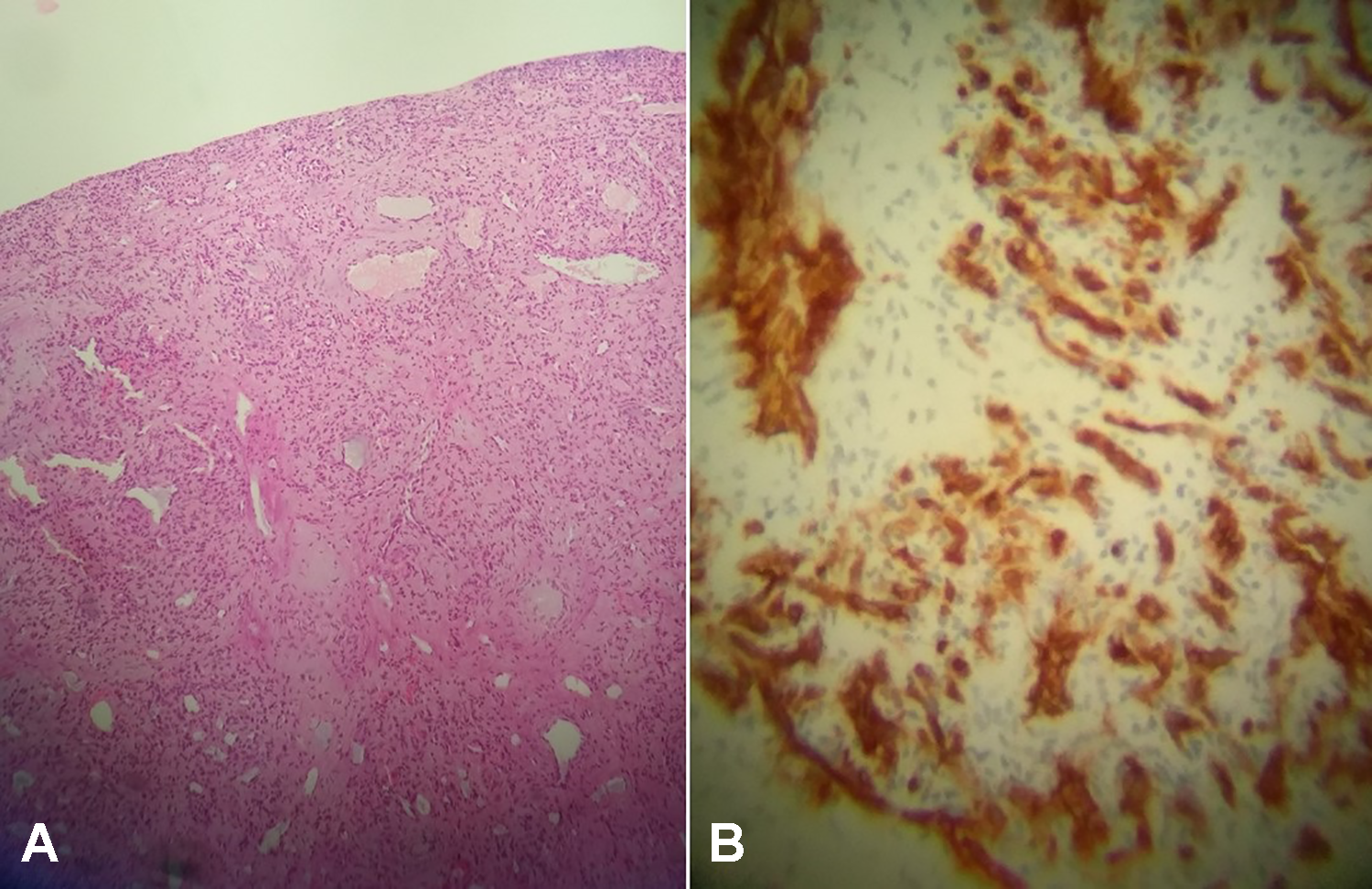
Histopathological and immunohistochemical examination showing nasal hemangioma. (A) nasal lesion with architectural proliferation of small dilated capillary spaces (H&E, ×20) and (B) strong positive immunochemical staining for CD34 which confirms the vascular nation of the proliferation (CD34 staining, ×10). CD indicates cluster of differentiation; H&E, hematoxylin and eosin.
Discussion
Hemangiomas are growing benign lesions that occur in skin and mucous membranes. Nasal septum hemangioma represents for about 31% of the entities of intranasal hemangiomas in adults. 1 Although hemangiomas are common lesions of the head and neck in children. Nasal cavity hemangiomas and especially NSH are extremely rare in childhood. To our knowledge, only 16 cases of intranasal hemangiomas in childhood have been previously described in the literature from 1980 since 2021 and 6 of them arising from the nasal septum. 2 -4 This is the seventh clinical report of NSH in children in the literature. The majority of the children were older than 5 years old and only 2 cases were infants. 2
The origin is unknown. Trauma and hormonal factors may play a role in the pathogenesis of the hemangioma. 3 There are 3 characteristic histologic subtypes: capillary, cavernous, and mixed hemangiomas. The subtype of capillary hemangioma occurs more often on the nasal septum in children. Whereas cavernous hemangioma occurs on the lateral nasal wall mainly in adulthood. On macroscopic examination, hemangioma may have a smooth surface, a polypoid, or a lopped pattern. 5
The signs and symptoms of intranasal hemangioma are mainly epistaxis, nasal obstruction, rhinorrhea, and pain. 1 -7 The most common symptom is nose bleeding and especially in children bleeding can result in rapid hemodynamic imbalance. 2,6 Differential diagnosis of NSH in a child with these clinical signs includes foreign bodies, hemangiopericytoma, juvenile nasopharyngeal angiofibroma, meningocele, dermoid cyst, schwannoma, glioma, and so on. 2,3,7
Εndoscopic examination is necessary to diagnose intranasal hemangioma. Generally, it presents as a red or purple mass that bleeds easily in touch at endoscopy. Important role in diagnosis have the radiological images. On computed tomography scan intranasal hemangioma appears as a well-defined and homogeneous soft tissue mass. 1 -3 In children, magnetic resonance imaging is more effective in diagnosis because MRI has no radiation exposure, which is very important for them. On MRI, the lesion appears with hyperintensity in T2 and spontaneous hypointensity in T1. 2,6
Intranasal hemangioma’s treatment is very important for avoiding complications and infections of the head and neck. The treatment of choice is the endoscopic excision with histologically clear resection margins. Although various therapeutic approaches have been developed including electrocoagulation, laser, excisional surgery following angiography with embolization, and cryotherapy. 2,4,6 The most common therapeutic approach is the endoscopic excision with bipolar electrocautery because it offers hemostasis. 2 The recurrence rate of these hemangiomas varies from 0% to 42%. 6
Footnotes
Authors’ Note
The authors declare that written informed consent for patient information and images to be published was provided by the patient.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.