
Abstract
Facial nerve schwannomas are rare, benign, slow-growing tumors that can occur in any segment of the facial nerve, although 71% of cases are intratemporal. Surgical resection can lead to facial nerve injury. Facial function recovery after reanimation is usually not better than House-Brackmann (HB) grade III. Thus, for cases of intratemporal facial nerve schwannomas (IFNSs) with favorable facial function (HB grade I or II), observation by periodic magnetic resonance imaging is the mainstay of management. Here, we present a case of a large IFNS with normal facial function in which the mass fully occluded the external auditory canal. The occlusion caused squamous debris to accumulate, potentially leading to cholesteatoma. Faced with this therapeutic dilemma, we chose surgical resection with the patient’s informed consent. Stripping surgery was achieved with normal postoperative facial function. There was no postoperative facial paralysis or recurrence at 2-year follow-up. We describe the experience of diagnosis and treatment process for this case, and discuss the possibility of total resection of the tumor with preserving the integrity of facial nerve.
Introduction
Facial nerve (FN) schwannomas are rare, benign, slow-growing tumors derived from Schwann cells. 1 Although they can occur in any segment of the FN, 71% of cases are intratemporal. 2 The most common clinical sign of intratemporal facial nerve schwannoma (IFNS) is facial paralysis. 1 Surgical resection with reconstruction is the standard management for patients with House-Brackmann (HB) grade III or worse, as facial function recovery is rarely better than HB grade III. 3 To retain favorable facial function as long as possible, observation with periodic magnetic resonance imaging (MRI) is generally advocated for patients with HB grade I or II. 4
However, large IFNS may completely occlude the external auditory canal (EAC), potentially leading to cholesteatoma. 5 In such cases, surgical resection is justified despite good facial function. Here, we present a case of a 50-year-old woman with an EAC mass and normal facial function caused by a large IFNS.
Case Report
A 50-year-old woman presented with gradual left hearing loss, occasional dizziness for 10 years, and tinnitus for 5 years. She had felt aural fullness for one month. There was no history of otalgia, otorrhea, or episodic vertigo. Her facial function was normal. Otoscopy revealed a smooth-surfaced reddish mass filling the left EAC. The mass was fixed interiorly, but the tympanic membrane and the root of the mass could not be seen. Audiogram demonstrated left mixed-type hearing loss of 76 dB with a 25-dB air–bone gap. High-resolution computed tomography revealed a soft tissue mass filling the left tympanic cavity, which was protruding into the EAC and displacing the ossicle laterally. The cochlear erosion was smooth and sharply marginated. The fallopian canal of the tympanic segment was eroded. The ossicular chain was disrupted (Figure 1A and B). Contrast-enhanced MRI showed a heterogeneously enhanced soft tissue lesion filling the left tympanic cavity with extension to the EAC. The lesion presented with an isointense signal on T1-weighted images and an iso-to-hyperintense signal on T2-weighted images (Figure 1C-F).
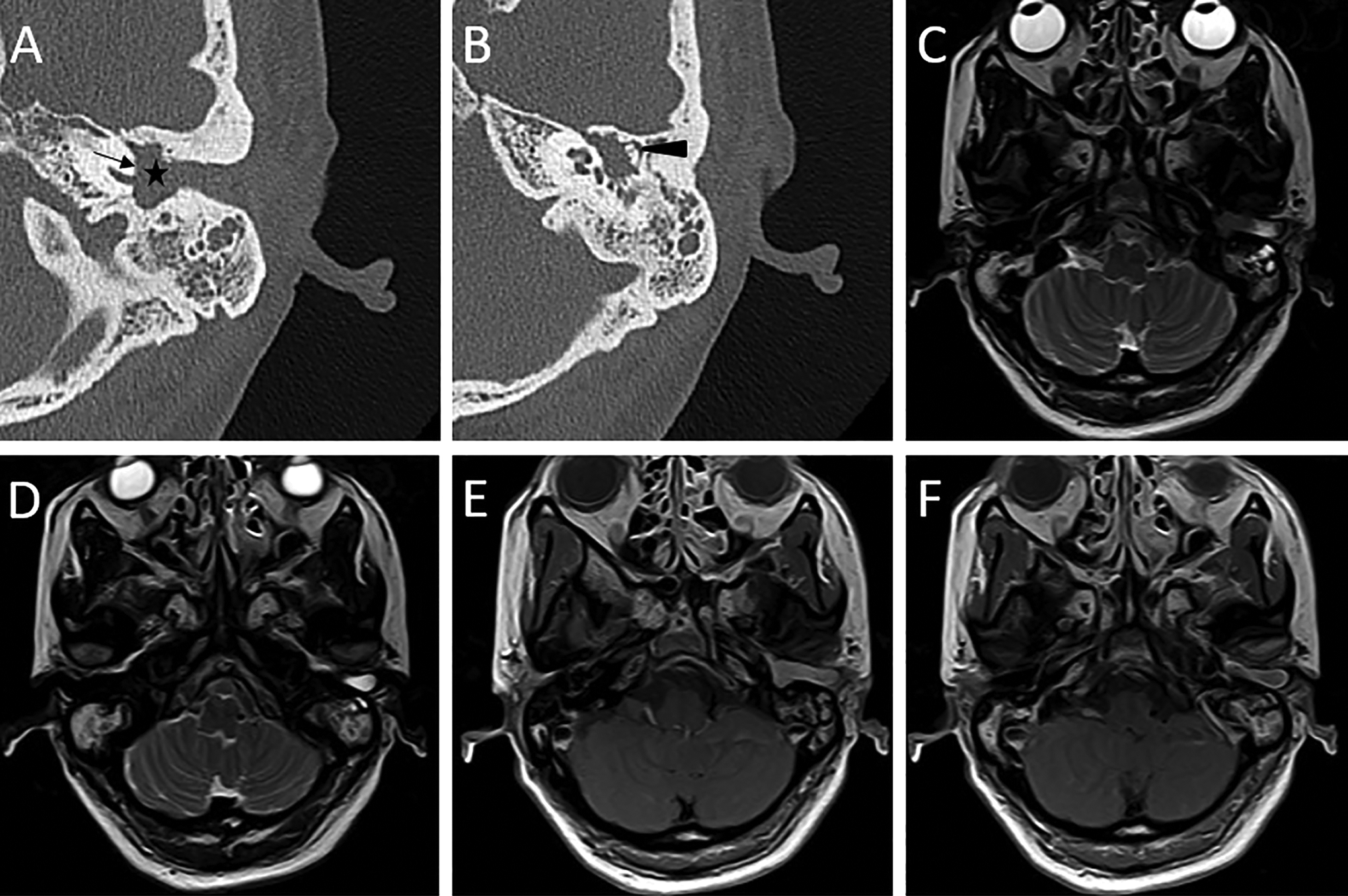
High-resolution computed tomography (HRCT) and contrast-enhanced magnetic resonance imaging findings. Axial HRCT (A, B), axial T2-weighted images (C, D), and contrast-enhanced axial T1-weighted images (E, F) of the left temporal bone show the soft tissue lesion filling the left middle ear cavity with an extension to the external auditory canal, which is causing bony erosion of the tympanic segment of the facial nerve (A, star) and displacing the ossicle laterally (B, arrowhead). The lesion also caused smooth and sharply marginated erosion of the cochlea (A, arrow). (C-D) It presents with an iso-to-hyperintense signal on T2-weighted images. (E, F) The lesion is heterogeneously enhanced.
A diagnosis of IFNS was suspected. As complete occlusion by the EAC mass caused squamous debris to accumulate, there was a high risk of cholesteatoma formation. Thus, surgical resection was adopted with the patient’s informed consent. We performed a transcanal biopsy for pathological diagnosis. The encapsulated mass was slightly indurated and occluded the entire EAC (Figure 2A). The pathology demonstrated a soft fibroma. Then, the patient underwent the transmastoid approach. The encapsulated reddish tumor was found to originate from the tympanic segment of FN. Due to the large size of the tumor, total resection may cause postoperative facial paralysis. It was decided to prioritize the preservation of facial function instead of complete tumor resection. Aided by intraoperative electrophysiological monitoring, we removed the nonstimulating portion of the tumor, achieved complete local exposure, and identified the plane of separation between FN and the tumor (Figure 2B). The tumor was completely removed with an anatomically intact FN. Pathological examination confirmed the diagnosis of a schwannoma. There was no postoperative facial paralysis or recurrence at 2-year follow-up.
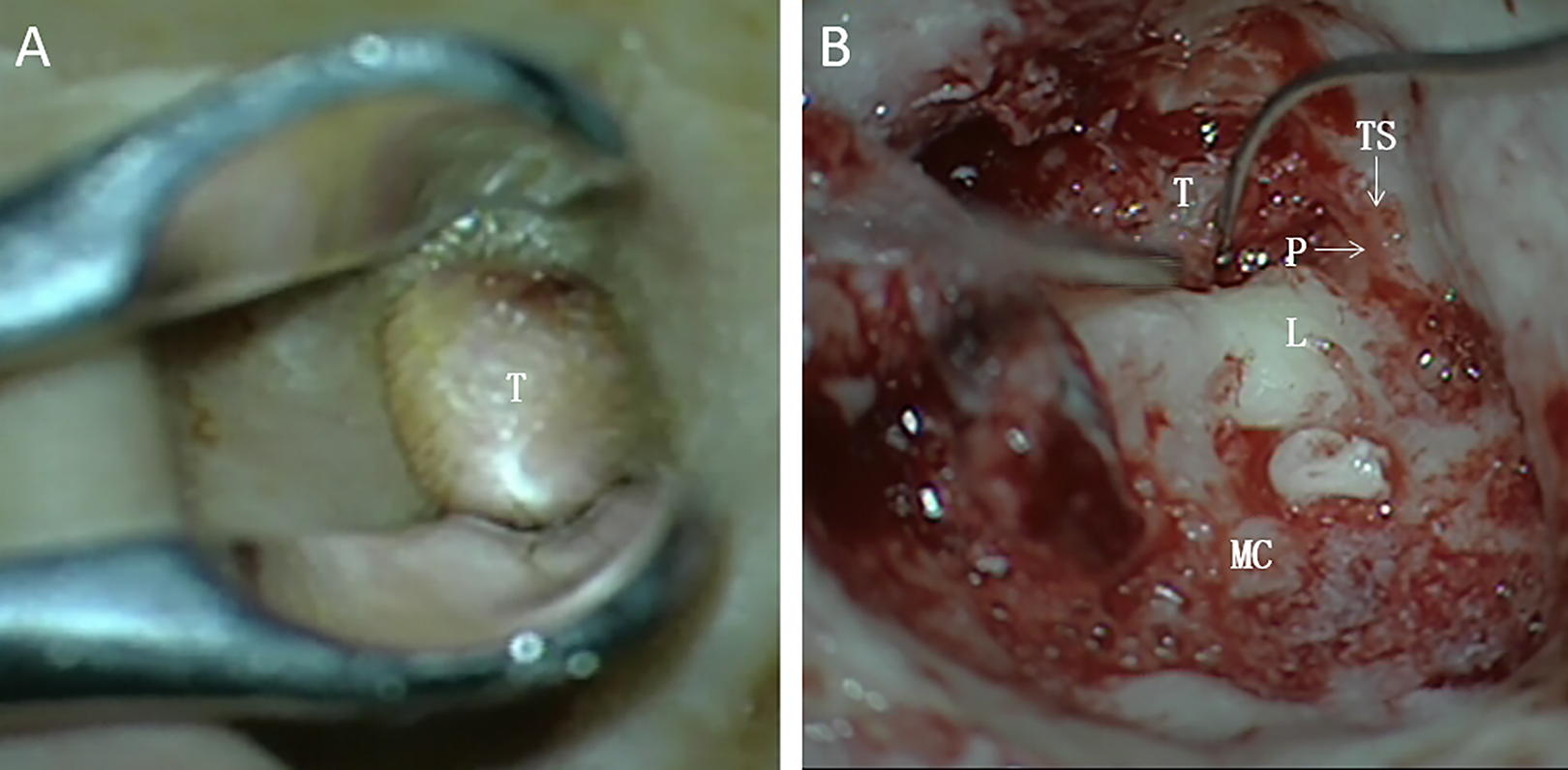
Intraoperative findings. Intraoperative microscopic image of biopsy (A) shows the encapsulated mass occluding the entire external auditory canal (EAC). Intraoperative microscopic image of stripping surgery (B) shows the good dissection plane of the facial nerve and tumor. L indicates lateral semicircular canal; MC, mastoid cavity; P, the plane of the facial nerve and tumor; T, tumor; TS, the tympanic segment of the facial nerve.
Discussion
According to pathologic features, IFNSs are classified as outgrowing IFNSs which originated from the perineurium at the dehiscence of the FN canal, and ingrowing IFNSs which originated from the center of FN. 6 Outgrowing IFNSs herniate out of the bony canal result in a pedunculated mass, and rarely compress the normal FN. Most outgrowing IFNSs originate from the tympanic segment of FN. These tumors extend to the tympanic cavity along the path of least resistance, and even protruded through the tympanic membrane to form EAC masses.
An IFNS presenting as an EAC mass is extremely rare. Biopsy can worsen facial function because the FN fibers may be scattered throughout the tumor or intimately adherent to the tumor surface. 7 Biopsy is not always helpful, as in the presented case. Correct preoperative diagnosis of IFNS can be difficult because of its rarity, nonspecific symptoms, and indistinguishable radiological findings. It is often misdiagnosed with otitis media, cholesteatoma, or glomus tumor. 8 -10 Therefore, surgical exploration is often required to diagnose.
The main trunk of the FN may be obscured by large tumor, and in an attempt to remove the mass, the FN can be unintentionally injured or transected. Facial function recovery after reanimation is usually not better than HB grade III. 3 Thus, observation with periodic imaging surveillance is recommended for patients with HB grade I or II to retain favorable facial function as long as possible. 4 However, in our case, complete occlusion of the EAC by the mass potentially led to cholesteatoma. Thus, observation was not appropriate for this situation despite normal facial function.
Stereotactic radiosurgery provides a good tumor control for IFNS; however, in many cases, this reflects a stabilization in growth. 11 It is unlikely to relieve the propensity for conductive hearing loss, otitis externa, and cholesteatoma formation. Stereotactic radiosurgery leads to transient tumor swelling and consequent desquamation, which increases the accumulation of keratin, thereby at higher risk for cholesteatoma 5 . Thus, we chose surgical resection in the presented case.
Theoretically, radical dissection with FN preservation can be achieved by stripping the nerve sheath, in a process similar to “acute demyelination.” 12 However, the FN fibers may be scattered throughout the tumor, making it impossible to identify the plane. 7 During the operation, priority was placed on preserving facial function and not necessarily total resection of the tumor. The tumor was removed through careful piecemeal bulk reduction by intraoperative monitoring until a good dissection plane between the tumor and FN was recognized. Stripping surgery was achieved with normal postoperative facial function.
Conclusion
The preoperative diagnosis of an IFNS is difficult to establish. Observation with periodic MRI is generally advocated for patients with HB grade I or II. The primary goal in managing IFNSs that occlude the EAC is to avoid cholesteatoma formation and maintain favorable facial function as long as possible. Surgical resection should be performed aided by intraoperative monitoring. During the operation, priority is placed on preserving facial function and not necessarily total resection of the tumor. If a good dissection plane of the FN and tumor is able to be recognized, surgeons can completely remove the tumor with FN preservation.
Footnotes
Authors’ Note
Written informed consent was obtained from the patient(s) for their anonymized information to be published in this article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.