
Abstract

A 54-year-old African American woman presented to our clinic with a 2-year history of progressive hoarseness and dyspnea. She had a documented history of sarcoid for the past 25 years. She noted breathiness in her speaking voice, vocal fatigue, voice breaks, tickle in the throat, weak voice, frequent throat clearing, and coughing. Her symptoms were worse in the evening. She had had mostly skin involvement of sarcoid lesions including her nose, back, cheeks, and forearms. She had been on Prednisone intermittently for years. She had also taken methotrexate and hydroxychloroquine without benefit.
She was noted to have sarcoid of the supraglottic airway appearing as severe thickening of the entire epiglottis and arytenoid mucosa scarred together with a narrowed inlet to the vocal folds (Figure 1A and B). The true vocal folds were bilaterally mobile with good abduction and adduction. Previously, tracheotomy had been recommended. However, the patient had declined. She was started on infliximab and adalimumab without change in her upper airway symptoms. She was consented for surgery with the possibility of needing tracheotomy.
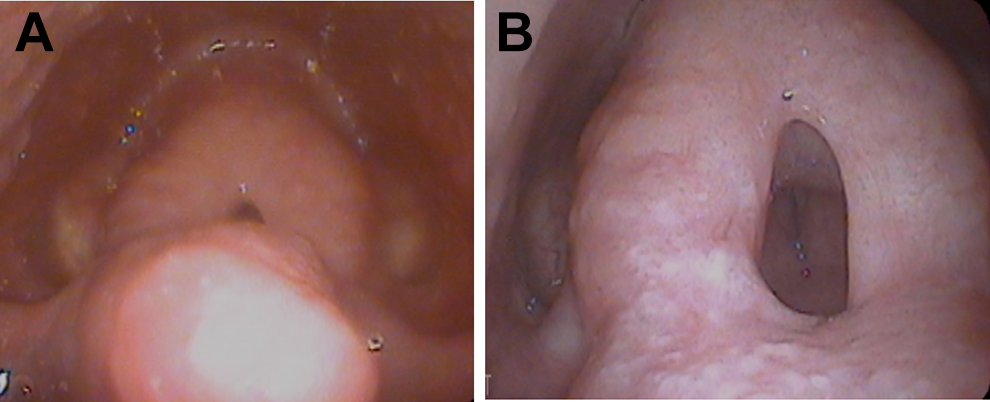
(A) Preoperative view of laryngeal sarcoidosis. (B) Preoperative view of laryngeal sarcoidosis.
She underwent microsuspension direct laryngoscopy with CO2 laser supraglottoplasty of obstructing sarcoid, and steroid injection. Postoperatively, she was breathing well on room air without stridor (Figure 2). She was discharged the following day. She had been breathing well in the months following the surgery. Pathology of the excised laryngeal lesion was reported as “chronic granulomatous inflammation is present, characterized by multiple non-necrotizing granulomas.”

Postoperative laryngologic view.
Discussion
Sarcoidosis is an idiopathic, inflammatory, granulomatous disorder compromised of epithelioid and multinucleated giant cells with little necrosis. 1 Most common sites of involvement include the lungs, hilar and mediastinal lymph nodes, liver, eyes, skin, bones, and nervous system. Laryngeal sarcoid is very rare. The estimated involvement of the larynx is between 1% and 5%. 2
Sarcoidosis of the larynx tends to develop in the supraglottic region. The most common area is the epiglottis. Supraglottic sarcoid also develops in the arytenoids, aryepiglottic folds, and false vocal folds. Severe airway obstruction is possible. The major impairment of the supraglottis probably occurs due to the amount of lymphatic vessels in that region, which are stretched by replacing the architecture by sarcoid deposits. 3 The most common complaints of laryngeal sarcoidosis are hoarseness, dyspnea, dysphagia, chronic cough, and obstructive sleep apnea. 4 Severe stridor and airway obstruction, needing tracheotomy, have been described. 5
Patients with laryngeal sarcoidosis do not necessarily show the systemic form. In a review by Benjamin et al, 6 of 5 patients with laryngeal lesions, only one had generalized disease. In other reports, 4 of 13 patients having laryngeal lesions, 7 showed involvement of other organs. In our case, sarcoidosis of the larynx was found in all areas mentioned causing supraglottic obstruction and airway compromise, and she had skin lesions. Because of the risk of airway symptoms, patients with laryngeal sarcoidosis should be seen regularly and be informed about complications and worrisome symptoms. Treatments for laryngeal sarcoid include systemic and intralesional corticosteroids, surgical excision, and radiation. Ten percent of patients with laryngeal sarcoidosis show spontaneous remission. 7
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.