
Abstract
Background:
Puncture and lavage of the paranasal sinuses, previously the primary treatment for unresponsive acute bacterial rhinosinusitis before surgery, has been abandoned due to procedural discomfort and advancements in antibiotic efficacy and endoscopic surgery. The rise in antibiotic-resistant bacteria has renewed the interest in minimally invasive sinus lavage to both avoid aggressive surgical interventions and identify appropriate antibiotic therapy. In this article, we describe the safety and feasibility of a new device in human patients and evaluate its efficacy as a treatment before the traditional sinus surgery in acute rhinosinusitis.
Methods:
The device with its seeker-shaped guiding tube and rotating wire can enter the sinus cavity through the natural ostium, pulverize the inspissated mucus, and enable lavage and culture sampling without the need for sinus puncturing. It was tested in 6 patients with chronic sinusitis under general anesthesia during endoscopic sinus surgery and in additional 10 patients with maxillary acute bacterial rhinosinusitis in outpatient settings under local anesthesia.
Results:
The device enabled rapid, efficient, and atraumatic insertion of the wire into the occluded sinuses. The rotating wire permitted pulverization of the thick mucus, which enabled irrigation without mucosal damage or adverse events. Overall, 9 of 10 patients with acute bacterial rhinosinusitis demonstrated remarkable improvements and were discharged the following day with no acute symptoms. The visual analog scale score for pain dropped from 8.9 to 0.4. The remaining one patient underwent endoscopic sinus surgery subsequently. None of the patients treated during endoscopic sinus surgery developed any adverse events.
Background
Acute rhinosinusitis (ARS) and acute exacerbations of chronic rhinosinusitis (CRS) are common diseases, 1 secondary to blockage of the natural sinus ostium due to a variety of reasons, such as impedance to mucus clearance. This results in the accumulation of mucus in the sinus, which often thickens and inspissates, thus resulting in facial pressure and pain. Although the disease is usually self-limiting, medical and surgical treatments may be warranted sometimes when pathogenic bacteria accumulate in the occluded sinus and natural immune processes cannot resolve the infection. 2
The commonly accepted first-line approach in ARS and acute exacerbations of CRS is watchful waiting 3 with saline irrigation and mucolytics followed by antibiotic treatment for acute bacterial rhinosinusitis (ABRS). Recent evidence suggests that antibiotic therapy does not shorten the disease duration, possibly, due to antibiotic-resistant bacteria. 3 -8 This has resulted in a cure rate of only approximately 71% 5 to 83% 6 following 2 weeks of treatment and failure rate of 10% over 2 months. 4 In some patients, the infection can last for weeks and evolve into subacute or CRS. Rarely, the infection may spread to the bloodstream or adjacent structures, such as the orbit, cranium, and lungs, which requires urgent surgical intervention. 3
Although balloon sinuplasty has popularly been used to treat CRS and recurrent ARS, information regarding its use in ARS is scarce. 9 It has been used to treat frontal ARS successfully 10 ; however, there are no clinical trials to support the procedure. For the management of acute or recurrent ARS while avoiding or minimizing antibiotic usage, a new sinus device (SinuSafe) was created to cannulate the ostium and break the inspissated mucus and remove it. SinuSafe enables sinus lavage via the natural opening without the need for puncturing, dilation, or trephination; it may fill the treatment gap between initial antibiotic failure and surgical intervention in some cases.
Methods
In the current study, we tested the safety and feasibility of SinuSafe in human patients and evaluated its efficacy as a treatment option before traditional sinus surgery for ARS. The clinical trial that examined the safety and feasibility of SinuSafe took place between January 2017 and December 2018, and included 3 parts; it was approved by the institutional ethical committee (Hillel Yaffe Medical Center Committee, No. 5582). Informed consent was obtained from all participating patients.
The SinuSafe Device
SinuSafe includes a 1-mm cannula and maxillary seeker–shaped guiding tube with 110° curve and nontraumatic tip that positions the cannula before the sinus opening (Figures 1 and 2). The shape assists in positioning the tube appropriately and sliding it around and beyond the uncinate process without the need for visualization of the anatomy. The tiny cannula enters the sinus cavity via the natural ostium, even if it is occluded, using the 0.35-mm motor-driven nitinol cable that can rotate up to 5000 rotations per minute within the cavity and cannula, which allows for irrigation and aspiration of liquids. The wire pulverizes inspissated secretions and breaks the mucin structure, 11 thus reducing its viscosity and enabling aspiration via the small 1-mm tube. The motor automatically stops when it encounters strong obstructions, thus avoiding any harm to the mucosa and sinus walls. The process requires an average of 60 seconds per sinus. The device is registered with the US Food & Drug administration (2017).

The SinuSafe device: (1) maxillary seeker–shaped cannula; (2) nitinol wire.
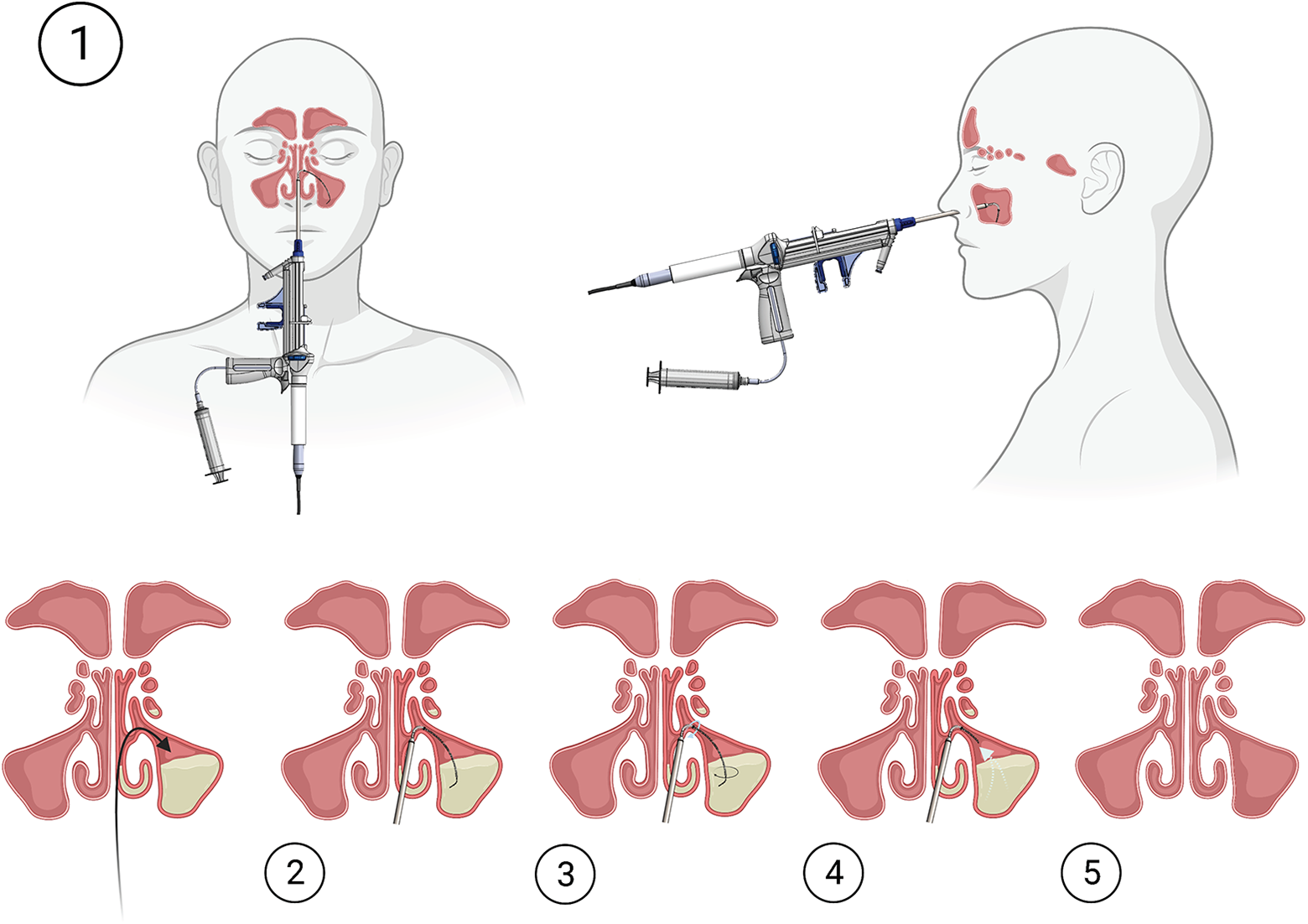
The SinuSafe device usage: (1) introduction through the natural ostium; (2) extension of the nitinol wire; (3) rotation of the wire; (4) sinus content suctioning; (5) clear sinus following the procedure.
Patients
The first 2 parts of the study were performed in the operating room (OR) during traditional endoscopic sinus surgery (ESS) for sinusitis under general anesthesia in clinically confirmed cases based on history, computed tomography (CT), and nasal endoscopy.
Patients with chronic maxillary sinusitis refractory to medical management demonstrated by history, nasal endoscopy, and CT were enrolled in the first and second parts of the trial. Computed tomography was performed at the time of diagnosis and within one month prior to the surgery.
During the first part, the cannula was tested to ensure that the device reached the ostium without harming the nasal pathway and sinus ostium; this was observed using 0° and 45° endoscopes.
The second part evaluated the safety and feasibility of cleaning the affected sinuses using irrigation, aspiration, and rotating wire. The subsequent effects on the sinus ostium and sinus mucosa were examined using 0° and 45° endoscopes. Postoperative sequelae were examined as well.
In the third part, the device was evaluated in managing acute maxillary sinusitis using irrigation, aspiration, and rotating wire. The nasal cavity was inspected using a 0° endoscope. All patients were treated by a single rhinologist.
This part included patients having ARS involving one or more maxillary sinuses, who did not improve under prolonged intravenous (IV) antibiotic treatment combined with nasal and oral decongestants. All patients included were considered candidates for surgical treatment.
Patients with maxillo-ethmoidal blockage of the ostium (Haller cells blocking the OMU, concha bullosa, large uncinate process bulla, or large ethmoidal bulla), those with suspected malignancies, and those with other confounding risk factors (coagulation disorders and abnormal results on blood count) were excluded.
In the third clinical part, the patients underwent sinus lavage with SinuSafe in office settings under local anesthesia. The visual analog scale (VAS) for pain was estimated before, during, immediately after the procedure, 3 hours after the procedure, and the following day. Temperature, blood pressure, and O2 saturation were obtained 3 times per day. Subsequently, the ostia were inspected endoscopically, and the patients were observed for an additional 24 hours.
Statistical analysis was performed using SPSS v25 (IBM Inc). Our outcome was the VAS score and we used repeated measures analysis. A P value <.05 was considered statistically significant.
Results
During the first and second parts of the study, the cannula could access the maxillary ostia bilaterally and the nitinol cable with wire could be successfully inserted into the maxillary sinus. Four maxillary sinuses were cannulated in the first part. These patients underwent ESS surgery subsequently; intraoperatively, the ostium was found to be slightly dilated. In the second part, 8 maxillary sinuses were cannulated and nitinol wire was inserted; irrigation and aspiration revealed thick mucus. Rigid nasal and sinus endoscopes revealed no injury to the nasal cavity and ostial mucosa.
Third part of the trial was performed in 10 patients with maxillary ABRS; 2 of them had acute exacerbations of CRS. The patients had ABRS for 4 to 45 days (mean, 18.1 days) with no response to antibiotic and supportive treatments (amoxicillin with clavulanic acid, 1 gram, thrice daily; intranasal steroid spray, thrice daily; xylometazoline spray, thrice daily; and various analgesics). They were hospitalized at the Hillel Yaffe Medical Center for 2 to 7 days and received IV antibiotics according to the standard protocol in Israel; however, there were no clinical improvements. Two of them received IV antibiotics for <10 days and developed orbital involvement. The others were treated with IV antibiotics for at least 10 days, which resulted in no improvements or worsening of the symptoms.
In this third part, 10 patients (6 females; mean age, 44.2 years; range, 21-69) underwent sinus lavage with SinuSafe. Four had prior ABRS episodes, and odontogenic etiology was suspected in 3 of 4 of them. Three patients presented with bilateral disease; 7 patients had limited single sinus disease; and 5 and 2 had right and left maxillary ABRS, respectively. One patient had simultaneous frontal and maxillary sinusitis. Three of the patients had orbital involvement.
The device enabled rapid, efficient insertion into the acutely occluded sinuses as observed on CT. Drainage was attempted before using the motor, which was unsuccessful. However, the nitinol wire broke the thick mucus, thus, enabling irrigation without any adverse events, which allowed for drainage and obtaining culture samples. Overall, 9 of 10 of them demonstrated remarkable improvements (Table 1, Figure 3) and were discharged the following day following rapid regression of periorbital soft tissue edema in 3 patients and complete regression of the pain. Their VAS score dropped from an average of 8.9 before the procedure to 5 immediately after the procedure, 2.7 three hours after the procedure, and 0.4 the next day (Table 1, Figure 3). Repeated measures analysis demonstrated that these results were statistically significant despite the small sample size (F 18,3 = 22.15, P < .001).
Patients Pain VAS.
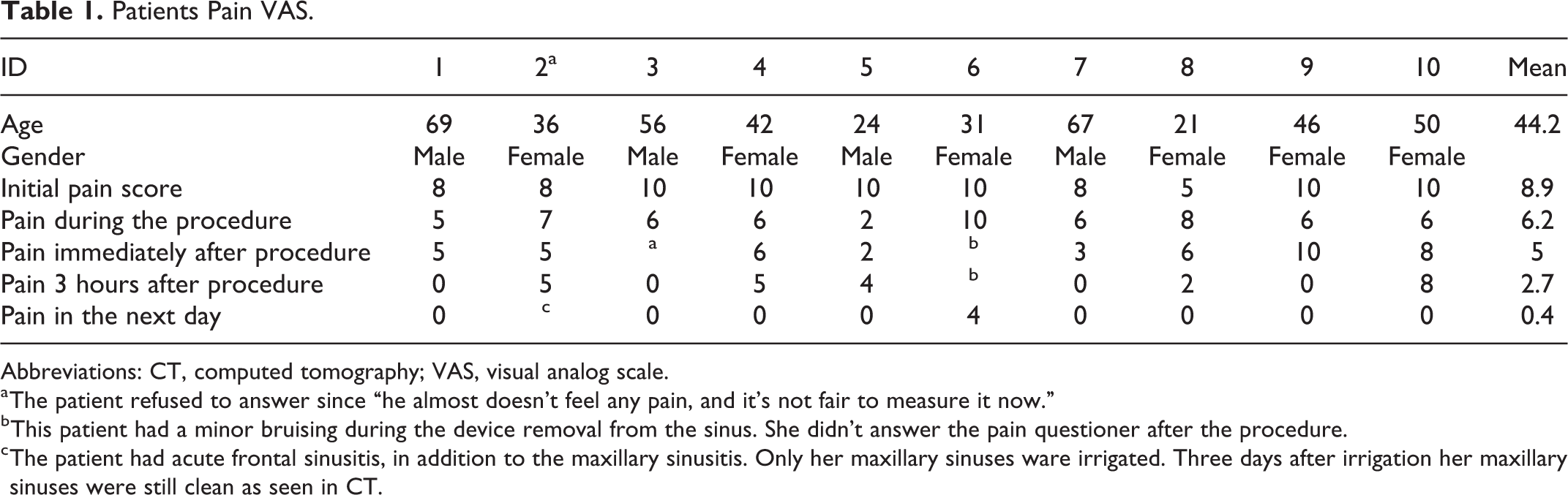
Abbreviations: CT, computed tomography; VAS, visual analog scale.
a The patient refused to answer since “he almost doesn’t feel any pain, and it’s not fair to measure it now.”
b This patient had a minor bruising during the device removal from the sinus. She didn’t answer the pain questioner after the procedure.
c The patient had acute frontal sinusitis, in addition to the maxillary sinusitis. Only her maxillary sinuses ware irrigated. Three days after irrigation her maxillary sinuses were still clean as seen in CT.
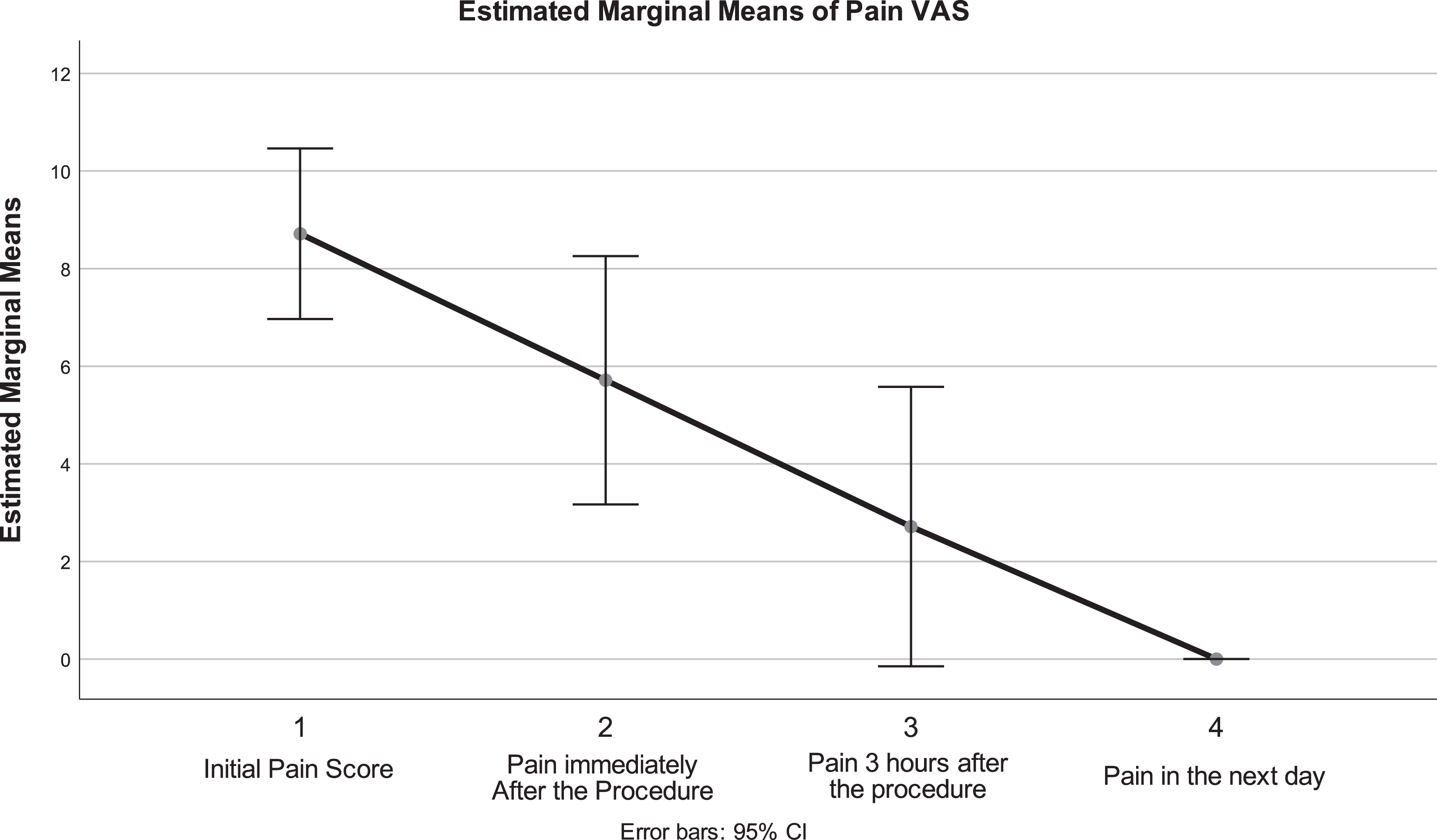
Estimated margin of means of the visual analog scale (VAS) for pain.
One patient who had simultaneous frontal and maxillary sinusitis underwent only maxillary sinus wash. Due to the lack of clinical improvements after additional 72 hours of antibiotic administration, the patient subsequently underwent frontal sinus ESS. Furthermore, X-ray performed 4 days after SinuSafe procedure demonstrated clean maxillary sinuses with persistent frontal disease. An additional patient underwent subsequent CT scan 59 days following the procedure, for an unrelated reason, showed no remnants in the maxillary sinus (Figure 4).
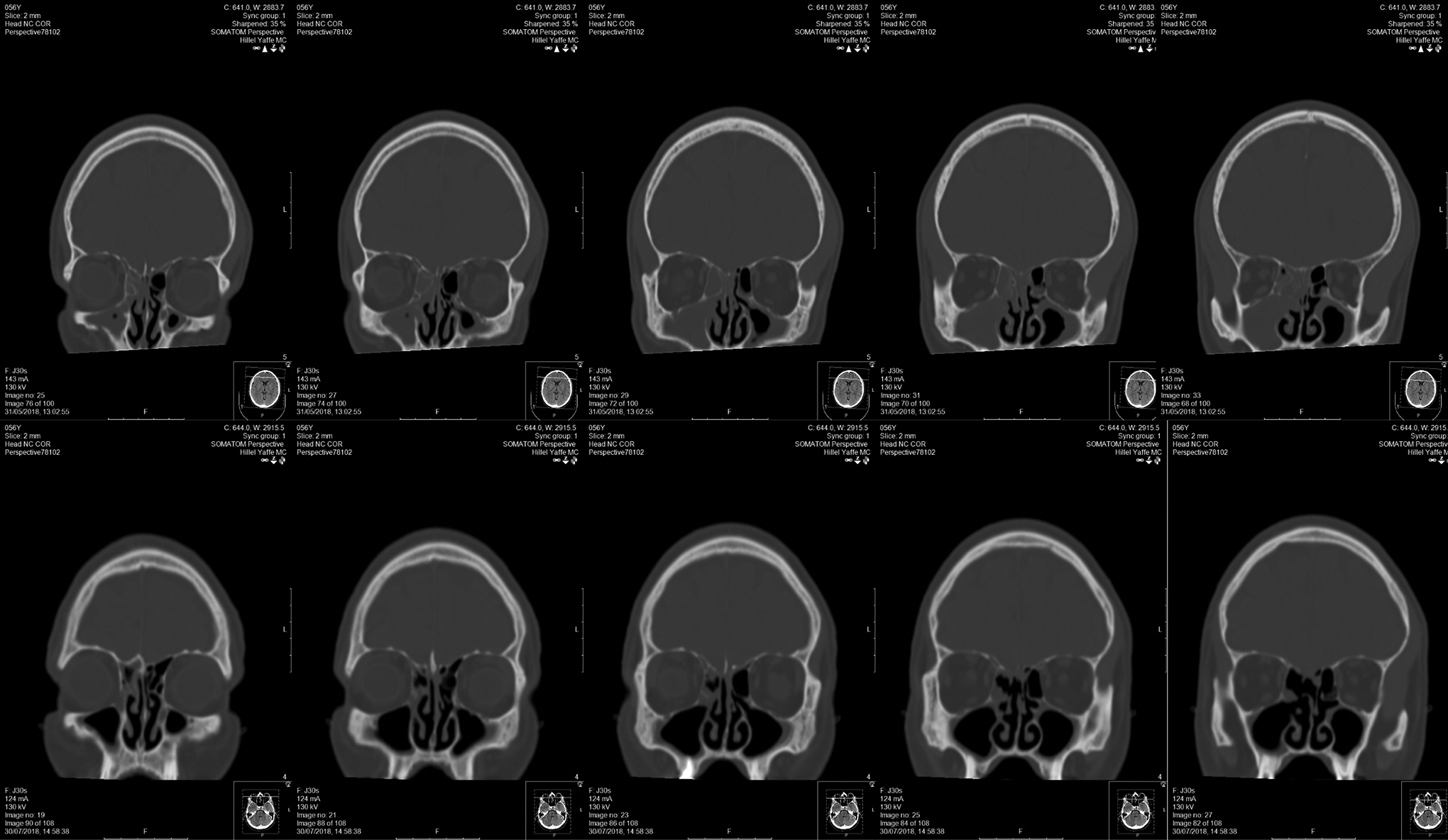
An additional patient underwent the procedure, a computed tomography (CT) scan before, and an unrelated CT scan 59 days later. Top row—Series of coronal images before the procedure, bottom row—series of coronal images after the procedure.
Overall, no adverse event was noted except discomfort during the procedure (Table 1).
Discussion
Early in the 20th century, several attempts were made to explore the contents of the sinuses. Mikulicz-Radecki suggested reaching the maxillary antrum intranasally through the middle meatus. Krause modified this approach by utilizing a drainage tube for repeated irrigations. 12 In the mid-20th century, sinus lavage with or without topical antibiotics and the Proetz maneuver (type of nasal lavage) were standards of care. Multiple reports have demonstrated that sinus lavages decreased the need for sinus surgeries. 13 -29 The importance of sinus lavage in nonresponders was considered obvious as most reports from that period did not describe its benefits empirically but rather focused on its role in various contexts or comparing the different techniques of sinus puncturing. 15,30 -36 However, patient selection and quantification of data were poor, which limited further data analysis. 30,31,37,38
Some studies, however, observed that repeated irrigation after antibiotic treatment failure could prevent sinus surgeries in patients with acute episodes. These studies (Table 2) included up to 523 patients and demonstrated significant positive effects of repeated lavage; no more than 46% of patients and as few as 0 of 202 cases 33 required surgery. 32,33,39 -44
Review of the Literature on Repeated Sinus Irrigations.
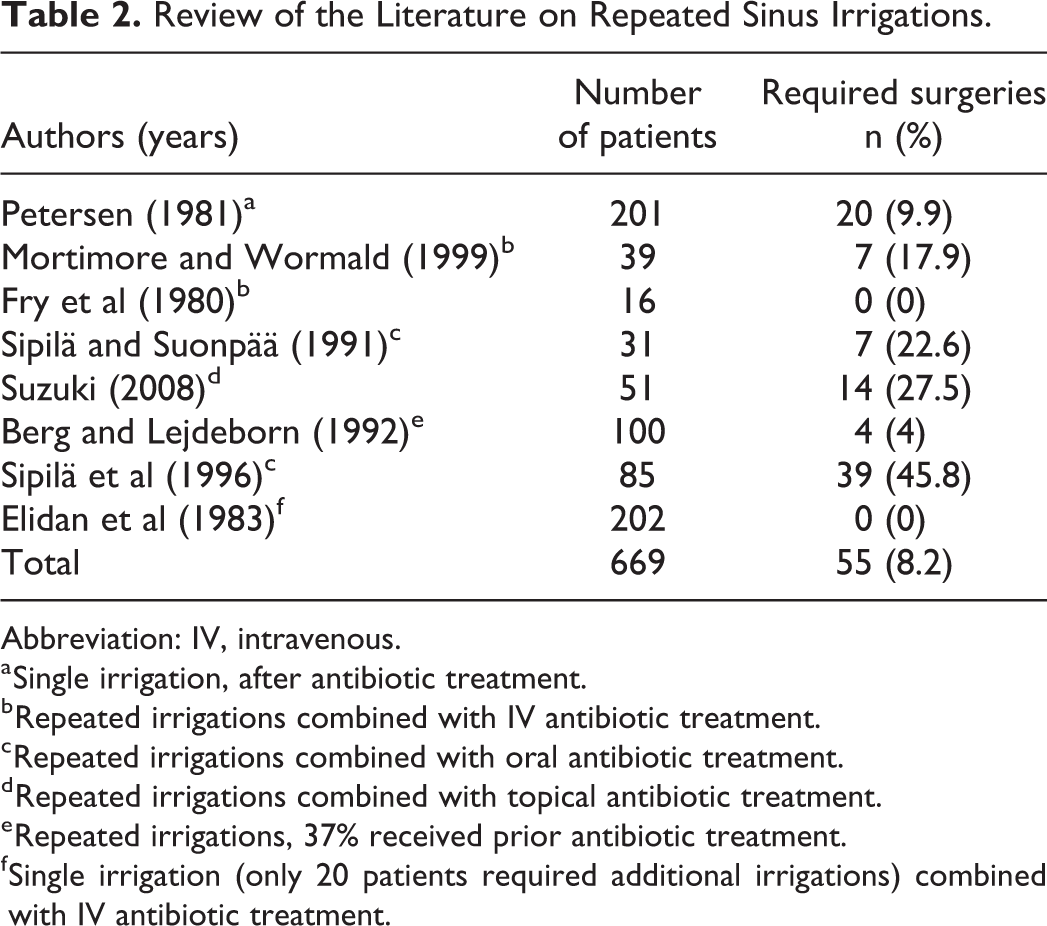
Abbreviation: IV, intravenous.
a Single irrigation, after antibiotic treatment.
b Repeated irrigations combined with IV antibiotic treatment.
c Repeated irrigations combined with oral antibiotic treatment.
d Repeated irrigations combined with topical antibiotic treatment.
e Repeated irrigations, 37% received prior antibiotic treatment.
f Single irrigation (only 20 patients required additional irrigations) combined with IV antibiotic treatment.
Subsequently, clinical trials reported a slight advantage of sinus irrigation over the traditional antibiotics without significant benefits over the newer generations of antibiotics 45 -47 and surgical techniques; therefore, the use of sinus trephination waned and was reserved for identification of bacteria and bacteria-specific antibiotics. 7,48 Furthermore, repeated puncturing and trephination included risks, such as bleeding, contamination, pain, swelling of the cheek, and in rare cases, puncturing of the orbit or vasovagal responses. 49
Antibiotic resistance continues to be an issue. 50 In 2005 to 2012, only 4 applications were approved for new antibiotics versus 19 approvals in 1980 to 1984 in the United States. Four reviews have demonstrated that antibiotics no longer shorten the disease duration as they did in the past. 6 -8,51 Guidelines recommend avoiding antibiotics for most respiratory infections initially since they are usually viral and self-limited. 3
The results of the current trial are significantly better than most previous results, except those of Elidan et al 33 who treated patients with IV antibiotics for additional 5 days following irrigation. In the current trial, an almost perfect effect was achieved in the maxillary sinuses after only one episode of irrigation; only one patient did not improve because of concomitant frontal sinusitis. In contrast, repeated irrigations were required in previous trials with subsequent mean success rate of 86%.
Similar to the current device, balloon sinuplasty is well established for recurrent ARS as it relies on ostial expansion to relieve the sinus and allow for suctioning and drainage. However, the need for ostial expansion is yet to be proved because recurrence is uncommon in ABRS. Furthermore, the current trial demonstrates promising, although preliminary, results of treating ARS without significant ostial dilation and disruption of the normal anatomy.
There may be several explanations for the current results. One possible explanation is the very small sample size, which limits the generalization of these results. Another explanation is that multiple irrigations were not required in all patients as was observed in the study by Elidan et al. 33 Another explanation might be patient selection. In the current trial, the patients had either acute disease for a long time or severe acute exacerbations, which made improvements more noticeable. In other trials, some patients might have had other mucosal conditions, such as polyposis or less acute disease and different bacteria and lower immune response. An additional explanation might be that irrigation enabled aeration of the sinus mucosa and that the treatment improved the acidity and oxygenation required to restore the antibiotic action. In some previous trials, the patients did not receive combined antibiotics and irrigation. Additionally, IV antibiotics in our trial might have had better penetration than those in previous trials where oral antibiotics were administered post- rather than preirrigation. 45 -47 In another trial, 52 repeated irrigations proved successful even without the need for antibiotics.
Another explanation might involve the adjuvant use of intranasal corticosteroids (INCS). Since INCS were introduced for allergic rhinitis in 1973, 53 they have been used in other conditions, including ARS. Meta-analyses of randomized clinical trials indicate a modest, but significant, effect of INCS in ARS. 54,55 The conventional theory is that steroids reduce inflammation and mucus secretion and might prevent ostial occlusion, thus, restoring and preserving the mucociliary clearance. The drawbacks of INCS in ARS include limited penetration into the sinus cavities and the inability of steroids in stopping inflammation during an active infection with high bacterial load. None of the reviewed trials had reported on INCS.
Compared to traditional irrigation via the sinus wall, SinuSafe cannula rotates within the sinus ostium, which gently and nontraumatically dilates it by compressing the ostial mucosa without affecting the ostial bone; this was demonstrated in 4 patients who underwent the procedure in an OR. Ostial dilation might lead to better aeration and mucociliary clearance of the sinuses. Sufficient mucociliary clearance is essential as an antibacterial mechanism and for the evacuation of inflammatory factors and bacteria-sensing molecules from the cavity, which reduces mucosal inflammation and bacterial virulence. Better sinus dilation and “sinus aeration” might be even more critical in cases of prolonged acute disease and anaerobic bacteria. This might be due to the higher efficacy of SinuSafe in mucous removal due to the rotating wire mechanism, which breaks the mucin and enables suctioning. Better mucus removal could also mean better bacteria-to-leukocyte/antibiotic ratio and faster resolution. Additional larger trials are required to understand the precise mechanisms of action completely. As with any sinus procedure, long-term follow-up is needed to determine the durability of treatment.
Finally, the current results might rather be due to the combined effects of IV antibiotics, sinus lavage with SinuSafe, and INCS and intranasal decongestants. The lavage allowed the drugs to reach the freshly aerated sinus and restore the mucociliary clearance, while IV antibiotics reduced the bacterial bioburden.
Acute rhinosinusitis is commonly a self-limiting disease that does not require interventions. Guidelines suggest that watchful waiting and antibiotics in the first 14 days should be sufficient in approximately 70% to 90% of patients. 3 Studies regarding the antibiotic and surgical interventions in patients with acute and sub-ARS who were nonresponsive to the initial antibiotics after 14 days are lacking. 3,56 The literature on disease progression from acute to subacute and subacute to chronic disease is mostly theoretical or retrospective, controversial, and missing. 3,56,57 SinuSafe might be better in managing a substantial number of patients nonresponsive to medical interventions and as a direct investigation. Further studies are required to evaluate the use of concomitant drugs and treatment protocols, and identify patients who will benefit from SinuSafe.
Conclusions
SinuSafe is a novel device that could permit safe cannulation of the maxillary sinus, reduces the viscosity of sinus secretions, and improves the efficiency of sinus lavage. Patients treated with SinuSafe in this preliminary study showed no adverse events and good clinical response. These results mirror the literature, with less traumatic consequences. The study was limited due to the very small sample size, hindering the result’s impact. Additionally, routine imaging following the procedure could have been used to measure the pre-, and post-procedural disease burden objectively but was not clinically justified. Further research is warranted to determine whether the device could fill the treatment gap between oral antibiotics and surgeries and evaluate its potential in combination with the current medical conventions.
Footnotes
Acknowledgments
The authors would like to thank Mrs Ariela Ehrlich MLS, Medical Information Specialist and Mrs Gal Noulman Russek for their assistance in editing the manuscript.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: I.B. is a board member and shareholder of SinuSafe® Medical Ltd. I.B. suggested the study but precluded himself from participating in the study execution, analysis, and writing. H.L. is an advisor for SinuSafe® Medical Ltd and joined after the study was concluded and analyzed, to help polish the English writing and the introduction and historic review part of the study. The devices were donated to Hillel Yaffe Medical Center as per the ethical board requirements and the Israeli Ministry of Health.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.