
Abstract
Central retinal artery occlusion (CRAO) is an ophthalmic emergency and has poor visual prognosis. It is commonly found in elderly people and very rare in child. We reported an 8-year-old girl who suffered from acute sinusitis, periorbital swelling, and the visual acuity of her right eye was only light perception. She was diagnosed with CRAO, SPOA (subperiosteal orbital abscess), and acute sinusitis. Emergency treatments including surgery, antibiotics, glucocorticoids, intraocular-pressure-lowering drugs, and vasodilators were taken immediately in order to save the eyesight. The visual acuity of the right eye returned to 20/400. Conclusions: Severe intraorbital complications of acute sinusitis can lead to CRAO. Timely drainage, strong antibiotics, and glucocorticoids are the most effective methods for the treatments.
Introduction
Acute sinusitis is the main cause of intraorbital complications. Subperiosteal abscess usually does not cause severe vision loss, let alone central retinal artery occlusion (CRAO). Central retinal artery occlusion is one of the ophthalmic emergencies that cause sudden loss of vision. It is commonly found in elderly people with high blood pressure, arteriosclerosis, and other diseases. The main reason is that emboli block the central retinal artery and result in severe vision loss, even blindness. 1 Central retinal artery occlusion in children resulting from subperiosteal orbital abscess (SPOA) due to acute sinusitis is extremely rare.
Case Report
An 8-year-old girl presented to our hospital and she developed bilateral nasal congestion, pus discharge, and cough 2 weeks ago due to a “cold.” The symptoms were significantly alleviated after anti-infection treatment at a local clinic. Six days ago, the patient’s nasal congestion and purulent nasal discharge increased, accompanied by swelling and pain in the right eye and face and difficulty in opening the eye; however, her visual acuity was normal. She was hospitalized at a local hospital and diagnosed with acute sinusitis and orbital cellulitis. After the infusion of antibiotic and glucocorticoids, her symptoms were alleviated. Twelve hours before she came to our hospital, the swelling and pain of the patient’s right eye suddenly worsened. The girl’s eyeball protruded, and her vision decreased obviously. Her right maxillofacial region and forehead were swollen and painful, and the left eye began to swell. She was urgently presented to our department and was admitted to the hospital.
Her body temperature was 37.7°C. The signs included bilateral nasal congestion and edema, purulent nasal discharge, and sinus tenderness. The right eyelid was very swollen, the orbital pressure was high, and proptosis and chemosis were observed. The visual acuity of the right eye was only light perception. The pupil was 6 mm in diameter, direct light reflection disappeared, indirect light reflection was present, and the left eyelid was also swollen (Figure 1). Her leukocyte count was 22.29 × 109/L, neutrophil percentage was 80.6%, and high-sensitivity C-reactive protein was 28.58 mg/L. Computed tomography (CT) scan: The right nasal sinusitis involved the right orbit, and SPOA was present (Figure 2). Fundus examination showed edematous optic disc, pale retina, thickened veins, narrowed arteries, and cherry red spot (Figure 3). Initial diagnosis: (1) CRAO, (2) SPOA, (3) acute sinusitis. Based on the consultation opinions of ophthalmology and clinical pharmacy, linezolid, methylprednisolone, and mannitol infusion and vasodilator therapy were given. On the day of admission, the patient underwent incision and drainage by nasal endoscopic surgery. During the operation, a large amount of purulent secretion overflowed after part of the lamina papyracea was removed. Granulation hyperplasia was seen between the orbital fascia and the lamina papyracea. Magnetic resonance imaging (MRI) on the 12th day after operation showed that the right eyeball protrusion and orbital soft tissue swelling nearly disappeared (Figure 4). Her visual acuity gradually improved until to 20/400. The result of bacterial culture was methicillin-resistant Staphylococcus aureus (MRSA).

Preoperative photograph of patient.
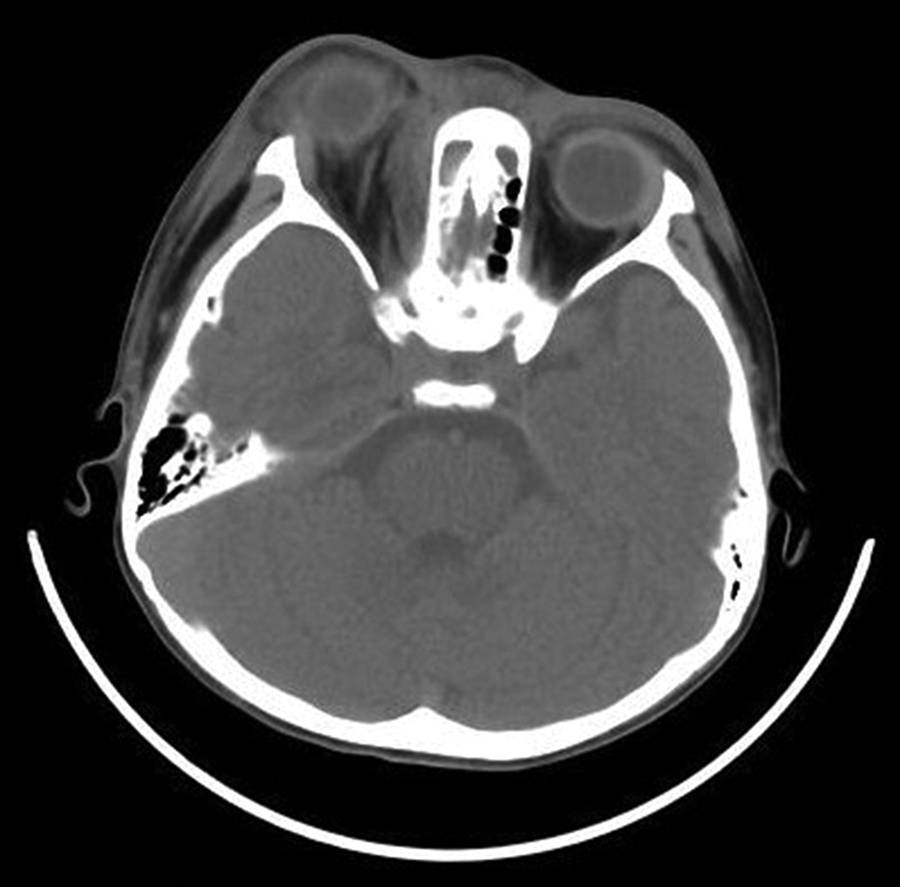
Preoperative computed tomography (CT) scan illustrating a mass lesion compressing the medial rectus muscle.
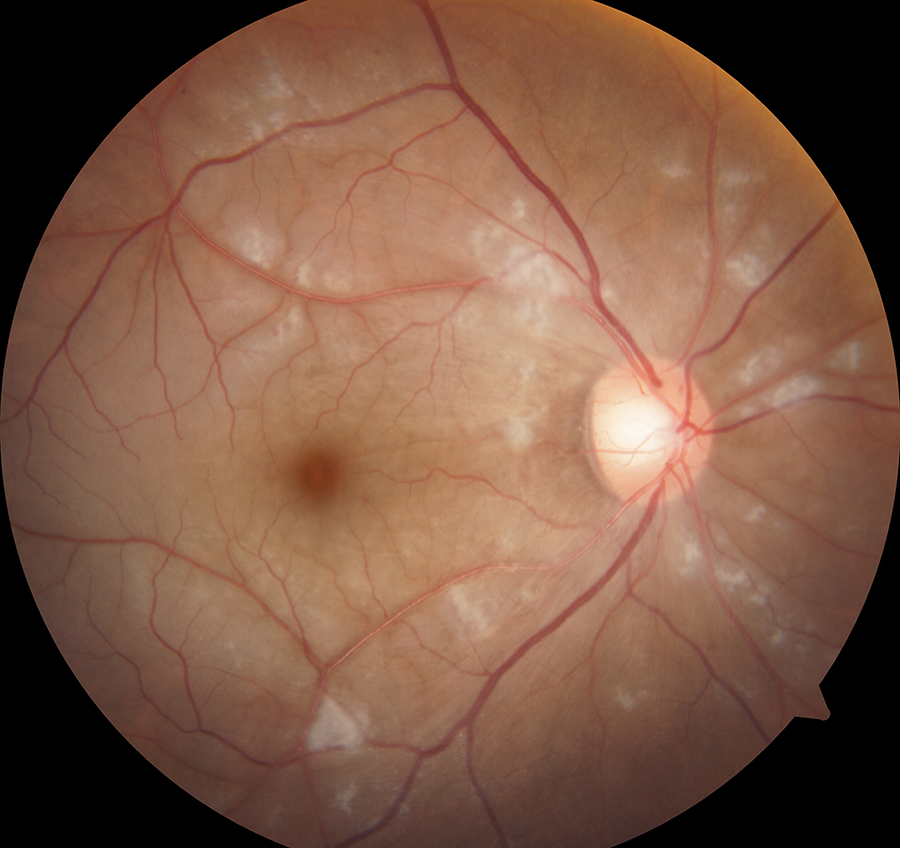
Fundus examination of patient with edematous optic disc, pale retina, thickened veins, narrowed arteries, and cherry red spot.
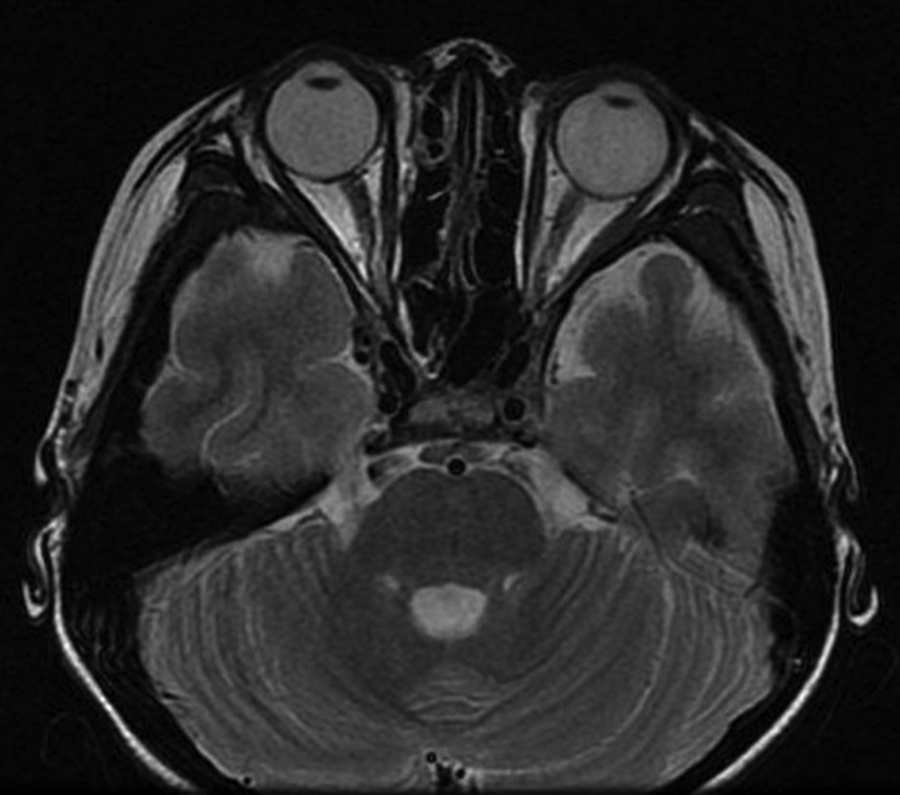
Magnetic resonance imaging (MRI) scan illustrating the lesion vanished.
Discussion
Central retinal artery occlusion is an acute ischemic disease of the retina caused by obstruction of the central retinal artery. It is an ophthalmic emergency that causes severe or complete loss of visual function in patients. Fundus examination shows edematous retinas, significantly narrowed arteries, beaded blood vessels, and cherry red spots in the macular area. According to literature, CRAO is mainly caused by vascular embolism due to atherosclerosis, the cause of which accounts for more than two-thirds of CRAO cases. 2 Most CRAO cases occur in elderly people with hypertension, diabetes, heart disease, and carotid atherosclerosis. 3 Central retinal artery occlusion caused by sinusitis is extremely rare. 4 In our case, the patient is a child with normal body development and normal biochemical indicators, showing normal blood glucose and blood lipids. Thus, atherosclerosis as etiology can be ruled out. The sudden loss of vision occurs after 2 weeks of sinusitis. The possible reason is considered to be intraorbital infections, leading to increased intraocular pressure (IOP). The compression of the central retinal artery leads to the occurrence of CRAO.
For the timing of surgery for orbital complications of sinusitis, the European EPOS guidelines issued in 2020 pointed out: ① Evidence of subperiosteal or intraorbital abscess in CT or MRI (with potential exception for small volume abscesses); ② Reduced visual acuity/reduced color vision/affected afferent pupillary reflex or inability to assess vision; ③ Progression or no improvement in orbital signs (diplopia, ophthalmoplegia, proptosis, swelling, chemosis) after 48 hours intravenous antibiotics; ④ Progression or no improvement in the general condition (fever, infection parameters) after 48 hours of intravenous antibiotics. 5 Acute sinusitis complicated by orbital abscess and visual loss is an important indication for immediate surgery. Studies have shown that CRAO is an ophthalmic emergency, and the longest window of emergency intervention is 4 hours. After 4 hours, the retina will undergo irreversible damage 6 ; thus, early diagnosis and treatment are essential to save vision. At present, there is no recognized effective treatment for CRAO. 7 In this case, the patient’s vision was only light perception at the time of admission. Antibiotics, IOP-lowering drugs, vasodilators, and glucocorticoids were immediately given. To preserve her vision, IOP should be quickly reduced. Hence, sinus opening and drainage of the abscess should be performed as soon as possible. The patient’s visual acuity had already decreased 12 hours at the moment of hospitalization, which was far beyond the optimal time point for visual recovery. However, her visual acuity returned to 20/400 after treatment. Compared with the majority of CRAO patients with vision loss or only light perception, the patient’s visual recovery was quite ideal.
Given that CRAO due to sinusitis is extremely rare, corresponding consensus or guidelines are lacking. Thus, we can only formulate treatment based on experience. Recalling the treatment of this patient, we considered that the most effective measures included ① drainage of abscesses as early as possible, ② effective antibiotics, and ③ appropriate application of glucocorticoids. Studies have shown that the main pathogenic bacteria of orbital cellulitis and orbital abscess are Staphylococcus and Streptococcus. 8 Other bacteria such as Haemophilus influenzae, Moraxella catarrhalis, and anaerobic bacteria may also be included. Therefore, second- or third-generation cephalosporins can be used for mild cases. If anaerobic infections are considered, metronidazole can be added. For severe cases, especially intraorbital infections caused by MRSA, the literature recommends vancomycin. 9 In addition, we believe that linezolid is more advantageous than vancomycin for severe cases that affect vision or life. This is because ① linezolid has a strong effect on Gram-positive cocci and anaerobic bacteria, ② linezolid has a good effect on MRSA, ③ linezolid is fat-soluble and has less side effects than vancomycin, and ④ critically ill patients are in a dangerous condition, and the infection should be controlled as soon as possible. Vancomycin is inferior to linezolid because of its tissue permeability, especially for skin and soft tissue infections. Its efficacy is poorer than that of linezolid. The antibiotics should be reduced according to the drug sensitivity results when the patient’s condition is stable.
At present, considering that large doses of glucocorticoids may cause the spread of infection and adverse consequences, the use of these drugs still has some controversies, especially for children. However, some studies show that the use of steroids in the treatment of orbital cellulitis can accelerate clinical improvement, shortens hospital stay, and does not cause obvious adverse reactions. 10,11 In this case, the patient’s vision had decreased to light perception at the time of consultation; thus, there was a need to control inflammation, reduce IOP, and relieve compression as soon as possible. Rapid relief of her symptoms cannot be easily achieved only by abscess drainage and antibiotics. With the use of strong antibiotics to prevent the spread of infection, the short-term application of large doses of glucocorticoids can ease the symptoms rapidly. Calcium supplements and gastric mucosal protective agents are often applied to counteract the side effects of glucocorticoids. Therefore, we believe that the application of glucocorticoids is necessary in severe intraorbital infections, especially in the case of decreased vision. However, evidence-based medicine is still needed to determine its specific effects and adverse reactions.
Footnotes
Authors’ Note
Xiumei Chen and Xuejing Man contributed equally to this article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.