
Abstract
Chondrosarcoma of the thyroid cartilage is a sporadic disease with nonspecific clinical presentation. Smooth swelling of the supraglottic area should arouse suspicion of possible pathology. In addition to laryngoceles, which usually do not have a significant impact, otolaryngologists should consider chondrosarcoma of the thyroid cartilage and indicate computed tomography (CT). Late diagnosis leads to worse prognosis, particularly worse voice after more extensive surgery, need for tracheostomy, and worse survival from higher degree chondrosarcomas.
A 63-year-old male was referred for otolaryngology examination due to hoarseness lasting for 5 months. The patient did not complain of respiratory problems. He had no history of smoking, laryngeal surgery, or recent intubation. Endoscopic laryngeal examination identified smooth swelling of the right false vocal fold (Figure 1). There was no evidence of pathological vascularization on narrow-band imaging. The movement of the vocal folds was normal. Computed tomography revealed a tumor mass in the right thyroid cartilage, causing its destruction (Figure 2).
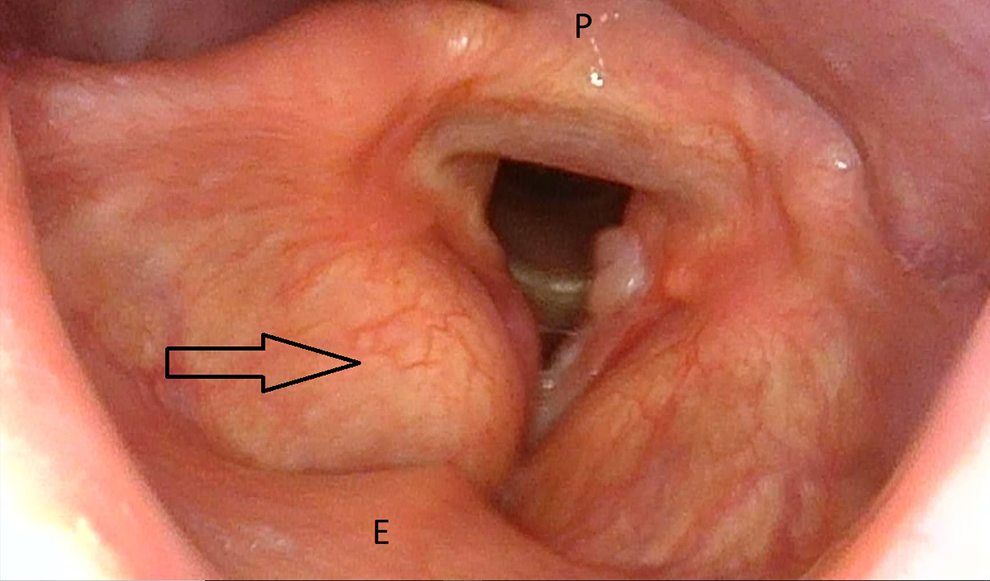
Preoperative flexible endoscopy of the larynx showing smooth swelling of the right false vocal fold (arrow). E indicates epiglottis; P, posterior pharyngeal wall.

Axial CT showing a tumor mass in the right thyroid cartilage, causing its destruction. CT indicates computed tomography.
The patient underwent diagnostic microlaryngoscopy, which revealed a soft tumor under the outer lamina of the thyroid cartilage of the right false vocal fold. Partial resection was performed to determine the specific type of tumor. Histopathological examination confirmed grade I to II laryngeal chondrosarcoma.
Complete surgical removal of the tumor was indicated. Partial resection (anterior 2/3) of the right thyroid cartilage was performed from an external approach (Figure 3). To secure the airway during the postoperative period, a temporary tracheostomy was performed. The surgery provided complete tumor removal without any peri- or postoperative complications. Final histopathological examination confirmed grade II laryngeal chondrosarcoma. Follow-up with no additional oncology therapy was chosen by the multidisciplinary team. Voice quality did not worsen after surgery compared to the preoperative quality. The patient has been followed for 4 years, with no evidence of recurrence.
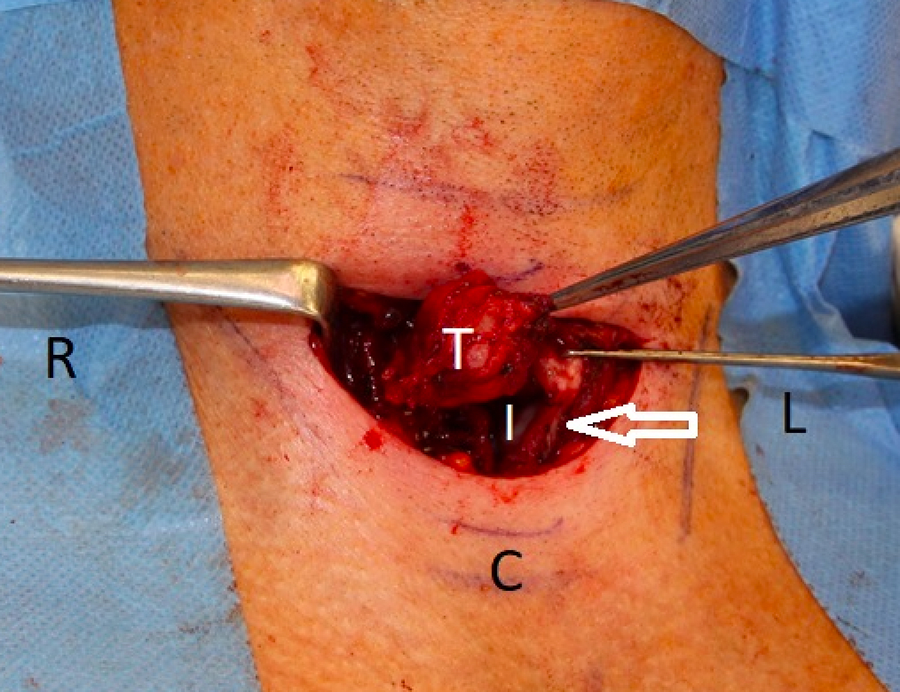
Partial resection of the right thyroid cartilage with the tumor via an external approach. The arrow indicates the thyroid cartilage. C indicates cricoid; I, inner part of the larynx; L, left; R, right; S, superior; T, tumor.
Discussion
Primary chondrosarcoma of the thyroid cartilage is an infrequent diagnosis, representing 20% of all laryngeal chondrosarcomas, which comprise 1% of laryngeal malignancies. 1,2 Chondrosarcoma typically occurs in patients between the fifth and sixth decades, and the incidence is 3 times higher in males than in females. 3 -9 The exact etiopathogenesis of chondrosarcoma in the thyroid cartilage remains unclear. 10 Disordered ossification is most often described as the possible etiology. 11 -14 There has also been debate over whether chondroma is a benign precursor lesion of chondrosarcoma. 15 -17
Diagnosis of chondrosarcomas can be challenging given the slow rate of growth and nonspecific symptoms at presentation, such as hoarseness, dyspnea, airway obstruction, dysphagia, and painless neck mass. 3 -9 The fundamental diagnostic step is endoscopic examination of the larynx and imaging. Smooth asymmetry of the supraglottic area should arouse suspicion of laryngocele, chondroma, chondrosarcoma, and other less frequent pathologies. Chondroma and chondrosarcoma have similar signs on CT. Typical findings include a hypodense, well-circumscribed mass containing fine, punctuate stippled calcifications to coarse “popcorn” calcifications. 3 -9 Histopathological examination is mandatory to distinguish between chondroma and chondrosarcoma. Microscopically, chondrosarcoma presents as several cells with large, irregular, and multiple nuclei with increased mitotic activity. 18
Surgery is the treatment of choice, and an external or endoscopic approach is possible. 2,19,20 Chondrosarcoma is considered less sensitive or insensitive to radiotherapy or chemotherapy. 3 -9,21 Moreover, both modalities have no significant effect on eliminating subclinical metastasis postoperatively. 10,22 Recurrence of chondrosarcoma is common, with recurrence rates of 18% to 40%, but the long-time prognosis is good, with a 10-year survival of 95%. 3 -9
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by MH CZ-DRO-FNOs/2021.