
Abstract
First branchial cleft anomalies (FBCAs) are the most infrequent malformations that occur during the development of the branchial apparatus, appearing in less than 8% of all branchial anomalies. Traditionally, they are classified into Work type I and II, depending on their origin. We present a pair of rare FBCAs: a case of a preauricular Work type I cyst with twin fistulae coursing toward the parotid gland and a Work type II cyst of significant dimensions.
Case Description
Work Type I Cyst and Fistulae
A 10-year-old girl presented to our ear, nose, and throat (ENT) department with a history of recurrent episodes of purulent discharge from a left preauricural sinus. Magnetic resonance imaging (MRI) and computed tomography (CT) were performed revealing a cystic formation of 15 × 12 × 9 mm in size (Figure 1A). Firstly, a preauricular incision was made with the fistula probed. After dissecting at about 5 mm in depth, the cystic component was identified, with a diameter of approximately 2 cm. We identified a set of fistulae 2 cm long diving into the parotid gland, in close proximity to the facial nerve (Figure 2A). Intraoperatively, methylene blue was used to visualize the fistulae and their branches. Histopathological examination showed a Work type I first branchial cleft anomalies (FBCA) with skin and stratified squamous keratinized epithelium (Figure 3A). After a follow-up period of 10 months, no recurrence was noted.
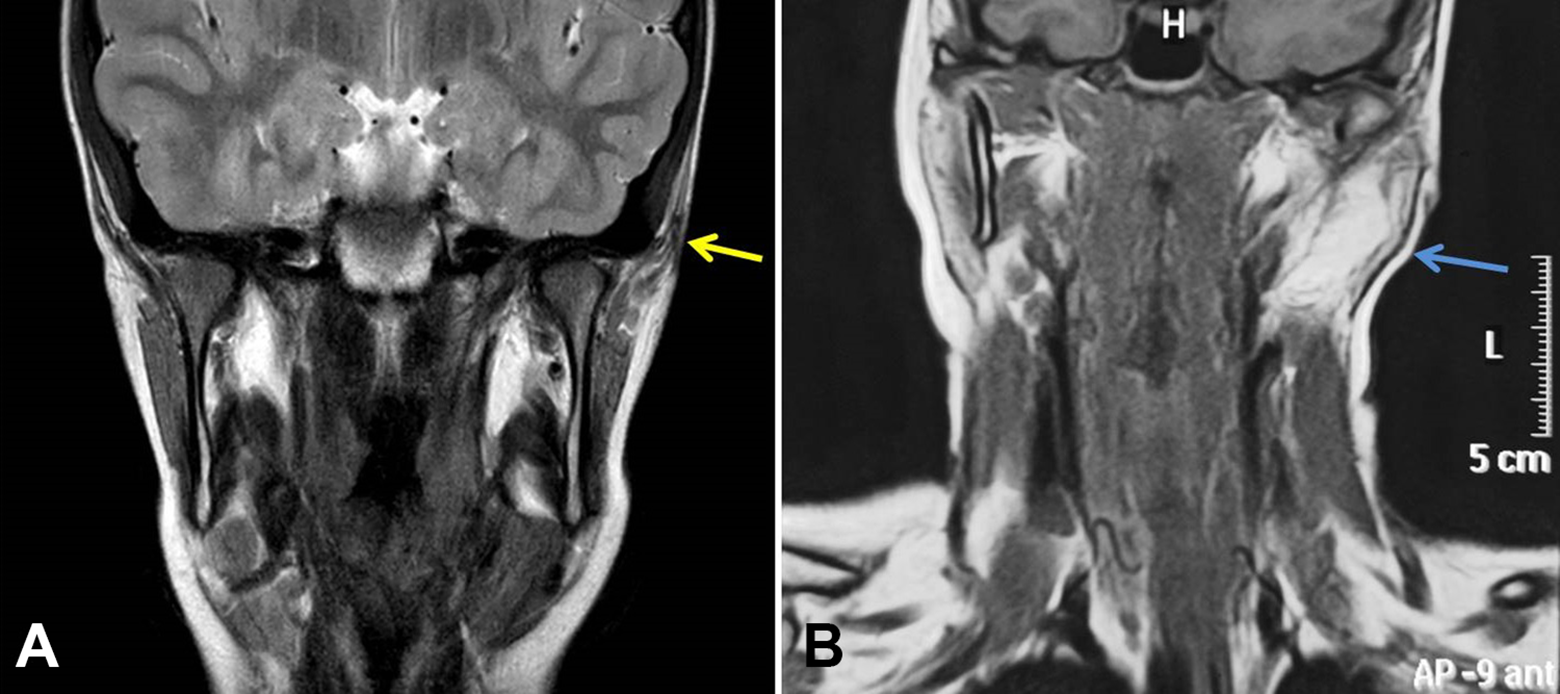
Magnetic resonance imaging (MRI) of FBCAs. Preoperative MRI in coronal plane, showing (A) the Work type I anomaly, with pathological T2 signal in the left superior parotid area (yellow arrow), and (B) the Work type II lesion inside the parotid gland with a high T2 signal (blue arrow). FBCA indicates first branchial cleft anomalies.
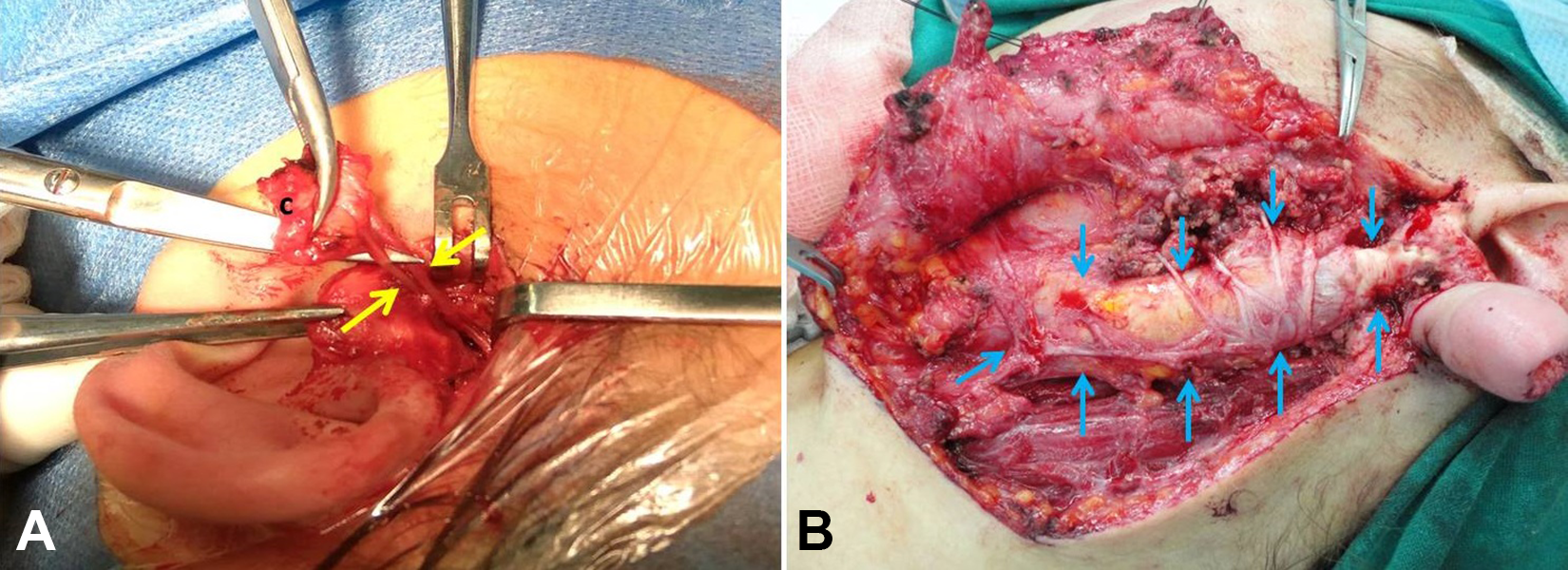
Intraoperative images of (A) dissection of the cystic part (c) and visualization of the twin fistulae (yellow arrows) diving toward the parotid gland of the Work type I anomaly, and (B) the Work type II cyst (blue arrows), visualized inside the parotid gland, in touch with the facial nerve branches and the great auricular nerve.
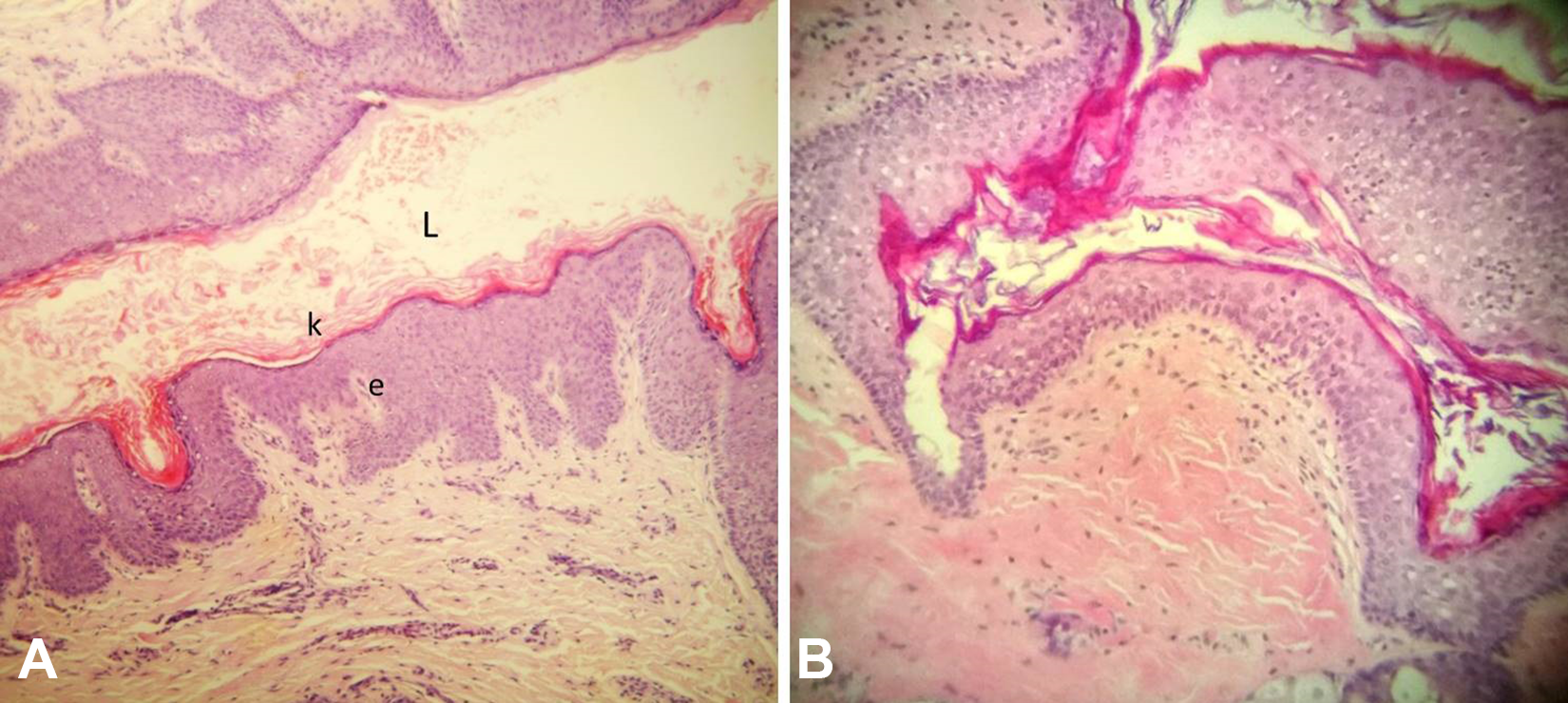
Histopathological examination showing (A) the fistula of the Work type I lesion with stratified squamous epithelium (e), with keratinization (k) and the lumen (L), and (B) stratified squamous keratinized epithelium covering the Work type II cyst (H&E, ×10). H&E indicates hematoxylin and eosin.
Work Type II Cyst
A 16-year-old female was referred to our ENT department with a 2-month history of a growing mass located at the left parotid and submandibular region. An ultrasound and a CT-scan revealed a large mass inside the left parotid gland, approximately 50 × 19 × 15 mm in size and mainly fatty in density. The MRI showed that the lesion had a high signal intensity in T1- and T2-weighted sequences (Figure 1B), and a low signal in fat suppression sequences. A superficial parotidectomy was performed and the mass was visualized, with the facial nerve surrounding it (Figure 2B). After meticulous dissection, with the use of electrophysiological monitoring of facial nerve, the mass was excised. Histopathological examination showed stratified squamous keratinized epithelium covering the cyst and the presence of cartilage, confirming the diagnosis of a Work type II FBCA (Figure 3B). There was no sign of recurrence during the 12-month follow-up period.
Discussion
Branchial cleft anomalies occur due to improper formation of the pharyngeal apparatus during embryonic development. Depending on the closure degree of the first branchial cleft’s ventral portion, they appear as a fistula, a sinus, or a cyst. 1 With that process being highly complex, their clinical presentation is varied, and therefore their treatment quite challenging. 2
First branchial cleft anomalies are the most uncommon of all the malformations of the pharyngeal apparatus, appearing in less than 8% of all cases. 3 -5 They are classified into 2 Work types, depending on their embryological origin. Unlike our 2 cases, type I anomalies are often diagnosed in adulthood, possibly due to mismanagement, while type II are identified shortly after birth or at childhood. 6,7
Type I anomalies arise due to the duplication of the membranous part of the external auditory canal (EAC). They are of ectodermal origin, containing only squamous epithelium. Usually, they are located in the postauricular region, or near the pinna, causing deformation of the concha or tragus. In addition, they develop superficially to the facial nerve, usually as a cystic formation.
Type II anomalies develop from the duplication of the membranous EAC and pinna. They originate from the ectoderm and mesoderm, with squamous epithelium, skin appendage, and cartilage present. They are located inside the parotid gland, laterally or medially to the facial nerve, rarely splitting its main trunk. The defect can extend from the EAC and the tympanic membrane, to the face and the upper neck region as a cyst, a sinus or a fistula. 8,9 The type II cyst that we present had significant dimensions, considering that it was diagnosed during adolescence.
Clinically, as in our cases, the appearance of a mass or a sinus in the postauricular or parotid region could suggest the diagnosis of a FBCA. Recurrent signs of inflammation and purulent discharge are frequent. Also, auricular symptoms of infection may be present, such as signs of inflammation and presence of pus inside the EAC. Differential diagnosis includes malignant and benign parotid neoplasms and cysts, parotitis, second branchial cleft anomalies, otitis media, and causes of head and neck lymphadenopathy. 7,10,11
Magnetic resonance imaging is the most accurate method in the diagnosis of FBCAs, because of its high-resolution in soft tissue differentiation and the absence of radiation. It can reveal valuable information about the size and consistency of the lesion, its relation to the parotid gland and neighboring structures, and a coexisting lymphadenopathy. Computed tomography-scanning with contrast material detects a cystic lesion with its wall thickness and enhancement varying, depending on tissue inflammation. Finally, ultrasound can be of assistance during the first diagnostic approach. 5,6,11
The treatment of choice is surgical removal of the anomaly, regardless of type or size, especially in cases of frequent infection and local symptoms. Relapse rate is low in a successful total excision, with a higher percentage in case of recurrent symptoms. 6,7,10
Footnotes
Authors’ Note
We declare that written informed consent for patient information and images to be published was provided by the patient.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article